|
|
|
|
|
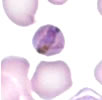
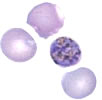
(contributed by Prof. Jacques Le Bras, Hôpital Bichat - Claude Bernard, Paris, France) A 30 year-old woman, HIV-positive, delivers by planned cesarean section an apparently normal female baby, weight 3.2 kg (7 lbs). At delivery AZT is administered IV for 7 hours. The mother is a native of the Democratic Republic of Congo (DRC) who came to France 2 years ago and has not traveled outside France since then. The only abnormality found in the baby at delivery is an anemia (12.3 g/dL hemoglobin) attributed to antiretroviral drugs toxicity (ARV given to mother?) At 6 weeks post-delivery, the infant is brought in for a fever of one-day duration. She is found to have a temperature of 38.5°C and both hepatomegaly (3 cm) and splenomegaly (3 cm). Serologic tests for HBs and HCV are negative, and PCR, DNA and RNA for HIV are negative. More routine laboratory exams show: hemoglobin 6.4 g/dL, platelets 122,000/µL, LDH 1080 IU/mL, and blood smears showing the following:
Question 1. What is your diagnosis?
A transfusion of 125 mLs of blood (serologically negative for CMV) is given to the child. Question 2. What antimalarial drug would you administer to the infant? Following treatment with the orally administered antimalarial drug, parasitemia drops to 1% by day 3. At day 7, some parasite remnants are found and the child is afebrile. Drug testing in vitro of the parasite shows it to be sensitive to chloroquine. Question 3. What test(s) would you perform to confirm current infection of the mother? A thick blood smear of the mother, taken 5 days after that of the infant, is indeed positive, while on the thin smear no parasites can be detected. Main Points
See Congenital Malaria as a Result of Plasmodium malariae - North Carolina, 2000. Page last modified : April 23, 2004 Content source: Division of Parasitic Diseases National Center for Zoonotic, Vector-Borne, and Enteric Diseases (ZVED)
|
|
||||||||||||||||||||||||||

| Home | Policies and Regulations | Disclaimer | e-Government | FOIA | Contact Us | ||||||
|