Public Health Injury Surveillance and Prevention Program 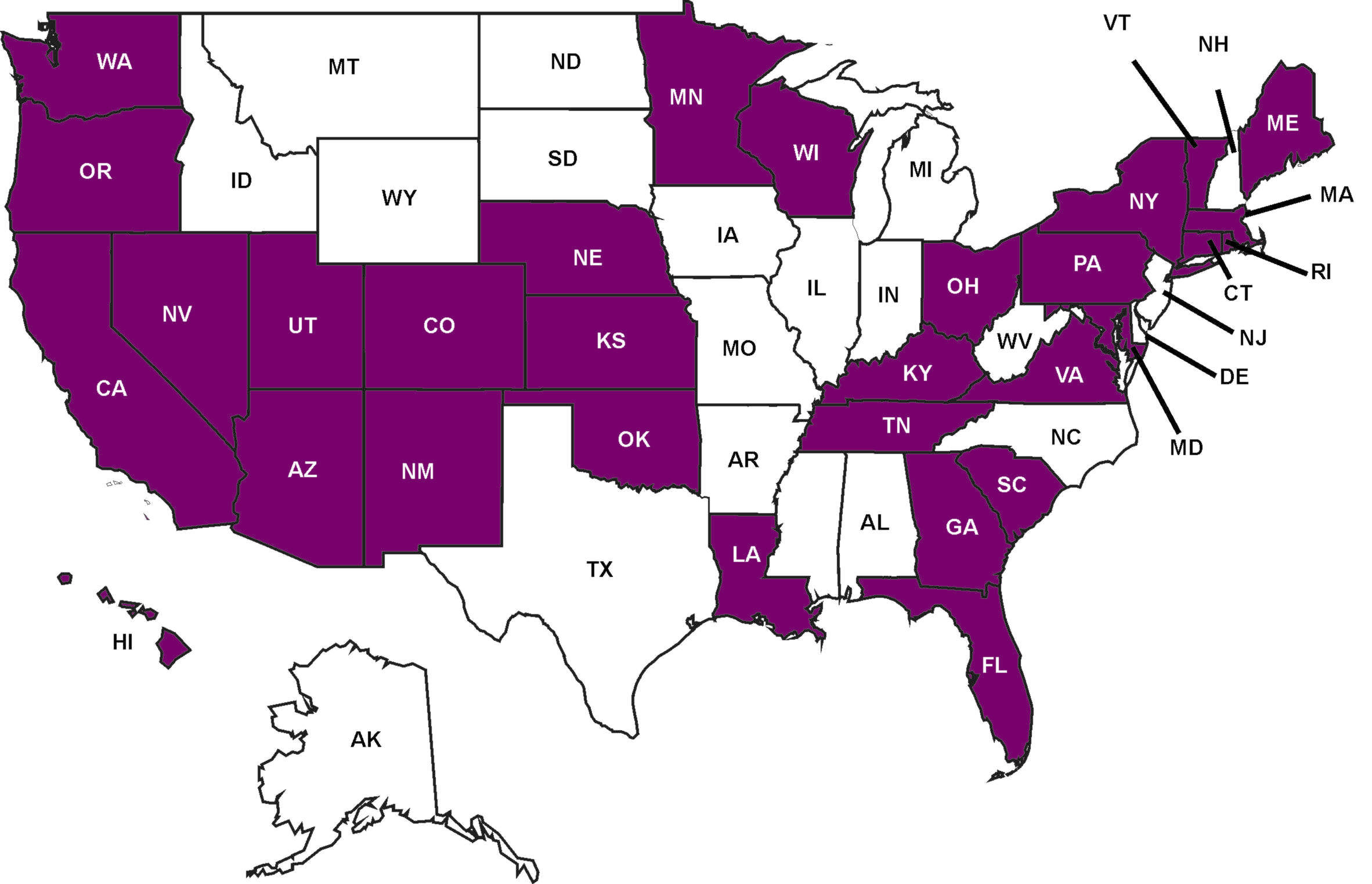 About the Program About the Program
Injury is a leading cause of death and disability throughout the United States. Due to varying weather, geography, and populations, injury problems differ from state to state. CDC addresses these differences through its Public Health Injury Surveillance and Prevention (PHISP) Program (formally known as the Core State Injury Program). This program funds “core” capacity building and surveillance activities to prevent and control injuries—including traumatic brain injury (TBI).
The PHISP Program has three primary objectives:
-
Build a solid infrastructure for injury prevention and control;
-
Collect, analyze, and use injury data; and
-
Implement and evaluate interventions.
Funding
CDC funds the following four components under the PHISP Program, with all states funded for Part A, and certain noted states receiving funding for Parts B, C and D:
-
Part A—Integrated Core Injury Prevention and Control (ICIPC) Program. Approximate funding per award: $120,000. All states funded under the PHISP Program receive this funding.
-
Part B—Traumatic Brain Injury Extended Surveillance Program. Approximate funding per award: $100,000. Four states received this funding in 2005: Colorado, Minnesota, Oklahoma, and Utah.
-
Part C—Traumatic Brain Injury Emergency Department Surveillance Program. Approximate funding per award: $125,000. Two states receive this funding in 2005: Minnesota and South Carolina.
-
Part D—Traumatic Brain Injury Service Linkage Program. Approximate funding per award: $50,000. Five states received this funding in 2005: Colorado, Minnesota, Oklahoma, Rhode Island, and South Carolina.
Program History and Accomplishments
In 1997, CDC funded four states to establish state injury programs; three more states were funded in 1999. By 2000, CDC-funded states totaled 24.
Currently, CDC funds 30 states to conduct basic surveillance, or Part A of the PHISP Program. CDC also funds four states (Colorado, Minnesota, Oklahoma, and Utah) to abstract supplemental data on TBI from medical records (TBIES). These data include information about alcohol use, severity of acute injury, and use of protective equipment such as automobile safety belts and child safety seats. Additionally, Minnesota and South Carolina are funded to conduct exploratory, emergency department-based surveillance to identify cases of
mild TBI (TBIED). Five states, (Colorado, Minnesota, Oklahoma, Rhode Island, and South Carolina), are also funded to link individuals with services in their community.
The ICIPC component of the PHISP Program helps states build capacity and strengthen essential infrastructure. Most CDC-funded states use advisory committees to develop and prioritize injury plans. CDC encourages states to build coalitions with partners from academic, nonprofit, private, local government, and professional organizations. As a result, injury is widely recognized as a critical public health problem.
Since the program began, significant accomplishments have occurred at the state level:
-
Oregon’s Health Department assisted policy makers by providing comprehensive injury data for 54 injury-related bills. Legislation was introduced in transportation safety, firearm safety, consumer product safety, child maltreatment, and domestic violence.
-
Findings from the Injury Surveillance Program in Massachusetts supported testimony at public hearings to require reporting of data for patients discharged from the emergency department. The Uniform Hospital Emergency Department Discharge System has since been established in this state.
-
In Kansas, the injury prevention staff partnered with the Kansas Highway Patrol, the Kansas Child Death Review Board in the Attorney General’s Office, and the Suicide Prevention Steering Committee to produce two public service announcements about suicide prevention.
-
Colorado’s injury prevention staff linked two data systems to better review helmet use, seatbelt use, elderly drivers, alcohol-impaired driving, and the impact of a graduated licensing law.
-
Suicide attempts were made a reportable condition in Oklahoma, and the Oklahoma legislature created the Youth Suicide Prevention Act and Youth Suicide Prevention Council.
Program Improvements
The program underwent notable changes in 2005:
-
Increased focus on expanding capacity by securing community resources, thereby sustaining programs and enhancing a state’s ability to implement injury prevention plans.
-
Increased focus on systematic data collection, analysis, and use.
-
Integration of TBI surveillance components into the ICIPC program to create the overarching PHISP Program.
|
|