|
 |

|
Print  Download Reader
Download Reader 
|
|
|
Print Download Reader
Testimony
Wednesday, May 3, 2006 Chairman Johnson, Representative Stark, distinguished members of the Subcommittee, thank you for the opportunity to update you on the new Medicare prescription drug coverage, and especially the steps we are taking to maximize enrollment as we enter the final days of open enrollment period. I also want to address the steps that we are taking concerning preparations for 2007 to make the prescription drug benefit program even better. I want to take this opportunity to thank those of you who have participated in CMS' enrollment events throughout the country. I appreciate your interest in this topic, but more importantly I am very grateful for your personal assistance and that of many of your colleagues in driving the awareness of and enrollment in Part D. Members of Congress have been an important part of this massive grassroots education effort and I am very hopeful that this partnership we have created can continue as we begin to drive greater awareness and use of the prevention benefits which the Congress included in the Medicare Modernization Act (MMA). More than 8 million beneficiaries have new individual prescription drug coverage since the program began and more than 93.8 million prescriptions were filled for these beneficiaries with drug coverage during March -- averaging 3 million prescriptions filled per day. The vast majority of beneficiaries are using their coverage effectively and each week hundreds of thousands of beneficiaries are enrolling in the new program. CMS has already exceeded the enrollment target with more than 30 million beneficiaries with drug coverage through Part D or a former employer as of April 18, 2006. In addition, almost 6 million Medicare beneficiaries get drug coverage from other sources with prescription drug coverage such as the Department of Veterans Affairs equal to Medicare. This brings the total to approximately 36 million Medicare beneficiaries who are now receiving prescription drug coverage. According to data collected through beneficiary satisfaction surveys, 84 percent of seniors enrolled in the Medicare prescription drug program are satisfied with their coverage and 52 percent say they are enjoying significant cost savings.1 Further, a U.S. Chamber of Commerce study shows that 85 percent of enrollees say their plan covers the medicine they need and a study conducted by the Kaiser Family Foundation reveals that 82 percent of enrollees who have filled a prescription under the benefit reported having no problems.2 CMS worked with the plans, pharmacists, States, and hundreds of other partners leading up to the start of the drug benefit to educate beneficiaries and their caregivers about the their choices and to help people understand how to make decisions based on cost, coverage, convenience, and peace of mind. There are still twelve more days to enroll before the May 15, 2006 enrollment deadline for the year, and we need to help beneficiaries get the savings and security of prescription drug coverage now. We have put into place many outreach resources to get the information to beneficiaries so they can enroll. To minimize an anticipated last minute rush to enroll, CMS is making a monumental effort to enroll beneficiaries as soon as possible. In the last month, there have been more than 1,880 events per week across the country to provide beneficiaries with personalized help so they understand the prescription drug coverage options available to them and so they can enroll in a plan. I know that you and other Members of Congress have been very helpful with events in your district as well. I have personally contacted many of the high enrollment plans to express my concern that they put adequate resources into their call centers. However, we know there will be a large number of enrollments as the May deadline approaches. While this may lead to longer wait times on both our call lines and plan sponsor lines, we have worked with the plans and we will make every effort to enroll everyone who wants to enroll. But to minimize problems, you should encourage your constituents to act now. Millions of seniors and people with disabilities are already using this benefit to save money, stay healthy, and gain peace of mind. This includes several million individuals who, because they also qualify for Medicaid, or the low-income subsidy (LIS), will have very low or no premiums deductibles and cost sharing. CMS estimates that almost 270 million prescriptions were filled during the first three months of 2006 for all Medicare beneficiaries with drug coverage. Because of strong competition in the prescription drug marketplace, there has been slower growth in prescription drug inflation in recent years, due in part to increasing generic drug availability. Also, the proliferation of tiered co-payment drug plans and use of formularies have caused the use of generic drugs to increase and further slow drug spending growth. Consequently, the new Medicare prescription drug coverage is costing much less for beneficiaries, taxpayers, and the States than anticipated. Beneficiaries are choosing plans that best meet their needs, leading to coverage that serves them well and costs less for them and for taxpayers. Enrollment data reveal that the vast majority of beneficiaries are choosing plans that offer benefits other than the standard option as defined in the law. They are choosing plans that have low premiums, no deductibles, fixed copays, and coverage in the gap. In fact, only 16 percent of prescription drug plan (PDP) enrollees chose the standard, statutory option and only 5 percent of Medicare Advantage prescription drug plan (MA-PD) enrollees chose the standard option. Beneficiaries are also often choosing plans with access to a broad range of drugs. Beneficiaries eligible for the low-income subsidy have a very comprehensive benefit, with no coverage gap and usually no deductible. CMS anticipates that plan sponsors will consider current enrollment statistics when submitting their bids for 2007, and will limit their plan options accordingly. CMS' expectations for plan bids are outlined in the 2007 Call Letter, which I will discuss shortly. We are hearing reports from our partners about the cost savings people with Medicare are experiencing. It is estimated that the Medicare drug benefit will pay on average about half of total drug spending in 2006 for seniors who are not eligible for extra help. The beneficiaries who qualify for the low-income subsidy receive substantially greater assistance, with a benefit that will cover on average over 95 percent of their drug costs. CMS and Our Partners have Raised Awareness Nationwide Before implementation of the drug benefit, CMS provided most information directly to beneficiaries using the traditional tools, including the Medicare & You Handbook, 1-800-MEDICARE, and www.medicare.gov. However, with the passage of the MMA, CMS saw the need to improve our existing tools and to develop new strategies in order to reach a wider audience and to target specific hard- to -reach populations, including rural areas and minority communities. In addition to print, radio and television advertisements, CMS has a multi-pronged approach to raise awareness and assist beneficiaries and their caregivers in making decisions about prescription drug plans. CMS knew from the outset that it was essential to provide beneficiaries with more hands -on assistance than was available in our traditional educational materials through outreach events and one-on-one training. This effort would have to be both a high-touch and high-tech outreach campaign, with high-tech resources like the personalized Plan Finder web tool for use by our partners and our beneficiaries, as well as high-touch efforts involving one-on-one personal contacts using an intricate web of grassroots partners collaborating and leveraging each other for the maximum benefit of people with Medicare. In addition, rather than just reaching beneficiaries, CMS cast a wider net to reach caregivers, family and friends of beneficiaries. During 2004, CMS began reaching out to develop partnerships, and now the network is incredibly diverse and committed. For several months, we held training sessions throughout the country to educate our partners about the benefit structure and the enrollment tools so they could help raise awareness, educate, and enroll beneficiaries. CMS provided special training for social service coordinators to help them counsel low-income seniors. CMS relied heavily on our partner organizations to work with beneficiaries on a one-on-one basis. President Bush, Secretary Leavitt, and I, along with CMS' regional office staff, have traveled over 500,000 miles across the country in a mobile office bus to form grassroots partnerships that help people with Medicare make an informed decision about prescription drug coverage. About 70 percent of these mobile office stops have taken place in rural communities throughout the country. Many Members of Congress have served as honorary chairs for these events and we appreciate their involvement in forging over 240 grassroots community and statewide networks, each led by a community partner. The mobile office reached rural areas across the country to complement our dedicated funding for outreach to rural areas. Since January 1, 2006, 269 events have involved the participation of an elected official. We appreciate your participation in outreach and we welcome your continued involvement in activities to reach beneficiaries. We have continued to work harder than ever to help beneficiaries and their loved ones learn about their drug coverage. Since January, CMS and its partners have hosted over 22,000 events. Our partner organizations are also providing personalized counseling by request to help beneficiaries enroll in a plan that best meets their needs. CMS worked with the Social Security Administration and various organizations to provide training and conduct outreach to beneficiaries who may qualify for low-income assistance. In addition, we forged partnerships with other federal agencies, which have helped to disseminate information to beneficiaries, especially to those who might qualify for the low-income subsidy. Also, CMS regional offices along with State Health Insurance Assistance Programs (SHIPs), senior advocacy organizations, and agencies on aging have held thousands of information and enrollment events. In fact, CMS has more than doubled its funding to SHIPs since 2003, recognizing the importance of SHIP assistance to beneficiaries. In 2004, CMS provided more than $21 million and increased that to more than $31 million in 2005. The funding level will remain high, even after the initial enrollment period for prescription drug coverage ends, to ensure that SHIP counselors will continue to play an important role in educating beneficiaries about the drug benefit and their plan options in the months ahead. We recognized that to achieve the promise of the MMA we would need to reach all segments of the Medicare population, especially underserved populations and those with language and other cultural barriers. To target these hard to reach populations, including minority, low-income, limited English-speaking, homebound, and rural populations, CMS has a contract with the National Association of Area Agencies on Aging. Strategies included contracting with Aging Network community-based organizations and nine National Aging Organizations with local affiliates to conduct outreach to low-income populations. Thus, we developed specialized campaigns for the African American, Hispanic, American Indians, and Asian American Pacific Islander communities, utilizing new partnerships, creating materials in other languages, and doing specialized paid media campaigns. In summing up a new set of outreach initiatives for African-American beneficiaries, Dr. Sandra Gadson, president of the National Medical Association, has described the importance of this targeted outreach to specific populations such as African American beneficiaries. "If we think we have a health disparity crisis in the African American community today, imagine if we do not succeed in enrolling the most needy of our eligible seniors and people with disabilities." She noted that many of the organizations she was working with had not supported the law, but that it was clearly time to put politics aside in helping people take advantage of the new coverage�coverage that for low income seniors, as Jim Firman, of the National Council on Aging has said, is the most important new health care benefit in 40 years. These extensive, grassroots-level partnerships are truly unprecedented for the Medicare program. We are reaching out to people with Medicare, many people, all over the country �"where they live, work, play, and pray." It has completely changed awareness about the drug benefit, and has helped millions make a decision about Medicare coverage already. It has helped personalize Medicare in a way that we could never do from our national offices. And I believe this will be a fundamental and lasting change in the way that Medicare works. This has been a very exciting time for CMS as we now have many new important relationships which we will continue to nurture for future outreach and education efforts aimed at continuous improvement in the quality of health of the Medicare population. In addition to events around the country, we have worked to enhance our traditional methods of outreach and education. For instance, CMS treats the Medicare & You 2006 handbook, which is mailed to all 42 million beneficiaries and includes detailed information about the new prescription drug coverage, as a continuous quality improvement project. Every year, in an effort to make the handbook a valuable and understandable beneficiary resource that is straightforward and easy to read, CMS conducts consumer testing of the draft handbook at two separate stages. Additional testing is sometimes done for specific sections. CMS also solicits input from our partners, including Members of Congress. CMS Prioritizes Customer Service to Our Beneficiaries and Our Partners CMS has handled more than 22 million calls between November 15, 2005 and April 24, 2006, and the Agency takes great care in answering these calls as promptly as possible and providing accurate, useful information to callers. Because of the great interest in the new drug benefit, call wait times have been longer than we would like at times. CMS has worked diligently to improve the wait times caused in part by data translation problems to ensure accurate information is available in a timely manner to those seeking assistance. As shown in Figure 1, on average, callers have experienced wait times of less than two minutes from January to mid-April, with longer waits sometimes occurring during peak call periods.
In order to help beneficiaries understand their drug plan choices and select the plan that best meets their needs, CMS increased the number of Customer Service Representatives (CSRs) from 3,000 in June of 2004 to as many as 7,800. We have also acquired additional infrastructure including telephone lines, workstations, and seats at call center sites. We have refined our CSR scripts by reducing redundant information, indexing scripts for quick access, and including probing questions to help the CSRs better identify the caller's concerns. In addition, all beneficiary toll-free numbers were moved to a single 1-800 number with a centralized Interactive Voice Response (IVR) system, allowing beneficiaries who call 1-800 MEDICARE to get answers to all Medicare questions through a single number, which has helped to channel calls appropriately and improve efficiency. Further, the IVR system was enhanced to incorporate more plain language, user-friendly functionalities, and synonyms for common beneficiary terms. CMS has implemented a major enhancement through the use of Smart Scripts, which provide the CSRs with an easily followed path of responses to the most frequently asked questions. Smart Scripts are a new type of script that has hyperlinks built into the body of the text. When activated, these hyperlinks will take the CSR directly to related information about that subject. In addition, we have CSRs participate in the content workgroups for the actual development of scripts and job aides. CMS has also implemented a CSR feedback system and streamlined our approval process for updating the scripts in a timely manner to respond to the changing needs of our customers or to incorporate policy updates. All CSRs receive one week of classroom training followed by two or three additional days of practice calls, simulation, quality monitoring, and follow-up coaching to ensure peak performance. CSRs are required to be certified with a written examination and test calls prior to taking live calls. CMS has taken steps to strengthen the call centers' capabilities and reduce wait times in order to address beneficiaries' concerns as they arise. CMS hired and trained additional staff to use the Prescription Drug Plan Finder tool to help beneficiaries get the information they need to enroll in a drug plan that suits their needs. I am pleased to say that CMS customer satisfaction surveys indicate that the bulk of callers who interact with our CSRs, 87 percent, are satisfied with their experience. They are particularly pleased with how courteous and patient the CSRs are (rated at 97 percent). These responses came not only from people with Medicare, but also friends or relatives calling on their behalf, who made up 23 percent of callers during March 2006. In addition to beneficiary satisfaction surveys, CMS also evaluates the 1-800- MEDICARE CSRs through "mystery shopping" to ensure they are providing accurate and complete responses to callers. "Mystery shopping" calls are made to CSRs by an independent specialized quality evaluation contractor who has developed scenarios and scripts to measure the CSRs on various topics to determine if CSRs are being "fully responsive." A response is considered "fully responsive" if all key points are conveyed to a caller. We have consistently found that the information provided by the CSRs was fully responsive to the caller's needs most of the time. CMS' Medicare web site, www.medicare.gov, has also been a source of useful information for people with Medicare. Since the first of the year, our frequently asked questions have been accessed more than one million times. CMS also has responded to more than 19,000 e-mails received through the site, with 93 percent of them being resolved satisfactorily in the first response. In addition, the medicare.gov web site has been visited more than 829 million times since January 1, 2006. With the array of educational tools available, I am confident that beneficiaries are getting the information they need to enroll. We have seen steady enrollment since November 15th. CMS Works with Plans to Improve Their Customer Service While many plans are now providing timely phone access, some have not responded adequately. Therefore, CMS has increased monitoring of plans' call center activities to help assure a high level of performance. We are surveying all prescription drug plans to assess whether they provide correct information to beneficiaries and pharmacists within a reasonable time. We expect continuing improvements as we address systems and data transfer issues. The 2007 Call Letter provides specific wait time metrics to which the plans must adhere, which I will outline shortly. CMS Provides Caseworkers for One-on-One Counseling CMS has established a system to help resolve urgent issues on a case-by-case basis. CMS has hundreds of trained caseworkers who are working as rapidly as possible to resolve urgent issues to help ensure that people with Medicare get their prescriptions filled. CMS urges people with Medicare or their family members who are having difficulties to call 1-800-MEDICARE, and if necessary, their case will be forwarded to our caseworkers. Urgent cases have high priority for rapid resolution. While the number of individual cases is small in comparison to the millions of prescriptions and individuals who are successfully receiving their prescriptions, CMS is committed to ensuring that every individual receives his or her needed medicines, is properly identified, and is charged the appropriate copays. CMS Takes Steps to Identify Areas of Concern CMS developed the Complaints Tracking Module (CTM) to capture complaints CMS receives from beneficiaries, providers, or plans about prescription drug plans, pharmacies, subcontractors, and providers. The design of CTM evolved from CMS' experience with the Medicare approved prescription drug cards. Because it is a web-enabled system, it can accept large numbers of daily transactions simultaneously from many users across the Agency. Information can be efficiently exchanged, which allows for quicker resolution and accountability. CMS launched the CTM into production October 3, 2005 and began tracking complaints in January 2006 and we have seen a general decline in the number of complaints during this time. In addition, in order to assist pharmacists, who have been outstanding in their commitment to service, CMS is working to ensure they have the resources and support they need. CMS is also coordinating with the States that used their state reimbursement systems to pay for prescriptions that should be paid by the new Medicare prescription drug plans. We are also monitoring plan activities and will use our enforcement measures, if necessary, to ensure they are adhering to the requirements of participating in the Medicare prescription drug program. The 2007 Call Letter outlines CMS plan sponsor evaluation criteria. These efforts build on the preparations that were made long before the January 1, 2006 launch of the Medicare prescription drug benefit. In addition, the 2007 Call Letter contains policy statements developed in response to lessons learned during the Part D program implementation. It also features reiteration of existing program requirements to emphasize their importance to CMS and to our beneficiaries. CMS Applauds and Supports the Outstanding Work of Pharmacists CMS Provides Dedicated Support to Pharmacists To help resolve issues pharmacists encounter in dispensing medications to those newly enrolled in the Medicare prescription drug plans, CMS has increased its call handling capacity at the pharmacist help line. In addition, the line is now available 24 hours a day. This increased capacity has reduced the wait time to less than a minute for pharmacists who want to use this mode of communication for eligibility and enrollment determination. CMS Supports Simplification Initiatives CMS has also identified a number of business process issues that can be simplified for plans, physicians and beneficiaries. To supplement established prescription drug reject codes, America's Health Insurance Plans (AHIP), the National Association of Chain Drug Stores (NACDS), the National Community Pharmacists Association (NCPA), and others have announced standardized coding messaging designed to assist pharmacists and better serve beneficiaries when they fill prescriptions at pharmacies. Specifically, these standardized electronic messages will help pharmacists quickly determine the appropriate course of action for filling beneficiaries' prescriptions under four different circumstances: (1) when a particular drug is not covered; (2) when prior authorization is required; (3) when plan quantity or other coverage limitations have been exceeded; and (4) when the pharmacy is not part of the Part D plan's network. This consensus agreement on new message coding protocols will make transaction processing more streamlined and efficient which will save time and prevent phone calls and delays between plans and pharmacists. This is important not only for the Medicare drug program, but may produce benefits throughout our entire health care system, as these and other protocols are applied to other public and private programs. CMS now views these consistent messages as best practices for the drug benefit, and we expect all Part D plan sponsors to adopt and implement these practices as soon as possible. We will be looking at these and other best practices as measures of plan performance. To further the goal of simplifying procedures in the new drug benefit, last week the American Medical Association (AMA) and America's Health Insurance Plans (AHIP), in conjunction with CMS, released a standardized exceptions form designed to assist physicians in requesting exceptions and prior authorizations on behalf of Medicare beneficiaries enrolled in Medicare drug plans. This form allows for a simplified process for physicians to apply for coverage determinations on behalf of all of their Medicare patients, regardless of which Part D plan the beneficiary is enrolled in. In addition to the new messaging standards, we sent information to the plans which will expedite their processes for making sure they are not inappropriately paying for drugs that should be covered under Part B, and we have worked with Epocrates, an electronic prescribing software company, to ensure that their product provides accurate and easy access to plan formularies. We've also held weekly prescribers' conference calls and bi-weekly meetings with the AMA and other organizations to find out what prescribers are experiencing, to supply them with information on our activities and answer their specific questions. CMS issued a fact sheet on February 24, 2006 to provide physicians with updated, practical information about the exceptions and appeals processes. This fact sheet describes the physician's role in these processes and emphasizes the short decision-making timeframes. In addition, on March 24, 2006, CMS held a "Coverage and Appeals" training session for providers and other CMS partners. We had close to 1,500 sites calling in for the training, and we conservatively estimate that 3,000 people were listening in. CMS Facilitates Creation of the Pharmacy Quality Alliance I am very pleased to announce the establishment of the Pharmacy Quality Alliance (PQA). Similar to the Ambulatory Quality Alliance (AQA), the mission of the Pharmacy Quality Alliance is to improve health care quality and patient safety, and to reduce overall healthcare costs. The PQA will use a collaborative process in which key stakeholders agree on a strategy for measuring performance at the pharmacy level; collecting data in the least burdensome way; and reporting meaningful information to consumers, plans, providers, and other stakeholders to inform choices and improve health outcomes. The Alliance highlights the role of the pharmacist as a member of the integrated health care team and recognizes the value the pharmacist can bring to the equation of total patient care. CMS may further support this collaborative process by developing a demonstration project to provide further evidence on the impact of Medication Therapy Management (MTM) and other pharmacist interventions that could help promote high quality patient care and lower costs in both the Medicare and Medicaid programs - a win-win for plans, pharmacists, and most importantly, beneficiaries. Individuals with more than one chronic disease often require treatment with several prescription medications, which increases their risk for drug related problems. Additionally, they represent a disproportionate amount of health care expenditures. Each Part D sponsor must have an MTM program for beneficiaries who have multiple chronic diseases and are taking multiple Part D drugs with projected annual costs of at least $4,000. The quality of care for these individuals can be improved and medical costs can be reduced through MTM, which promotes appropriate medication use, reduces the risk of adverse events, and optimizes therapeutic outcomes. MTM programs may be furnished by a pharmacist or other qualified provider and must be developed in cooperation with pharmacists and physicians. This creates opportunities for the pharmacists to play active roles in the MTM services provided. To realize the full potential of MTM, quality metrics for MTM and related pharmacy services must be developed so that more can be done to support high-quality pharmacy care. Physician Outreach Provides Information about Formularies, Exceptions, Appeals, and Expedited Requests
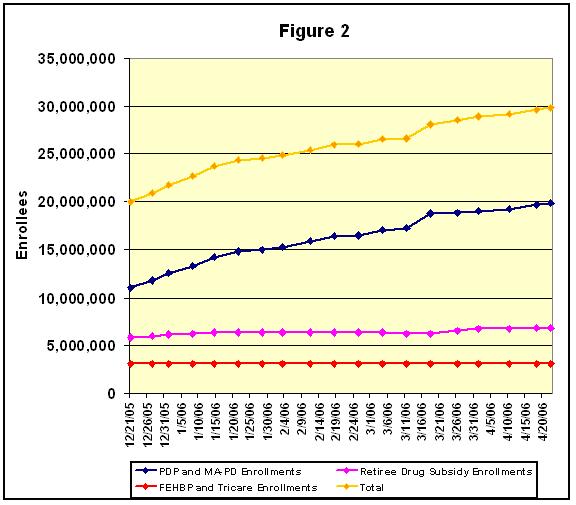
Strong Enrollment Trends Continue Overall prescription drug coverage figures as of April 18 are:
So, in addition to over eight million beneficiaries in stand-alone prescription drug plans, many millions more are getting more comprehensive coverage in Medicare Advantage plans, and millions more continue to receive retiree coverage-exactly as the law was intended to work.
In addition to general participation, CMS research indicates that our partners' and our outreach efforts have been particularly successful in minority communities. Seventy percent of Medicare-eligible African Americans, 75 percent of Asians, and 70 percent of Hispanics have enrolled in Part D or have coverage from an employer taking the retiree drug subsidy. These figures exclude FEHB and TRICARE. Polls show that people are finding the enrollment process easy and are saving money from participating in the benefit. An AARP survey found that 78 percent of those enrolled in a Medicare prescription drug plan say they are satisfied.5 An AHIP survey released on March 13, 2006 found that nine out of 10 seniors who are dually eligible for Medicare and Medicaid say they have experienced no problems using the new Medicare drug benefit.6 According to AARP's survey, of those surveyed who had prescription drug coverage before 2006, 63 percent indicated that their Medicare drug plan is either better or as good as their previous coverage. Further, the survey found that 40 percent of survey participants thought if Medicare had not added the new prescription drug benefit, they would need to give up things such as groceries, full dosages of medication, or cut back on savings. More than 30 million Medicare beneficiaries now have prescription drug coverage and CMS is encouraged by the strong enrollment numbers. Outreach efforts will continue to promote enrollment for those who have not yet enrolled. Competition Helps Lower Drug Prices CMS analyses demonstrate that Medicare beneficiaries with common chronic conditions can save a substantial amount on their drug bills by enrolling in a Medicare prescription drug plan (PDP) compared to what they would pay with no drug coverage.7 For instance, people with Medicare who select the lowest-cost plan in their area may find savings up to 71 percent off the prices they would pay without prescription drug coverage. The analysis also demonstrates that a range of plans available to beneficiaries can provide significant savings. This is also true for a very broad range of plans if beneficiaries are willing to use generic versions of their existing drugs, when available, which are required to have the same active ingredients and work in the same way as the brand-name drug. These results indicate that beneficiaries can see substantial savings on their drug bills by focusing on a few plans with the features they prefer - such as a low premium, or fixed copayments, or coverage in the gap, and low out-of-pocket costs. Even larger savings are possible - as much as 83 percent - by switching to drugs in the same class that treat the same condition as a beneficiary's current brand-name drug, for example drugs that treat common conditions like stomach acid problems, allergic rhinitis, high blood pressure, and high cholesterol levels. According to Consumers Union, considering these alternative drugs could save beneficiaries billions more in drug costs each year.8 Beneficiaries can get personalized information on these additional savings from www.medicare.gov, 1-800-MEDICARE, and many of Medicare's partners. A number of external reports strongly support these findings. For example, the Pharmaceutical Care Management Association (PCMA) released a study in February 2006 indicating that Medicare drug plans offer significant price discounts compared to what beneficiaries would pay without coverage.9 The study found that prices under the Medicare prescription drug program were on average 35 percent less at participating retail pharmacies and 46 percent less through mail order pharmacies. Further, for 25 commonly used medications, the PCMA study found savings from 18 percent on brand name drugs at retail pharmacies to 26 percent at mail order pharmacies. In addition, a January 2006 report prepared by the Lewin Group demonstrates that beneficiaries with chronic conditions, particularly those with multiple conditions, will see significant savings on their prescription drug bills by enrolling in a Medicare prescription drug plan.10 For example, while beneficiaries with one chronic condition will save on average $396 on their medications with Medicare drug coverage, accounting for 26 percent of their current drug spending, those with four or more conditions will save an average of $1,774, or 41 percent, on their medications. These studies have made "apples to apples" comparisons of drug prices available at retail pharmacies instead of, for example, common, but misleading, comparisons between retail pharmacy and mail-order prices. In addition, in their recent forecast of prescription drug spending trends, the independent Medicare actuaries have concluded that overall drug spending in the presence of the Medicare drug benefit will be slightly lower when compared to spending in the absence of a Medicare drug benefit, even though Medicare beneficiaries will be able to fill millions more prescriptions than would have been possible without the drug coverage. Beneficiary premiums are expected to average $25 a month - down from the $37 projected in last July's budget estimates - and the overall cost to taxpayers for 2006 has dropped about 20 percent since the July 2005 estimate, according to the CMS Office of the Actuary. The savings result from lower than expected costs per beneficiary; projected enrollment in the drug benefit has not changed significantly. For the 10-year period from 2006-2015, the net total cost of the drug benefit to Medicare is now estimated to be about $130 billion less - $797 billion compared to an estimated $926 billion last year.11 In addition, the state phase-down contributions are now projected to be $37 billion (about 27 percent) less over the 10-year period. Market Forces Drive Plan Simplification Medicare and its partners are already making available personalized information on important plan features, and we are working with many outside organizations to enhance the resources available to beneficiaries to help them identify the specific plan or plans that are a good fit based on their own preferences. As individuals have different needs and preferences when it comes to their health-care coverage, presenting plan features in a way that facilitates comparison on the basis of plan attributes and performance indicators will make it easier for beneficiaries to choose the plan with the features that are most important to them. In our research, we found that the vast majority of the new enrollees in stand-alone drug plans have chosen plans offering a plan design other than the "standard" drug benefit. Many beneficiaries chose coverage with a low or no deductible, fixed copayments for most prescriptions instead of coinsurance, and/or coverage in the coverage gap - coverage options made possible by the strong competition in the Medicare drug benefit. In fact, as Figure 3 shows, CMS found that nearly 69 percent of PDP and almost 90 percent of MA-PD enrollees chose a plan with no Part D deductible. A very small percentage (2 percent) of PDP enrollees selected plans with a deductible between $1 and $249, and 29 percent of the enrollment was in plans with a $250 deductible.
The range of premiums offered by PDPs varies between $1.87 and $104.89, and the Part D portion of the MA-PD total premium ranged from $0 to $147.12. The majority of PDP enrollees are in plans with drug premiums below the national average. In fact, as shown in Figure 4, while 38 percent of PDP plans offered premiums below $32.20, 73 percent of the beneficiaries enrolled in one of these plans. It appears that beneficiaries place a high priority on premium when selecting a plan.
CMS Automatically Enrolled Full Benefit Dual Eligible Individuals into Plans CMS has also worked with the States to identify and auto-enroll individuals who are about to become full-benefit dual eligible prior to the end of their Medicaid drug coverage to work toward a seamless transition. This includes those Medicaid individuals who will age into Medicare or who will reach the end of the 24-month Medicare disability waiting period. In anticipation of the shift of drug coverage from Medicaid to Medicare for full benefit dual eligible individuals, CMS developed a process for a back-up plan at the pharmacy point-of-sale to ensure that these individuals experience no gap in coverage. CMS Facilitates Enrollment for Individuals who Qualify for the LIS In the first phase of this effort, CMS began mailing letters to approximately 1 million people who are LIS-enrolled but have not chosen a plan. The letters let them know which Medicare prescription drug plan they would be enrolled in if they took no action before April 30th and that their prescription drug coverage would begin on May 1st. The letter explains that beneficiaries can choose a different approved plan in their area. It listed all the prescription drug plans available in their region with premiums at or below the low-income premium subsidy amount. It also makes clear that they can decline enrollment if they choose and recommends calling 1-800-MEDICARE to find out more about these plans. Medicare beneficiaries who qualify after May 15th for the LIS will have a one-time opportunity, using a special enrollment period, to enroll in the drug benefit if they have not already done so. The extra help allows for comprehensive and valuable drug coverage - in most cases it means beneficiaries must pay just a few dollars for every prescription - and we want to make sure that people who need help the most can use this coverage as soon as they become eligible. The change in status resulting from an LIS determination after May 15th is an "exceptional circumstance" that warrants a special enrollment period. This special enrollment period enables these beneficiaries to enroll in a Medicare prescription drug plan right after they become eligible for the LIS. Medicare will also continue to facilitate enrollment into a drug plan for people who qualify for the LIS if they do not choose a plan on their own. Medicare similarly offers one-time special enrollment periods for other important changes in status. CMS Worked to Achieve a Smooth Transition in Long Term Care Facilities CMS established dedicated fax lines and mail-in services to allow nursing homes to obtain beneficiary enrollment information from CMS. This strategy enabled CMS to help nursing homes identify the plans into which CMS auto-enrolled more than 500,000 residents. Pharmacists used the electronic eligibility and enrollment verification (E1) system to identify the remainder of beneficiaries. By notifying plans that their dual eligible enrollees reside in nursing homes, and by assisting LTC facilities in working to correct cases where copay information is not up to date, CMS is ensuring nursing home residents who are full-benefit dual eligible beneficiaries have access to Medicare drug coverage without premiums and copays. CMS Has Taken Specific Steps to Address Areas Where State Changes are Needed We are committed to making the distinctions between Part D versus Part B coverage as clear as possible. CMS is currently working with providers, states, and the home infusion industry to clarify payment obligations under Medicare for home infusion therapy. In addition to comprehensive guidance issued in 2005, we recently distributed a quick reference chart to plans and pharmacists and posted a MedLearn article on the subject. In March, CMS sent to plans and the State Medicaid Directors letters clarifying the roles of the Medicare Part D drug program and State Medicaid programs in providing home infusion drugs and services. The letter clarified CMS access requirements for home infusion drugs, provided information about how home infusion drugs must be provided in usable forms, addressed the need for plans to receive assurances that ancillary services will be provided, and provided a reminder of the time sensitive nature of home infusion therapy. Further, we recently sent information to the plans which will expedite their processes for making sure they are not inappropriately paying for drugs that should be covered under Part B, and we have worked with Epocrates, an electronic prescribing software company, to ensure that their product provides accurate and easy access to plan formularies. We've also held weekly prescribers' conference calls and bi-weekly meetings with the AMA and numerous specialty societies to find out what prescribers are experiencing, to supply them with information on our activities and answer their specific questions. Finally, on February 13, 2006, we sent letters to medical specialty groups recommending that providers include certain additional information on prescriptions that may help plans and pharmacists differentiate between Part B and D drugs. CMS Works With States CMS also engaged the States in a series of summits, conference calls, and workshops to discuss and address implementation issues associated with the MMA. These gatherings include monthly all-State conference calls; State Pharmacy Assistance Program Workgroup conference calls; and conferences hosted by organizations representing the States. In addition, CMS provided States with beneficiary enrollment information, comparative information about the plans, and targeted educational and outreach materials. Finally, CMS has worked diligently with States to appropriately identify their full benefit dual eligible individuals. Reimbursing States for Assisting in the Transition Process To that end, we have established a demonstration project to reimburse the 50 States and the District of Columbia for costs they incurred by covering drugs that should be covered by the appropriate plan. Under the demonstration, Medicare will reimburse States by reconciling drug payments with prescription drug plans, and by paying any differential between the drug plan reimbursement and Medicaid costs, as well as certain state administrative costs. Forty-five States and the District of Columbia have been accepted into the demonstration program. Of the States accepted into the demonstration program, 12 did not activate their state payment systems and are seeking reimbursement only for administrative costs. In February we notified states that they could apply for reimbursement for the help they provided to beneficiaries during the transition until March 8, with some states receiving extensions until March 31 for costs associated with Part D claims. By the time that deadline occurred, the vast majority of early difficulties had been resolved and states no longer needed to provide emergency back-up. We are ready to honor our commitment to states. CMS has extended the deadline for states to incur administrative costs related to transition full benefit dual eligible individuals to May 5, 2006. We are currently working through a contractor to process claims, reconcile with plan sponsors, and begin reimbursing states. CMS is Correcting Data Transmission Issues As an additional safeguard in mid-January, CMS contracted with Electronic Data Systems (EDS) to help CMS work together with the plans, States, and pharmacies to resolve challenging data translation issues. CMS has worked diligently to ensure our data systems interact properly with other systems so that data information exchanges are accomplished smoothly and completely to correct problems. Many plans are sending CMS daily files reflecting their enrollment transactions, and reliably use our responses to these daily files as well as our weekly summaries of the results for timely and accurate updates of their systems. Our goal is that plans covering 90 percent of the enrollee population will use these daily and weekly data transfer processes successfully to reduce lags in obtaining updated beneficiary information. To check and further assure the accuracy of the information exchange between plans and CMS, we have sent special updated data files to plans, including full copayment information, on the full dual and low-income subsidy enrollment in plans. Our goal is to achieve, by ten days before a new coverage month begins, at least a 95 percent match for enrollment and LIS copayment information on applicable beneficiaries between Medicare and the plans. We obtained a match rate of greater than 99 percent for duals submitted by the States in the fall of 2005, and we expect to maintain a high match rate. CMS is Monitoring Plan Compliance Key dimensions of customer service include timely access for beneficiaries and their representatives, pharmacists, and other health professionals. HHS is conducting routine surveys to determine plan compliance with Part D standards concerning call abandonment rates and percentage of calls answered within 30 seconds. Plans will receive this analysis to inform their performance and compliance analysis, and information on the performance of plan service lines will be publicly available in the weeks ahead. Complaint rates related to customer service are also an important consideration for future participation by a plan. We are addressing issues on a case-by-case basis. While we are responding to complaints, we are also monitoring trends. This tracking information can lead to corrective action or sanctions if needed, and will be considered in our contracting decisions for future years. While most plans are complying with the requirements set forth in their contracts, we will use the full array of administrative tools and other enforcement remedies to ensure plans adhere to the terms of their contracts. When we hear of specific complaints we work with plans to ensure timely resolution. Extensive Plan Formulary Requirements Provide Access to Needed Prescription Drugs In addition, each Medicare prescription drug plan's formulary was developed and reviewed by the plan's pharmacy and therapeutics committee. Each formulary must be consistent with widely used industry best practices. Furthermore, CMS compared the prescription drug plans' use of benefit management tools to the way these tools are used in existing drug plans to ensure they are being applied in a clinically appropriate fashion. Plans must accommodate the needs of long-term care residents within their formulary structure by providing coverage for all medically necessary Part D medications at all levels of care. Coverage of all medically necessary medications may include, but is not limited to, alternative dosage forms such as liquids that can be administered through feeding tubes, intravenous medications, or intramuscular injections. CMS will review any request for deletion of a drug from a plan's formulary to ensure continued access to a broad range of drugs. Plans cannot remove a drug from their formulary without, among a number of other steps, first obtaining CMS approval and providing a 60-day advance notice to their affected enrollees. As we deem it appropriate, we are working to strengthen formulary protections. On April 26, we changed our policy to better protect Medicare beneficiaries from the sudden loss of coverage for drugs they currently take. Now, plans that change their formularies during the year will exempt beneficiaries who are already receiving the drugs when the change is made. This should provide many beneficiaries with greater peace of mind that their prescription drugs will remain covered throughout the plan year. The enrollment period continues for almost two more weeks and we are encouraging and helping people with Medicare to review their options and select a plan that works best for them. In addition, CMS developed specific procedures for timely exceptions and appeals to ensure that enrollees receive prompt decisions regarding whether medications are medically necessary and therefore covered by their prescription drug plan. For example, if the enrollee is requesting coverage of a non-formulary drug, the drug may be covered if the prescribing physician determines that all of the drugs on the formulary would not be as effective as the non-formulary drug or would have adverse effects for the enrollee, or both. The plan would review the physician's determination and must make its decision as expeditiously as the enrollee's health condition requires after it receives the request, but no later than 24 hours for an expedited coverage determination or 72 hours for a standard coverage determination. We are collecting information on the use of a plan's appeals and grievance processes to ensure that each plan is complying with the requirements. CMS is Ensuring Pharmacists Receive Prompt and Accurate Payments from Plans CMS Commitment to Continuous Quality Improvement demonstrated in Annual Adjustments for 2007 CMS Anticipates Bids Will More Clearly Reflect Variations that Beneficiaries Prefer Plans will continue to have flexibility to offer people with Medicare benefit designs with these popular features in 2007. However, in general we expect that more than two bids from a sponsoring organization would not provide meaningful variation, unless one of the bids is an enhanced alternative plan. Further, CMS anticipates that plan sponsors will design new plan options for 2007 in accordance with the enrollment trends in 2006. CMS Evaluation Criteria
CMS Changes Co-Branding Policy in 2007 Anticipating Next Steps In addition, we will continue to improve data translation among Medicare, the health plans, and States to continue reductions in the number of rejected or delayed transactions. CMS also is monitoring plans' customer service and hotline wait times, while also providing responsive service through 1-800-MEDICARE. CMS continues to work with the States participating in the reimbursement program to ensure effective use of Medicare coverage by connecting beneficiaries to their new Medicare prescription drug plans and helping pharmacists use Medicare backup systems if necessary. As implementation continues, and more and more beneficiaries select and enroll in a new prescription drug plan, CMS will continue to improve the program and solve problems, guided by the lessons we have learned to date. Conclusion
---------------------- Last Revised: May 4, 2006 |