The President's Emergency Plan for AIDS Relief: First Annual Report to Congress
Released by the Office of the U.S. Global AIDS Coordinator
May 23, 2005
Chapter 1 -- Critical Intervention in the Focus Countries: Prevention

Prevention is one of the cornerstones of the President’s Emergency Plan for AIDS Relief (PEPFAR/Emergency Plan). To limit the progression of the HIV/AIDS pandemic, there must be a dramatic reduction in new infections. By 2008, the President’s Emergency Plan will seek to prevent 7 million new HIV infections in the 15 focus countries. The President’s Emergency Plan is working rapidly to deploy prevention resources and build sustainable systems for future prevention efforts, recognizing the reality that in 2004, 14,000 people were newly infected around the world every day. More than half of those infected were between the ages of 15 and 24.
 It is estimated that existing prevention efforts reach fewer than one in five of those at risk. Thus, one of the most significant challenges the Emergency Plan faces is to scale up prevention efforts to reach the millions of people at risk of HIV infection worldwide. To this end, in fiscal year 2004 the Emergency Plan committed $193,097,000 to prevention programs in the focus countries. It is estimated that existing prevention efforts reach fewer than one in five of those at risk. Thus, one of the most significant challenges the Emergency Plan faces is to scale up prevention efforts to reach the millions of people at risk of HIV infection worldwide. To this end, in fiscal year 2004 the Emergency Plan committed $193,097,000 to prevention programs in the focus countries.
Young people are an important focus of the Emergency Plan’s prevention efforts. Of particular concern are the dramatic increases in HIV infection among girls and young women, who now make up more than 60 percent of 15- to 24-year-olds living with HIV/AIDS in some focus countries. In some of the focus countries, adolescent girls face infection rates that are up to six times higher than those of boys of the same age.
The President’s Emergency Plan employs a combination of prevention programs in order to support individual risk behavior change; improve preventive medical services; influence social norms regarding risk behaviors; and address social, economic, legal, and policy barriers to effective prevention. These programs include promotion of behavior change aimed at risk avoidance and risk reduction; prevention of mother-to-child transmission of HIV; provision of comprehensive programs for individuals who engage in high-risk behavior (including connecting them to HIV counseling and testing services, treating them for sexually transmitted diseases, and providing them with condoms, when appropriate); and reduction of medical transmission of HIV by ensuring safe blood supplies, safe medical injections, and training in universal medical precautions.
President Bush’s Emergency Plan is committed to the development and application of evidence-based best practices that are informed by and responsive to local needs, local epidemiology, and distinctive social and cultural patterns, and are coordinated with the HIV/AIDS strategies of host governments. The Plan promotes the strong engagement and involvement of people living with HIV/AIDS, because engaging these people in HIV prevention is critical to successful interventions. The involvement of people living with HIV/AIDS can help reduce transmission by providing effective advocates for change and increasing adoption of prevention behaviors.
The Emergency Plan builds upon the synergies that exist among prevention, care, and treatment. Just as prevention programs are unlikely to achieve full impact in the absence of treatment, the impact of care and treatment programs is reduced without vigorous prevention efforts. In 2003, it is estimated that 3 million people died of AIDS. At the same time, 5 million more became infected. In the long fight against HIV/AIDS, the tide will not turn in the absence of effective prevention.
Abstinence and Be Faithful Programs
Results: Rapid Scale-Up
In fiscal year 2004, the Emergency Plan made significant progress in targeting messages and interventions to specific groups, especially young people. In many countries in which the Emergency Plan works, the demographics are such that youth (ages 10 to 24) represent approximately one-third of the total population. The vast majority of new infections in the 15 focus countries occur through sexual transmission. Evidence from countries such as Kenya, the Dominican Republic, Thailand, Ethiopia, Zambia, and Uganda indicate that changing social norms through the promotion of behaviors aimed at risk avoidance and risk reduction will likely avert a large number of new infections and reduce the spread of HIV. The approach endorsed by the Emergency Plan ABC: Abstain, Be faithful, and, as appropriate, correct and consistent use of Condoms - employs population-specific, targeted interventions that emphasize abstinence for youth and other unmarried people, including delay of sexual debut; mutual faithfulness and partner reduction for sexually active adults; and correct and consistent use of condoms by those whose behavior or circumstances place them at risk for transmitting or becoming infected with HIV. This targeted approach results in a comprehensive and effective prevention strategy that helps individuals personalize risk and develop tools to avoid the risk behaviors that are under their control.
In fiscal year 2004, the Emergency Plan supported a range of interventions and programs to reach individuals with lifesaving prevention messages and skills. These included the mobilization of communities through peer education and school-based and workplace programs; the engagement of local leaders, including the faith community; and the development and use of multiple targeted media channels, including television, radio, and print. These interventions focused on seven central themes:
- Promotion of abstinence, including delayed initiation of sexual activity and secondary abstinence for youth who have already become sexually active
- Promotion of mutual faithfulness in reducing HIV transmission among individuals in long-term sexual partnerships
- Elimination of casual sex and multiple sexual partnerships
- HIV counseling and testing for individuals and couples who do not know their HIV status
- Development of skills for sustaining marital fidelity
- Adoption of social and community norms supportive of marital fidelity and partner reduction using strategies that respect and respond to local customs and norms
- Adoption of social and community norms that denounce forced sexual activity in marriage or long-term partnerships
During the reporting period, $91,630,000 was dedicated to prevent the sexual transmission of HIV; $50,545,000 (56 percent) was allocated to abstinence and faithfulness (AB) programs. When resources for PMTCT, blood safety, and safe medical programs are considered, 27 percent of total prevention funding was dedicated to AB programs. These funds supported 1,000 community outreach programs that promoted abstinence and faithfulness, reaching more than 24 million individuals. Of the more than 17 million of these people for whom gender is known, more than 8.3 million were female. As a subset of AB programs, 200 programs that promoted abstinence as their primary behavioral objective reached approximately 11.5 million individuals. The President’s Emergency Plan supported 135 mass media programs focused on AB messages that reached an estimated 120 million people. More than 32.1 million people were reached by 25 mass media campaigns promoting abstinence.
![Table 1-1 -- Prevention: FY04 Results of Community Outreach Programs that Promote Abstinence and Being Faithful [AB]](https://webarchive.library.unt.edu/eot2008/20081107002934im_/http://www.state.gov/cms_images/chapter_1-3.jpg)

Sustainability: Building Capacity
As in other areas of the Emergency Plan, the long-term sustainability and success of prevention programs depends on the ability of local organizations, communities, and individuals to develop, implement, and support programs over time. This is particularly important in the area of behavior change, as constant support and
![Table 1.2 -- Prevention: FY04 Results of Mass Media Programs that Promote Abstinence and Being Faithful [AB]](https://webarchive.library.unt.edu/eot2008/20081107002934im_/http://www.state.gov/cms_images/chapter_1-5.jpg)
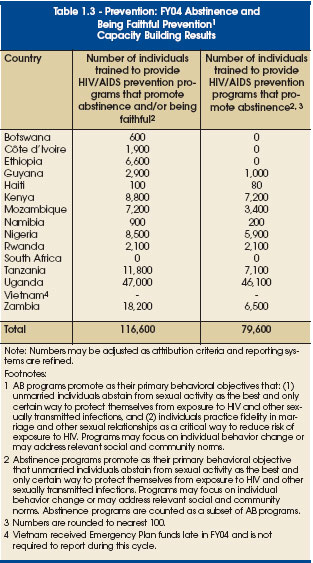
adaptation are required to sustain the changed social norms that promote safe sexual behaviors. Given the complexity of the issues, success also greatly depends on the long-term involvement and commitment of local organizations, leaders, and communities. To achieve this, the Emergency Plan supports activities reaching from the highest level of a country to the local community. For example, the Emergency Plan supports the development of national life skills curricula in schools to give youth the tools they need to lead healthy sexual lives. At the community level, support is provided to train local leaders, the faith community, and youth through peer education programs. Activities strengthen local organizations to help them implement strong technical programs and manage their organizations effectively. During the reporting period, more than 116,600 people were trained to support the promotion of abstinence and/or be faithful prevention services, including more than 79,600 trained to provide abstinence-only prevention programs largely targeted to youth.
Key Challenges and Future Directions
Despite the great progress made in reaching people with lifesaving prevention messages and tools, important challenges remain and will be addressed in the upcoming year. These challenges include the need to continue to refine and focus behavior change interventions toward target groups and individuals, ensuring that implementation is consistent with the Emergency Plan’s results-driv-en strategy. It will also be important to deepen the knowledge base about determinants of sexual behavior in order to ensure effective abstinence programs.
Combating stigma, sexual coercion, exploitation, and violence continues to be a significant challenge. Faith communities have a special role to play in continuing to broaden and deepen their efforts to combat stigma, discrimination, and sexual violence, as do programs that target boys and men. Given the importance of partner reduction and mutually faithful relationships in reducing HIV transmission, the "Be faithful" component of ABC programs will be strengthened in the upcoming year. There is a need to further identify the parameters of a quality program and outcome indicators, given the wide array of diverse community organizations and approaches to behavior change.
Prevention for People Who Engage in High-Risk Activity
Results: Rapid Scale-Up
The ABC approach recognizes that comprehensive services, including risk reduction and risk avoidance counseling, linkages to HIV counseling and testing, treatment of sexually transmitted infections (STIs), and promotion of correct and consistent condom use, are an essential means of reducing, but not eliminating, the risk of HIV infection for individuals who engage in high-risk activity. Such high-risk activity includes engaging in casual sexual encounters; engaging in sex in exchange for money or favors; having sex with an HIV-positive person or one whose status is unknown; using drugs or abusing alcohol in the context of sexual interactions; and using intravenous drugs. Discordant couples, in whom one partner is HIV-positive and the other is not, are a crucial target group. In Uganda, for example, approximately one-third of couples are discordant. Women, even if faithful themselves, can still be at risk of becoming infected by their spouse, regular male partner, or someone using force against them.
 The experiences of Thailand, Cambodia, the Dominican Republic, Senegal, and other countries illustrate that targeted efforts with people who engage in high-risk activity can be effective in preventing the spread of HIV infection. In countries such as Vietnam and Guyana, where HIV infection has yet to move into or is at low levels in the general population, aggressive prevention strategies among people who engage in high-risk activity are critical to stop the spread of infection; because these individuals often serve as a "bridge" to those at lower risk, they are an essential target group. Such people at high risk, including sex workers and their clients, men who have sex with men, and injecting drug users, are among those who are most marginalized in society and have the least access to basic health care, yet they are often in the greatest need of services. The experiences of Thailand, Cambodia, the Dominican Republic, Senegal, and other countries illustrate that targeted efforts with people who engage in high-risk activity can be effective in preventing the spread of HIV infection. In countries such as Vietnam and Guyana, where HIV infection has yet to move into or is at low levels in the general population, aggressive prevention strategies among people who engage in high-risk activity are critical to stop the spread of infection; because these individuals often serve as a "bridge" to those at lower risk, they are an essential target group. Such people at high risk, including sex workers and their clients, men who have sex with men, and injecting drug users, are among those who are most marginalized in society and have the least access to basic health care, yet they are often in the greatest need of services.
During the reporting period, the Emergency Plan supported activities that target specific outreach, services, and comprehensive prevention messages directed at ending risky behavior. Strategies included:
- Interpersonal approaches to behavior change, such as counseling, mentoring, and peer outreach
- Community and workplace interventions to eliminate or reduce risky behaviors
- Initiatives to promote the use of testing and counseling services, including developing innovative strategies to encourage and increase HIV testing, such as provider-initiated voluntary testing where appropriate
- Promoting and supporting substance abuse prevention and treatment targeting HIV-positive individuals
- Promoting a comprehensive package for sex workers and other high-risk groups, including HIV counseling and testing, STI screening and treatment, targeted condom promotion and distribution, and other risk reduction education
- Promoting correct and consistent condom use during high-risk sexual activity
- Media interventions with specially tailored messages appropriately targeted to specific populations
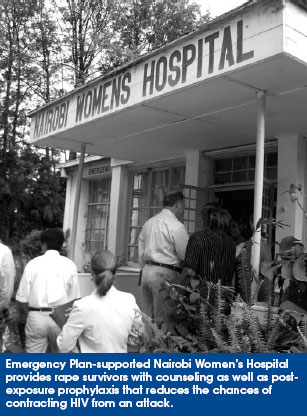
- Addressing sexual coercion and exploitation of young people and women, including providing psychosocial and other assistance (such as post-exposure HIV prophylaxis for rape victims) for victims of sexual abuse
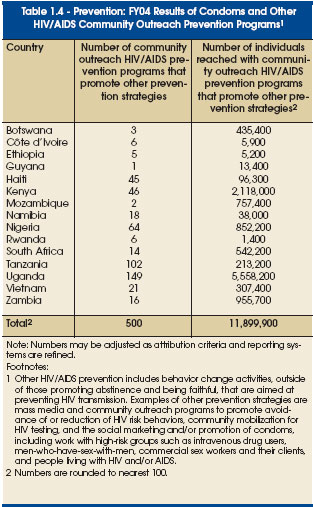
During the reporting period, the Emergency Plan committed $40,518,000 to programs and services that rely on a range of prevention strategies intended to reach people who engage in high-risk sexual activities. These funds supported 500 community outreach programs targeting people engaging in high-risk activity, reaching almost 12 million people. In addition, 200 media campaigns that included a range of prevention messages reached approximately 76.6 million people.
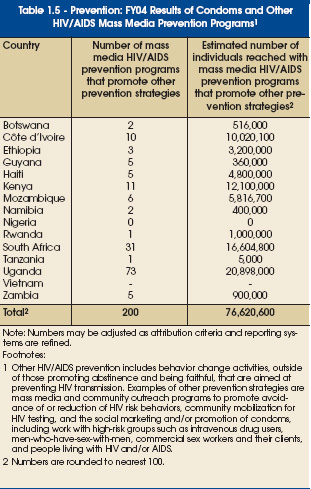 Building on the mechanisms developed to support bilateral programs for reproductive health, the Emergency Plan is now utilizing the Commodity Fund, which was established at the U.S. Agency for International Development (USAID) in fiscal year 2002. This fund has provided between $25 million and $28 million each fiscal year to procure male and female condoms for HIV/AIDS prevention and to ensure their expedited delivery to countries. By procuring condoms centrally, low prices and economies of scale are achieved. In fiscal year 2004, close to 96 million condoms were purchased and shipped to Emergency Plan focus countries through this mechanism. In addition to the Commodity Fund mechanism, many focus country programs have other long-standing condom supply arrangements and distribution mechanisms that are also supported by the U.S. Government, including assistance to host-country governments and other partners. Through these mechanisms, the Emergency Plan contributed to the distribution of more than 340 million additional condoms in the focus countries. Building on the mechanisms developed to support bilateral programs for reproductive health, the Emergency Plan is now utilizing the Commodity Fund, which was established at the U.S. Agency for International Development (USAID) in fiscal year 2002. This fund has provided between $25 million and $28 million each fiscal year to procure male and female condoms for HIV/AIDS prevention and to ensure their expedited delivery to countries. By procuring condoms centrally, low prices and economies of scale are achieved. In fiscal year 2004, close to 96 million condoms were purchased and shipped to Emergency Plan focus countries through this mechanism. In addition to the Commodity Fund mechanism, many focus country programs have other long-standing condom supply arrangements and distribution mechanisms that are also supported by the U.S. Government, including assistance to host-country governments and other partners. Through these mechanisms, the Emergency Plan contributed to the distribution of more than 340 million additional condoms in the focus countries.
Sustainability: Building Capacity
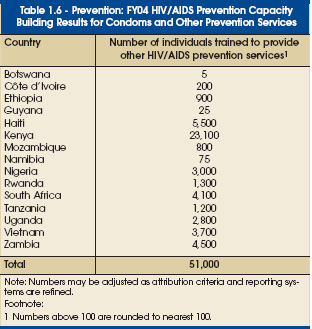
As discussed above, correct and consistent messages are crucial factors in determining the effectiveness of behavior change-oriented prevention strategies. The Emergency Plan has supported extensive training and capacity building of local groups to promote and sustain the use of correct and consistent evidence-based strategies for youth and other unmarried people, sexually active adults, and those who engage in high-risk behaviors. For those who engage in high-risk behaviors, the Emergency Plan trained more than 51,000 individuals to provide prevention services that included information on the correct and consistent use of condoms when appropriate and other risk-reduction strategies.
Key Challenges and Future Directions
A key challenge to delivering comprehensive ABC programs is a lack of well-trained outreach workers and providers. The Emergency Plan is addressing this issue by strengthening and expanding existing networks of public and private services through training and enhanced linkages. More programs are employing the experience and expertise of people living with HIV/AIDS. Additional tools, such as enhanced prevention counseling and improved linkages to care, are required to help discordant couples protect themselves. There will be continued emphasis on improving prevention services for vulnerable girls and young women and on scaling up prevention for HIV-positive people.
In July 2004, Vietnam was selected as the 15th Emergency Plan focus country. People who engage in injecting drug use are an important population at risk for acquiring or transmitting HIV infection in Vietnam. Another challenge to the existing Plan strategy is to develop policies and programs for substance users. In the next funding cycle, the Emergency Plan will seek to support comprehensive HIV prevention and care programs for injecting drug users. Emergency Plan funds will not support needle or syringe exchange. The Plan will work to develop multicomponent HIV prevention programs that include outreach; risk reduction counseling and prevention education for substance abusers; HIV counseling and testing in substance abuse programs; HIV treatment or referral for HIV-positive substance users; and medica-tion-assisted treatment of addiction.
![[boxed text] Increasing HIV/AIDS Awareness Through Bold Leadership](https://webarchive.library.unt.edu/eot2008/20081107002934im_/http://www.state.gov/cms_images/aids_awareness.jpg)
Prevention of Mother-to-Child Transmission
 Results: Rapid Scale-Up Results: Rapid Scale-Up
The prevention of mother-to-child transmission (PMTCT) remains a high-priority intervention under the Emergency Plan. Prior to the President’s Mother and Child HIV Prevention Initiative, fewer than 4 percent of HIV-positive pregnant women had access to antiretroviral drugs to prevent HIV transmission to their infants.
In fiscal year 2004, total PMTCT obligations in focus countries exceeded $50 million. The Emergency Plan works to expand access to comprehensive programs that offer HIV testing for pregnant women, prevention interventions for those who are HIV-negative, and medical support for those who are HIV-positive. The primary goal of these programs is to prevent transmission of HIV during pregnancy through the provision of a minimum package of services that includes counseling and testing for pregnant women; antiretroviral prophylaxis to prevent mother-to-child transmission; counseling and support for safe infant feeding practices; family planning counseling or referral; and referral for HIV/AIDS treatment. In fiscal year 2004, the Emergency Plan supported PMTCT services under national strategies for 1,271,400 women, of whom 125,100 received mostly short-course antiretroviral preventive therapy, averting an estimated 23,766 infections of newborns. As impressive as these results are, there are also multiple other benefits of PMTCT programs not reflected in these data. As a venue for HIV counseling and testing, 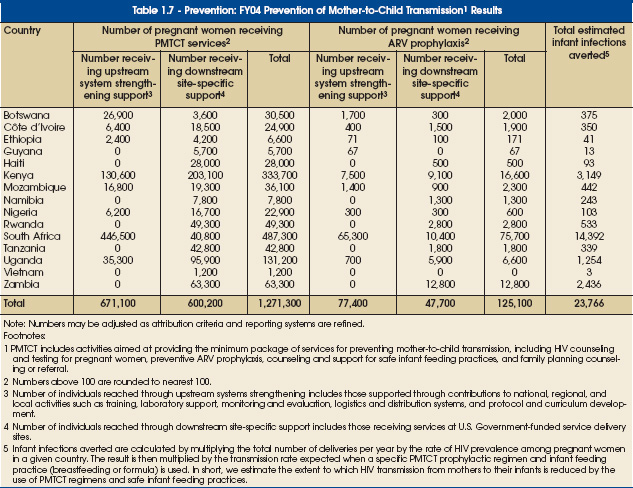
PMTCT programs provide an important opportunity for women who are HIV-negative to learn strategies to remain negative. In addition, thanks to the strong linkages being developed through the Emergency Plan, not only are infections in infants prevented, but also mothers and fathers who need care and support are brought into long-term antiretroviral treatment (ART) programs, thus helping to prevent a new generation from being orphaned.
Sustainability: Building Capacity
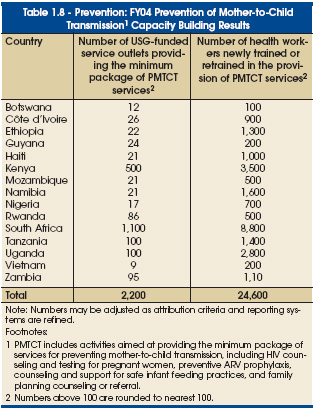
During the reporting period, the Emergency Plan made important progress in strengthening the capacity of national governments to comprehensively serve pregnant women and to implement and manage the distribution and logistics systems essential for PMTCT programs. In addition, the Plan provided support to ensure that host country personnel were trained in both the delivery and management of these programs. During fiscal year 2004, the Emergency Plan supported training of 24,600 health workers in the provision of PMTCT services and supported 2,200 service outlets that provide the minimum package of PMTCT services.
Key Challenges and Future Directions
The establishment of effective PMTCT programs in resource-limited settings has required addressing a range of challenges, including developing and implementing models of HIV primary care services focused on women and families that can be easily adapted and widely replicated; implementing reliable systems for the regular supply of pharmaceuticals and testing supplies; ensuring appropriate patient monitoring in settings where access to laboratory services is limited; developing simple, comprehensive training strategies for health care providers; and developing effective, locally appropriate strategies to encourage treatment adherence.
The President’s Emergency Plan will continue to address the ongoing challenges in PMTCT programs, including the stigma of HIV, which poses a barrier to service and increasing access; the failure of women to return for HIV test results where rapid testing is not available; low acceptance of ART offered to HIV-positive women at antenatal clinics; poor adherence to "take home" ART for mothers and newborns by HIV-positive mothers; and low acceptance of recommended infant feeding behaviors to minimize mother-to-child transmission. Additionally, there is a need to address the difficult issues of reaching women who deliver at home and ensure referrals to treatment for mothers and children who need it. As the Emergency Plan moves forward, the PMTCT program will seek to address these barriers and to expand to new sites, especially rural health care sites and settings with limited health systems infrastructure.
Prevention of Medical Transmission of HIV
 Results: Rapid Scale-Up Results: Rapid Scale-Up
Throughout the developing world people still acquire HIV through blood transfusions and unsafe medical injections. The Emergency Plan supports host-country efforts to improve the quality of their blood supply, introduce practices that prevent transmission through unsafe injections, and improve infection prevention. In addition, health workers exposed to blood during their daily work need training in universal medical precautions to avoid exposure to bloodborne infections. The Plan works closely with national governments to support policies, infrastructure, commodity procurement, and management capacity to ensure a safe and adequate blood supply.
Similar support is provided for medical injection safety. The safe injection initiative includes two components — decreasing unnecessary injections and making injections safer. Specific activities include support of distribution supply chain logistics, appropriate disposal of injection equipment and other related equipment and supplies, and training in universal medical precautions. Currently, 14 focus countries have developed national injection safety strategic plans, and nine have established national injection safety advisory groups.
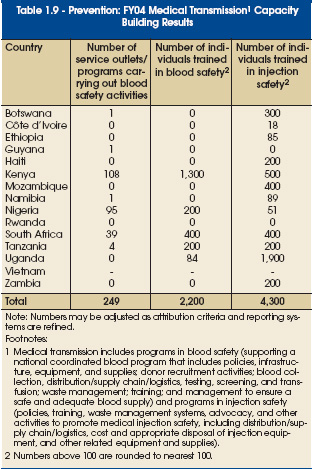
 Activities for preventing medical transmission are based on plans that can adapt to a country’s specific needs. For example, some countries conducted needs assessments in 2004 to identify a strategy for improving their national blood safety and injection safety programs. Other countries had already conducted appropriate assessments and were ready to begin training for health care workers, commodity procurement, and improving systems for the prevention of medical transmission. In the Emergency Plan’s first eight months, 2,200 individuals were trained in safe blood techniques and 4,300 in injection safety. Additionally, almost 250 programs funded by the Emergency Plan focused on blood safety activities. Activities for preventing medical transmission are based on plans that can adapt to a country’s specific needs. For example, some countries conducted needs assessments in 2004 to identify a strategy for improving their national blood safety and injection safety programs. Other countries had already conducted appropriate assessments and were ready to begin training for health care workers, commodity procurement, and improving systems for the prevention of medical transmission. In the Emergency Plan’s first eight months, 2,200 individuals were trained in safe blood techniques and 4,300 in injection safety. Additionally, almost 250 programs funded by the Emergency Plan focused on blood safety activities.
The total budget for medical transmission prevention activities was $51,955,000.
Sustainability: Building Capacity
The Emergency Plan for AIDS Relief made progress during the reporting period in strengthening the capacity of national governments to implement and manage the distribution and logistics systems essential for effective blood safety, medical injection safety, and condom programs. In addition, support was provided to ensure that host-country personnel were trained in the delivery and management of these programs.
Key Challenges and Future Directions
 As with other approaches to prevention, a key challenge in delivering blood safety and safe injection programs is a lack of well-trained personnel. This issue is being addressed by providing training on infection control, universal medical precautions, and safe injection and blood safety techniques to new health care workers before they enter the workforce, while certification programs and on-the-job training are provided for current health care workers. Consistent and secure supply chains for health care commodities and medications are an additional challenge. Through an announced request for applications, the Emergency Plan will provide technical assistance to countries to strengthen existing supply chains, develop new supply chains, provide bulk purchasing at a reduced price, and accurately forecast procurement needs. As with other approaches to prevention, a key challenge in delivering blood safety and safe injection programs is a lack of well-trained personnel. This issue is being addressed by providing training on infection control, universal medical precautions, and safe injection and blood safety techniques to new health care workers before they enter the workforce, while certification programs and on-the-job training are provided for current health care workers. Consistent and secure supply chains for health care commodities and medications are an additional challenge. Through an announced request for applications, the Emergency Plan will provide technical assistance to countries to strengthen existing supply chains, develop new supply chains, provide bulk purchasing at a reduced price, and accurately forecast procurement needs.
Accountability: Reporting on the Components of Prevention
To account for Emergency Plan prevention programming, in-country teams total all of the programs, services, and activities aimed at preventing HIV transmission. This includes mass media and community outreach programs to promote abstinence, faithfulness, correct and consistent condom use, and other behavior change to support avoidance of or reduction of HIV risk behaviors; community mobilization for HIV testing; and preventing mother-to-child transmission and medical transmission (blood safety and injection safety). These indicator data are drawn from country program reports collected in-country from partners with guidance from the Office of the U.S. Global AIDS Coordinator. Condom shipments are tracked by a central database within the U.S. Government.
To account for programs addressing medically transmitted HIV, country teams identify programs that support a national blood program that includes policies, infrastructure, equipment, and supplies; donor recruitment activities; blood collection, distribution and supply chain logistics, testing, screening, and transfusion; waste management; training; and management to ensure a safe and adequate blood supply. In addition, they identify policies, training, waste management systems, advocacy, and other activities that promote medical injection safety, including distribution and supply chain logistics, cost, and appropriate disposal of injection equipment, and other related equipment and supplies.
 Country teams monitor activities aimed at providing the minimum package of PMTCT services for preventing mother-to-child transmission, including counseling and testing for pregnant women; preventive antiretroviral prophylaxis; counseling and support for safe infant feeding practices; and family planning counseling or referral. These data are drawn from program reports and health management information systems. Country teams monitor activities aimed at providing the minimum package of PMTCT services for preventing mother-to-child transmission, including counseling and testing for pregnant women; preventive antiretroviral prophylaxis; counseling and support for safe infant feeding practices; and family planning counseling or referral. These data are drawn from program reports and health management information systems.
Currently, significant gaps exist in the evidence base for determining the impact of HIV prevention efforts and their effect on country epidemic trajectories. Services provided and people reached through activities do not provide sufficient data to predict the number of infections averted. The number of infections averted as a result of expanded programs must be estimated through modeling since it is impossible to measure directly (by definition, it is a non-event). To provide as much accountability as possible, the Emergency Plan will estimate infections averted based on periodic prevalence studies, with the U.S. Census Bureau taking the lead on progress toward the goal of 7 million HIV infections averted by 2010 in the focus countries. The modeling approach will establish prevalence trends for each country using data through 2003. In 2005, these prevalence trends will be re-estimated for those countries with additional surveillance data available for 2004 and 2005. The difference in these two prevalence trends will represent the net impact of program activities since the start of the Emergency Plan. During the five years of the Emergency Plan, each focus country will have a number of assessments at strategic intervals; infections averted will be estimated following those assessments.
|



