| U.S. Department of Labor | |
|||||
| Occupational Safety & Health Administration | ||||||
|
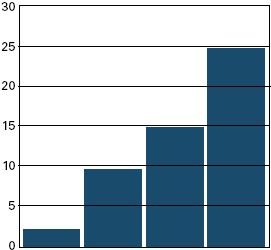
Guidelines for Preventing Workplace Violence for Health Care & Social Service Workers U.S. Department of Labor Occupational Safety and Health Administration OSHA 3148-01R 2004 www.osha.gov This informational booklet provides a general overview of a particular topic related to OSHA standards. It does not alter or determine compliance responsibilities in OSHA standards or the Occupational Safety and Health Act of 1970. Because interpretations and enforcement policy may change over time, you should consult current OSHA administrative interpretations and decisions by the Occupational Safety and Health Review Commission and the Courts for additional guidance on OSHA compliance requirements. This publication is in the public domain and may be reproduced, fully or partially, without permission. Source credit is requested but not required. This information is available to sensory impaired individuals upon request. Voice phone: (202) 693-1999; teletypewriter (TTY) number: (877) 889-5627. Contents Notice Acknowledgments Introduction Overview of Guidelines Violence Prevention Programs Management Commitment and Employee Involvement Worksite Analysis Hazard Prevention and Control Safety and Health Training Recordkeeping and Program Evaluation Conclusion References OSHA assistance Safety and Health Program Management Guidelines State Programs Consultation Services Voluntary Protection Programs (VPP) Strategic Partnership Program Alliance Programs OSHA Training and Education Information Available Electronically OSHA Publications Contacting OSHA OSHA Regional Offices Appendices Appendix A: Workplace Violence Program Checklists Appendix B: Violence Incident Report Forms Appendix C: Suggested Readings Notice These guidelines are not a new standard or regulation. They are advisory in nature, informational in content and intended to help employers establish effective workplace violence prevention programs adapted to their specific worksites. The guidelines do not address issues related to patient care. They are performance-oriented, and how employers implement them will vary based on the site's hazard analysis. Violence inflicted on employees may come from many sources— external parties such as robbers or muggers and internal parties such as coworkers and patients. These guidelines address only the violence inflicted by patients or clients against staff. However, OSHA suggests that workplace violence policies indicate a zero-tolerance for all forms of violence from all sources. The Occupational Safety and Health Act of 1970 (OSH Act)(1) mandates that, in addition to compliance with hazard-specific standards, all employers have a general duty to provide their employees with a workplace free from recognized hazards likely to cause death or serious physical harm. OSHA will rely on Section 5(a)(1) of the OSH Act, the "General Duty Clause,"(2) for enforcement authority. Failure to implement these guidelines is not in itself a violation of the General Duty Clause. However, employers can be cited for violating the General Duty Clause if there is a recognized hazard of workplace violence in their establishments and they do nothing to prevent or abate it. When Congress passed the OSH Act, it recognized that workers' compensation systems provided state-specific remedies for job-related injuries and illnesses. Determining what constitutes a compensable claim and the rate of compensation were left to the states, their legislatures and their courts. Congress acknowledged this point in Section 4(b)(4) of the OSH Act, when it stated categorically: "Nothing in this chapter shall be construed to supersede or in any manner affect any workmen's compensation law. . .."(3) Therefore, these non-mandatory guidelines should not be viewed as enlarging or diminishing the scope of work-related injuries. The guidelines are intended for use in any state and without regard to whether any injuries or fatalities are later determined to be compensable. Acknowledgments Many people have contributed to these guidelines. They include health care, social service and employee assistance experts; researchers; educators; unions and other stakeholders; OSHA professionals; and the National Institute for Occupational Safety and Health (NIOSH). Also, several states have developed relevant standards or recommendations, such as California OSHA's CAL/OSHA Guidelines for Workplace Security and Guidelines for Security and Safety of Health Care and Community Service Workers; New Jersey Public Employees Occupational Safety and Health's Guidelines on Measures and Safeguards in Dealing with Violent or Aggressive Behavior in Public Sector Health Care Facilities; and the State of Washington Department of Labor and Industries' Violence in Washington Workplaces and Study of Assaults on Staff in Washington State Psychiatric Hospitals. Other organizations with relevant recommendations include the Joint Commission on Accreditation of Health Care Organizations' Comprehensive Accreditation Manuals for Hospitals, the Metropolitan Chicago Healthcare Council's Guidelines for Dealing with Violence in Health Care, and the American Nurses Association's Promoting Safe Work Environments for Nurses. These and other agencies have information available to assist employers. Introduction Workplace violence affects health care and social service workers. The National Institute for Occupational Safety and Health (NIOSH) defines workplace violence as "violent acts (including physical assaults and threats of assaults) directed toward persons at work or on duty."(4) This includes terrorism as illustrated by the terrorist acts of September 11, 2001 that resulted in the deaths of 2,886 workers in New York, Virginia and Pennsylvania. Although these guidelines do not address terrorism specifically, this type of violence remains a threat to U.S. workplaces. For many years, health care and social service workers have faced a significant risk of job-related violence. Assaults represent a serious safety and health hazard within these industries. OSHA's violence prevention guidelines provide the agency's recommendations for reducing workplace violence, developed following a careful review of workplace violence studies, public and private violence prevention programs and input from stakeholders. OSHA encourages employers to establish violence prevention programs and to track their progress in reducing work-related assaults. Although not every incident can be prevented, many can, and the severity of injuries sustained by employees can be reduced. Adopting practical measures such as those outlined here can significantly reduce this serious threat to worker safety. Extent of the problem The Bureau of Labor Statistics (BLS) reports that there were 69 homicides in the health services from 1996 to 2000. Although workplace homicides may attract more attention, the vast majority of workplace violence consists of non-fatal assaults. BLS data shows that in 2000, 48 percent of all non-fatal injuries from occupational assaults and violent acts occurred in health care and social services. Most of these occurred in hospitals, nursing and personal care facilities, and residential care services. Nurses, aides, orderlies and attendants suffered the most non-fatal assaults resulting in injury. Injury rates also reveal that health care and social service workers are at high risk of violent assault at work. BLS rates measure the number of events per 10,000 full-time workers—in this case, assaults resulting in injury. In 2000, health service workers overall had an incidence rate of 9.3 for injuries resulting from assaults and violent acts. The rate for social service workers was 15, and for nursing and personal care facility workers, 25. This compares to an overall private sector injury rate of 2. The Department of Justice's (DOJ) National Crime Victimization Survey for 1993 to 1999 lists average annual rates of non-fatal violent crime by occupation. The average annual rate for non-fatal violent crime for all occupations is 12.6 per 1,000 workers. The average annual rate for physicians is 16.2; for nurses, 21.9; for mental health professionals, 68.2; and for mental health custodial workers, 69. (Note: These data do not compare directly to the BLS figures because DOJ presents violent incidents per 1,000 workers and BLS displays injuries involving days away from work per 10,000 workers. Both sources, however, reveal the same high risk for health care and soical service workers.) As significant as these numbers are, the actual number of incidents is probably much higher. Incidents of violence are likely to be underreported, perhaps due in part to the persistent perception within the health care industry that assaults are part of the job. Underreporting may reflect a lack of institutional reporting policies, employee beliefs that reporting will not benefit them or employee fears that employers may deem assaults the result of employee negligence or poor job performance.
The risk factors Health care and social service workers face an increased risk of work-related assaults stemming from several factors. These include:
In January 1989, OSHA published voluntary, generic safety and health program management guidelines for all employers to use as a foundation for their safety and health programs, which can include workplace violence prevention programs.(5) OSHA's violence prevention guidelines build on these generic guidelines by identifying common risk factors and describing some feasible solutions. Although not exhaustive, the workplace violence guidelines include policy recommendations and practical corrective methods to help prevent and mitigate the effects of workplace violence. The goal is to eliminate or reduce worker exposure to conditions that lead to death or injury from violence by implementing effective security devices and administrative work practices, among other control measures. The guidelines cover a broad spectrum of workers who provide health care and social services in psychiatric facilities, hospital emergency departments, community mental health clinics, drug abuse treatment clinics, pharmacies, community-care facilities and long-term care facilities. They include physicians, registered nurses, pharmacists, nurse practitioners, physicians' assistants, nurses' aides, therapists, technicians, public health nurses, home health care workers, social workers, welfare workers and emergency medical care personnel. The guidelines may also be useful in reducing risks for ancillary personnel such as maintenance, dietary, clerical and security staff in the health care and social service industries. Violence Prevention Programs A written program for job safety and security, incorporated into the organization's overall safety and health program, offers an effective approach for larger organizations. In smaller establishments, the program does not need to be written or heavily documented to be satisfactory. What is needed are clear goals and objectives to prevent workplace violence suitable for the size and complexity of the workplace operation and adaptable to specific situations in each establishment. Employers should communicate information about the prevention program and startup date to all employees. At a minimum, workplace violence prevention programs should:
The five main components of any effective safety and health program also apply to the prevention of workplace violence:
Management commitment and employee involvement are complementary and essential elements of an effective safety and health program. To ensure an effective program, management and frontline employees must work together, perhaps through a team or committee approach. If employers opt for this strategy, they must be careful to comply with the applicable provisions of the National Labor Relations Act.(7) Management commitment, including the endorsement and visible involvement of top management, provides the motivation and resources to deal effectively with workplace violence. This commitment should include:
Employee involvement should include:
Value of a worksite analysis A worksite analysis involves a step-by-step, commonsense look at the workplace to find existing or potential hazards for workplace violence. This entails reviewing specific procedures or operations that contribute to hazards and specific areas where hazards may develop. A threat assessment team, patient assault team, similar task force or coordinator may assess the vulnerability to workplace violence and determine the appropriate preventive actions to be taken. This group may also be responsible for implementing the workplace violence prevention program. The team should include representatives from senior management, operations, employee assistance, security, occupational safety and health, legal and human resources staff. The team or coordinator can review injury and illness records and workers' compensation claims to identify patterns of assaults that could be prevented by workplace adaptation, procedural changes or employee training. As the team or coordinator identifies appropriate controls, they should be instituted. Focus of a worksite analysis The recommended program for worksite analysis includes, but is not limited to:
This activity should include reviewing medical, safety, workers' compensation and insurance records—including the OSHA Log of Work-Related Injury and Illness (OSHA Form 300), if the employer is required to maintain one—to pinpoint instances of workplace violence. Scan unit logs and employee and police reports of incidents or near-incidents of assaultive behavior to identify and analyze trends in assaults relative to particular:
Value of screening surveys One important screening tool is an employee questionnaire or survey to get employees' ideas on the potential for violent incidents and to identify or confirm the need for improved security measures. Detailed baseline screening surveys can help pinpoint tasks that put employees at risk. Periodic surveys—conducted at least annually or whenever operations change or incidents of workplace violence occur—help identify new or previously unnoticed risk factors and deficiencies or failures in work practices, procedures or controls. Also, the surveys help assess the effects of changes in the work processes. The periodic review process should also include feedback and follow-up. Independent reviewers, such as safety and health professionals, law enforcement or security specialists and insurance safety auditors, may offer advice to strengthen programs. These experts can also provide fresh perspectives to improve a violence prevention program. Conducting a workplace security analysis The team or coordinator should periodically inspect the workplace and evaluate employee tasks to identify hazards, conditions, operations and situations that could lead to violence. To find areas requiring further evaluation, the team or coordinator should:
After hazards are identified through the systematic worksite analysis, the next step is to design measures through engineering or administrative and work practices to prevent or control these hazards. If violence does occur, post-incident response can be an important tool in preventing future incidents. Engineering controls and workplace adaptations to minimize risk Engineering controls remove the hazard from the workplace or create a barrier between the worker and the hazard. There are several measures that can effectively prevent or control workplace hazards, such as those described in the following paragraphs. The selection of any measure, of course, should be based on the hazards identified in the workplace security analysis of each facility. Among other options, employers may choose to:
Administrative and work practice controls affect the way staff perform jobs or tasks. Changes in work practices and administrative procedures can help prevent violent incidents. Some options for employers are to:
Post-incident response and evaluation are essential to an effective violence prevention program. All workplace violence programs should provide comprehensive treatment for employees who are victimized personally or may be traumatized by witnessing a workplace violence incident. Injured staff should receive prompt treatment and psychological evaluation whenever an assault takes place, regardless of its severity. Provide the injured transportation to medical care if it is not available onsite. Victims of workplace violence suffer a variety of consequences in addition to their actual physical injuries. These may include:
Several types of assistance can be incorporated into the post-incident response. For example, trauma-crisis counseling, critical-incident stress debriefing or employee assistance programs may be provided to assist victims. Certified employee assistance professionals, psychologists, psychiatrists, clinical nurse specialists or social workers may provide this counseling or the employer may refer staff victims to an outside specialist. In addition, the employer may establish an employee counseling service, peer counseling or support groups. Counselors should be well trained and have a good understanding of the issues and consequences of assaults and other aggressive, violent behavior. Appropriate and promptly rendered post-incident debriefings and counseling reduce acute psychological trauma and general stress levels among victims and witnesses. In addition, this type of counseling educates staff about workplace violence and positively influences workplace and organizational cultural norms to reduce trauma associated with future incidents. Safety and Health Training Training and education ensure that all staff are aware of potential security hazards and how to protect themselves and their coworkers through established policies and procedures. Training for all employees Every employee should understand the concept of "universal precautions for violence"— that is, that violence should be expected but can be avoided or mitigated through preparation. Frequent training also can reduce the likelihood of being assaulted. Employees who may face safety and security hazards should receive formal instruction on the specific hazards associated with the unit or job and facility. This includes information on the types of injuries or problems identified in the facility and the methods to control the specific hazards. It also includes instructions to limit physical interventions in workplace altercations whenever possible, unless enough staff or emergency response teams and security personnel are available. In addition, all employees should be trained to behave compassionately toward coworkers when an incident occurs. The training program should involve all employees, including supervisors and managers. New and reassigned employees should receive an initial orientation before being assigned their job duties. Visiting staff, such as physicians, should receive the same training as permanent staff. Qualified trainers should instruct at the comprehension level appropriate for the staff. Effective training programs should involve role playing, simulations and drills. Topics may include management of assaultive behavior, professional assault-response training, police assault-avoidance programs or personal safety training such as how to prevent and avoid assaults. A combination of training programs may be used, depending on the severity of the risk. Employees should receive required training annually. In large institutions, refresher programs may be needed more frequently, perhaps monthly or quarterly, to effectively reach and inform all employees. What training should cover The training should cover topics such as:
Supervisors and managers need to learn to recognize high-risk situations, so they can ensure that employees are not placed in assignments that compromise their safety. They also need training to ensure that they encourage employees to report incidents. Supervisors and managers should learn how to reduce security hazards and ensure that employees receive appropriate training. Following training, supervisors and managers should be able to recognize a potentially hazardous situation and to make any necessary changes in the physical plant, patient care treatment program and staffing policy and procedures to reduce or eliminate the hazards. Training for security personnel Security personnel need specific training from the hospital or clinic, including the psychological components of handling aggressive and abusive clients, types of disorders and ways to handle aggression and defuse hostile situations. The training program should also include an evaluation. At least annually, the team or coordinator responsible for the program should review its content, methods and the frequency of training. Program evaluation may involve supervisor and employee interviews, testing and observing and reviewing reports of behavior of individuals in threatening situations. Recordkeeping and Program Evaluation How employers can determine program effectiveness Recordkeeping and evaluation of the violence prevention program are necessary to determine its overall effectiveness and identify any deficiencies or changes that should be made. Records employers should keep Recordkeeping is essential to the program's success. Good records help employers determine the severity of the problem, evaluate methods of hazard control and identify training needs. Records can be especially useful to large organizations and for members of a business group or trade association who "pool" data. Records of injuries, illnesses, accidents, assaults, hazards, corrective actions, patient histories and training can help identify problems and solutions for an effective program. Important Records:
As part of their overall program, employers should evaluate their safety and security measures. Top management should review the program regularly, and with each incident, to evaluate its success. Responsible parties (including managers, supervisors and employees) should reevaluate policies and procedures on a regular basis to identify deficiencies and take corrective action. Management should share workplace violence prevention evaluation reports with all employees. Any changes in the program should be discussed at regular meetings of the safety committee, union representatives or other employee groups. All reports should protect employee confidentiality either by presenting only aggregate data or by removing personal identifiers if individual data are used. Processes involved in an evaluation include:
Employers who would like help in implementing an appropriate workplace violence prevention program can turn to the OSHA Consultation Service provided in their State. To contact this service, see OSHA's website at www.osha.gov or call (800) 321-OSHA. OSHA's efforts to help employers combat workplace violence are complemented by those of NIOSH, public safety officials, trade associations, unions, insurers and human resource and employee assistance professionals, as well as other interested groups. Employers and employees may contact these groups for additional advice and information. NIOSH can be reached toll-free at (800) 35-NIOSH. Conclusion OSHA recognizes the importance of effective safety and health program management in providing safe and healthful workplaces. Effective safety and health programs improve both morale and productivity and reduce workers' compensation costs. OSHA's violence prevention guidelines are an essential component of workplace safety and health programs. OSHA believes the performance-oriented approach of these guidelines provides employers with flexibility in their efforts to maintain safe and healthful working conditions. References California State Department of Industrial Relations, Cal/OSHA. (1998). Guidelines for Security and Safety of Health Care and Community Service Workers. www.dir.ca.gov/dosh/dosh%5Fpublications/hcworker.html Centers for Disease Control and Prevention, National Institute for Occupational Health. (2002). Occupational Hazards in Hospitals. DHHS (NIOSH) Pub. No. 2002-101. www.cdc.gov/niosh/2002-101.html U.S. Department of Justice, Bureau of Justice Statistics. (2001). National Crime Victimization Survey. Violence in the Workplace, 1993-99. www.ojp.gov/bjs/pub/pdf/vw99.pdf U.S. Department of Labor, Bureau of Labor Statistics. (2002). Census of Fatal Occupational Injuries, 2001. www.bls.gov/iif/oshwc/cfoi/cfnr0008.pdf U.S. Department of Labor, Bureau of Labor Statistics. (2001). Survey of Occupational Injuries and Illnesses, 2000. www.bls.gov/iif/oshwc/osh/os/osnr0013.pdf Washington, Department of Labor and Industries. Workplace Violence: Awareness and Prevention for Employers and Employees, 2000. www.lni.wa.gov/ipub/417-140-000.htm OSHA assistance OSHA can provide extensive help through a variety of programs, including technical assistance about effective safety and health programs, state plans, workplace consultations, voluntary protection programs, strategic partnerships, training and education and more. An overall commitment to workplace safety and health can add value to your business, to your workplace and to your life. Safety and Health Program Management Guidelines Effective management of worker safety and health protection is a decisive factor in reducing the extent and severity of work-related injuries and illnesses and their related costs. In fact, an effective safety and health program forms the basis of good worker protection and can save time and money (about $4 for every dollar spent) and increase productivity and reduce worker injuries, illnesses and related workers' compensation costs. To assist employers and employees in developing effective safety and health programs, OSHA published recommended Safety and Health Program Management Guidelines(54 Federal Register (16): 3904-3916, January 26, 1989). These voluntary guidelines apply to all places of employment covered by OSHA. The guidelines identify four general elements critical to the development of a successful safety and health management program:
The Occupational Safety and Health Act of 1970(OSH Act) encourages states to develop and operate their own job safety and health plans. OSHA approves and monitors these plans. There are currently 26 state plans: 23 cover both private and public (state and local government) employment; 3 states, Connecticut, New Jersey and New York, cover the public sector only. States and territories with their own OSHA-approved occupational safety and health plans must adopt standards identical to, or at least as effective as, the federal standards. Consultation Services Consultation assistance is available on request to employers who want help in establishing and maintaining a safe and healthful workplace. Largely funded by OSHA, the service is provided at no cost to the employer. Primarily developed for smaller employers with more hazardous operations, the consultation service is delivered by state governments employing professional safety and health consultants. Comprehensive assistance includes an appraisal of all-mechanical systems, work practices and occupational safety and health hazards of the workplace and all aspects of the employer's present job safety and health program. In addition, the service offers assistance to employers in developing and implementing an effective safety and health program. No penalties are proposed or citations issued for hazards identified by the consultant. OSHA provides consultation assistance to the employer with the assurance that his or her name and firm and any information about the workplace will not be routinely reported to OSHA enforcement staff. Under the consultation program, certain exemplary employers may request participation in OSHA's Safety and Health Achievement Recognition Program (SHARP). Eligibility for participation in SHARP includes receiving a comprehensive consultation visit, demonstrating exemplary achievements in workplace safety and health by abating all identified hazards and developing an excellent safety and health program. Employers accepted into SHARP may receive an exemption from programmed inspections (not complaint or accident investigation inspections) for a period of one year. For more information concerning consultation assistance, see the OSHA website at www.osha.gov. Voluntary Protection Programs (VPP) Voluntary Protection Programs and onsite consultation services, when coupled with an effective enforcement program, expand worker protection to help meet the goals of the OSH Act. The three levels of VPP are Star, Merit, and Demonstration designed to recognize outstanding achievements by companies that have successfully incorporated comprehensive safety and health programs into their total management system. The VPPs motivate others to achieve excellent safety and health results in the same outstanding way as they establish a cooperative relationship between employers, employees and OSHA. For additional information on VPP and how to apply, contact the OSHA regional offices listed at the end of this publication. Strategic Partnership Program OSHA's Strategic Partnership Program, the newest member of OSHA's cooperative programs, helps encourage, assist and recognize the efforts of partners to eliminate serious workplace hazards and achieve a high level of worker safety and health. Whereas OSHA's Consultation Program and VPP entail one-on-one relationships between OSHA and individual worksites, most strategic partnerships seek to have a broader impact by building cooperative relationships with groups of employers and employees. These partnerships are voluntary, cooperative relationships between OSHA, employers, employee representatives and others (e.g., trade unions, trade and professional associations, universities and other government agencies). For more information on this and other cooperative programs, contact your nearest OSHA office, or visit OSHA's website at www.osha.gov. Alliance Programs The Alliances Program enables organizations committed to workplace safety and health to collaborate with OSHA to prevent injuries and illnesses in the workplace. OSHA and the Alliance participants work together to reach out to, educate and lead the nation's employers and their employees in improving and advancing workplace safety and health. Alliances are open to all groups, including trade or professional organizations, businesses, labor organizations, educational institutions and government agencies. In some cases, organizations may be building on existing relationships with OSHA that were developed through other cooperative programs. There are few formal program requirements for Alliances and the agreements do not include an enforcement component. However, OSHA and the participating organizations must define, implement and meet a set of short- and long-term goals that fall into three categories: training and education; outreach and communication; and promoting the national dialogue on workplace safety and health. OSHA Training and Education OSHA area offices offer a variety of information services, such as compliance assistance, technical advice, publications, audiovisual aids and speakers for special engagements. OSHA's Training Institute in Arlington Heights, Ill., provides basic and advanced courses in safety and health for federal and state compliance officers, state consultants, federal agency personnel, and private sector employers, employees and their representatives. The OSHA Training Institute also has established OSHA Training Institute Education Centers to address the increased demand for its courses from the private sector and from other federal agencies. These centers are nonprofit colleges, universities and other organizations that have been selected after a competition for participation in the program. OSHA also provides funds to nonprofit organizations, through grants, to conduct workplace training and education in subjects where OSHA believes there is a lack of workplace training. Grants are awarded annually. Grant recipients are expected to contribute 20 percent of the total grant cost. For more information on grants, training and education, contact the OSHA Training Institute, Office of Training and Education, 2020 South Arlington Heights Road, Arlington Heights, IL 60005, (847) 297-4810 or see "Outreach" on OSHA's website at www.osha.gov. For further information on any OSHA program, contact your nearest OSHA area or regional office listed at the end of this publication. Information Available Electronically OSHA has a variety of materials and tools available on its website at www.osha.gov. These include e-Tools such as Expert Advisors, Electronic Compliance Assistance Tools (e-cats), Technical Links; regulations, directives and publications; videos and other information for employers and employees. OSHA's software programs and compliance assistance tools walk you through challenging safety and health issues and common problems to find the best solutions for your workplace. OSHA's CD-ROM includes standards, interpretations, directives and more, and can be purchased on CD-ROM from the U.S. Government Printing Office. To order, write to the Superintendent of Documents, P.O. Box 371954, Pittsburgh, PA 15250-7954 or phone (202) 512-1800, or order online at http://bookstore.gpo.gov. OSHA Publications OSHA has an extensive publications program. For a listing of free or sales items, visit OSHA's website at www.osha.gov or contact the OSHA Publications Office, U.S. Department of Labor, 200 Constitution Avenue, NW, N-3101, Washington, DC 20210. Telephone (202) 693-1888 or fax to (202) 693-2498. Contacting OSHA To report an emergency, file a complaint or seek OSHA advice, assistance or products, call (800) 321-OSHA or contact your nearest OSHA regional or area office listed at the end of this publication. The teletypewriter (TTY) number is (877) 889-5627. You can also file a complaint online and obtain more information on OSHA federal and state programs by visiting OSHA's website at www.osha.gov. OSHA Regional Offices Region I (CT,* ME, MA, NH, RI, VT*) JFK Federal Building, Room E340 Boston, MA 02203 (617) 565-9860 Region II (NJ,* NY,* PR,* VI*) 201 Varick Street, Room 670 New York, NY 10014 (212) 337-2378 Region III (DE, DC, MD,* PA,* VA,* WV) The Curtis Center 170 S. Independence Mall West Suite 740 West Philadelphia, PA 19106-3309 (215) 861-4900 Region IV (AL, FL, GA, KY,* MS, NC,* SC,* TN*) 61 Forsyth Street, SW Atlanta, GA 30303 (404) 562-2300 Region V (IL, IN,* MI,* MN,* OH, WI) 230 South Dearborn Street, Room 3244 Chicago, IL 60604 (312) 353-2220 Region VI (AR, LA, NM,* OK,TX) 525 Griffin Street, Room 602 Dallas, TX 75202 (214) 767-4731 or 4736 x224 Region VII (IA,* KS, MO, NE) City Center Square 1100 Main Street, Suite 800 Kansas City, MO 64105 (816) 426-5861 Region VIII (CO, MT, ND, SD, UT,* WY*) 1999 Broadway, Suite 1690 PO Box 46550 Denver, CO 80201-6550 (303) 844-1600 Region IX (American Samoa, AZ,* CA,* HI, NV,* Northern Mariana Islands) 71 Stevenson Street, Room 420 San Francisco, CA 94105 (415) 975-4310 Region X (AK,* ID, OR,* WA*) 1111 Third Avenue, Suite 715 Seattle, WA 98101-3212 (206) 553-5930 *These states and territories operate their own OSHA-approved job safety and health programs (Connecticut, New Jersey and NewYork plans cover public employees only). States with approved programs must have a standard that is identical to, or at least as effective as, the federal standard. Note: To get contact information for OSHA Area Offices, OSHA-approved State Plans and OSHA Consultation Projects, please visit us online at www.osha.gov or call us at 1-800-321-OSHA. Appendix A: Workplace Violence Program Checklists Reprinted with permission of the American Nurses Association, Promoting Safe Work Environments for Nurses, 2002. Checklist 1: Organizational Assessment Questions Regarding Management Commitment and Employee Involvement
Perform a step-by-step review of each work area to identify specific places and times that violent incidents are occurring and the risk factors that are present. To ensure multiple perspectives, it is best for a team to perform this worksite analysis. Key members of the analysis team should be front-line health care workers, including nurses from each specialty unit, as well as the facility's safety and security professionals. Find Out What's Happening on Paper The first step in this worksite analysis is to obtain and review data that tells the "who, what, when, where and why" about violent incidents. These sources include:
Checklist 2: Analyze Workplace Violence Records
It is important to keep in mind that injuries from violence are often not reported. One of the best ways to observe what is really going on is to conduct a workplace walkthrough. A walkthrough, which is really a workplace inspection, is the first step in identifying violence risk factors and serves several important functions. While on a walkthrough, hazards can be recognized and often corrected before anyone's health and safety is affected. While inspecting for workplace violence risk factors, review the physical facility and note the presence or absence of security measures. Local police may also be able to conduct a security audit or provide information about experience with crime in the area. Ask the Workers A simple survey can provide valuable information often not found in department walkthroughs and injury logs. Some staff may not report violent acts or threatening situations formally but will share the experiences and suggestions anonymously. This can provide information about previously unnoticed deficiencies or failures in work practices or administrative controls. It also can help increase employee awareness about dangerous conditions and encourage them to become involved in prevention activities. Types of questions that employees should be asked include:
Identifying Environmental Risk Factors for Violence Use the following checklist to assist in your workplace walkthrough. General questions about approach:
Assessing the Influence of Day-to-Day Work Practices on Occurrences of Violence
Post-Incident Response
Assessing Employee and Supervisor Training
Recordkeeping and Evaluation Does the violence prevention program provide for:
Appendix B Violence Incident Report Forms Sample 1 The following items serve merely as an example of what might be used or modified by employers in these industries to help prevent workplace violence. (Sample/Draft—Adapt to your own location and business circumstances.) Confidential Incident Report
To: ______________________________ Date of Incident: ______________________________ Location of Incident (Map/sketch on reverse side or attached): ___________________________ ____________________________________________________________________________ From: ___________________ Phone: ________________ Time of Incident: ________________ Nature of the Incident ("X" all applicable boxes): ❑ Assaults or Violent Acts: ____ Type "l" ___ Type "2" ___ Type "3" ___ Other ___ ❑ Preventative or Warning Report ❑ Bomb or Terrorist Type Threat ❑ Yes ❑ No ❑ Transportation Accident ❑ Contacts with Objects or Equipment ❑ Falls ❑ Exposures ❑ Fires or Explosions ❑ Other Legal Counsel Advised of Incident? ❑ Yes ❑ No EAP Advised? ❑ Yes ❑ No Warning or Preventative Measures? ❑ Yes ❑ No Number of Persons Affected: ____________________________ (For each person, complete a report; however, to the extent facts are duplicative, any person's report may incorporate another person's report.) Name of Affected Person(s): __________________ Service Date: __________ Position: ___________ Member of Labor Organization? ❑ Yes ❑ No Supervisor: __________________ Has Supervisor Been Notified? ❑ Yes ❑ No Family: _____________________ Has Been Notified by: ? ❑ Yes ❑ No Lost Work Time? ❑ Yes ❑ No Anticipated Return to Work: ____________________ Third parties or non-employee involvement (include contractor and lease employees, visitors, vendors, customers)? ❑ Yes ❑ No Nature of the Incident Briefly describe: (1) event(s); (2) witnesses with addresses and status included; (3) location details; (4) equipment/weapon details; (5) weather; (6) other records of the incident (e.g., police report, recordings, videos); (7) the ability to observe and reliability of witnesses; (8) were the parties possibly impaired because of illness, injury, drugs or alcohol? (were tests taken to verify same?); (9) parties notified internally (employee relations, medical, legal, operations, etc.) and externally (police, fire, ambulance, EAP, family, etc.). Previous or Related Incidents of This Type? ❑ Yes ❑ No Or by This Person? ❑ Yes ❑ No Preventative Steps? ❑ Yes ❑ No OSHA Log or Other OSHA Action Required? ❑ Yes ❑ No Incident Response Team: _____________________________ Team Leader: ___________________________ __________________ Signature Date Source: Reprinted with permission of Karen Smith Keinbaum, Esq., Counsel to the Law Firm of Abbott, Nicholson, Quilter, Esshaki & Youngblood, P. C., Detroit, MI. Sample 2 The following items serve merely as an example of what might be used or modified by employers in these industries to help prevent workplace violence. A reportable violent incident should be defined as any threatening remark or overt act of physical violence against a person(s) or property whether reported or observed. 1. Date: Day of Week: Time: Assailant: ❑ Female ❑ Male 2. Specific Location: ___________________________________ 3.Violence Directed Toward: ❑ Patient ❑ Staff ❑ Visitor ❑ Other Assailant: ❑ Patient ❑ Staff ❑ Visitor ❑ Other Assailant's Name: ______________________________________ Assailant: ❑ Unarmed ❑ Armed (weapon) 4. Predisposing Factors: ❑ Intoxication ❑ Dissatisfied with Care/Waiting Time ❑ Grief Reaction ❑ Prior History of Violence ❑ Gang Related ❑ Other (Describe) _________ 5. Description of Incident: ❑ Physical Abuse ❑ Verbal Abuse ❑ Other 6. Injuries: ❑ Yes ❑ No 7. Extent of Injuries: _____________________________________ 8. Detailed Description of the Incident: ______________________ 9. Did Any Person Leave the Area because of Incident? ❑ Yes ❑ No ❑ Unable to Determine 10. Present at Time of Incident: ❑ Police Name of Department: _______________________________ ❑ Hospital Security Officer 11. Needed to Call: ❑ Police Name of Department: _______________________________ ❑ Hospital Security 12.Termination of Incident: Incident Diffused ❑ Yes ❑ No Police Notified ❑ Yes ❑ No Assailant Arrested ❑ Yes ❑ No 13. Disposition of Assailant: ❑ Stayed on Premises ❑ Escorted off Premises ❑ Left on Own ❑ Other 14. Restraints Used: ❑ Yes ❑ No Type: _____________________ 15. Report Completed By: ________________ Title: ___________ Witnesses: _____________________________________________ Supervisor Notified: ___________________ Time: _______________ Please put additional comments, according to numbered section, on reverse side of form. Source: Reprinted with permission of the Metropolitan Chicago Healthcare Council, Guidelines for Dealing with Violence in Health Care, Chicago, IL, 1995. Appendix C Suggested Readings Alspach, G. (1993). "Nurses as Victims of Violence." Critical Care Nurse13(5):13-17. Biles, P.D. (1997). "OSHA's Guidelines for Protecting Health Care Workers from Workplace Violence." Joint Commission on Accreditation of Healthcare Organizations: Environment of Care/PTSM Series 3:29-35. Cal/OSHA. (1998). "Guidelines for Security and Safety of Health Care and Community Service Workers." www.dir.ca.gov/dosh/dosh%5Fpublications/hcworker.html Carroll, V. and Morin, K.H. (1998). "Workplace Violence Affects One-Third of Nurses." nursingworld.org/tan/98sepoct/violence.htm Centers for Disease Control and Prevention, National Institute for Occupational Health. (2002). "Occupational Hazards in Hospitals." DHHS (NIOSH) Pub. No. 2002-101. www.cdc.gov/niosh/2002101.html Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. (1996). "Violence in the Workplace: Risk Factors and Preventive Strategies." Current Intelligence Bulletin 57, DHHS (NIOSH) Pub. No. 96-100. www.cdc.gov/niosh/violcont.html Colling, R.L. (1997). "Controlling Workplace Violence: A Security Management Plan Approach." Joint Commission on Accreditation of Healthcare Organizations: Environment of Care/PTSM Series 3:37-47. Colorado Nurses Association, Task Force on Workplace Violence. (1998). "Survey on Workplace Violence of Nurses in Seven State Nurses Associations." Available from Colorado Nurses Association, Denver, CO. www.nurses-co.org Davis, S. (1991). "Violence in Psychiatric Inpatients: A Review." Hospital and Community Psychiatry 42:585-590. DiBenedetto, D.V. (1992). "Occupational Hazards of the Healthcare Industry: Protecting Healthcare Workers." AAOHN Journal 43(3):131-137. Dillon, S. (1992). "Social Workers: Targets in a Violent Society." New York Times: Al; Al8, November 1, 1992. Distasio, C.A. (2002) "Protecting Yourself From Violence in the Workplace." Nursing 2002 32(6):58-63. www. nursingcenter.com/library/JournalArticle. asp?Article_ID=273445 Elliott, P.P. (1997). "Violence in Health Care: What Nurse Managers Need to Know." Nursing Management 28 (12):38-41. Fazzone, P.A.; Barloon, L.F.; McConnell, S.J.; and Chitty, J.A. (2000). "Personal Safety, Violence and Home Health." Public Health Nursing 17(1):43-52. Flannery, R.B., Jr. (1995). "Violence in the Workplace." New York: Crossroad Press. Flannery, R.B., Jr.; Hanson, M.A.; and Penk, W.E. (1994). "Risk Factors for Psychiatric Inpatient Assaults on Staff." Journal of Mental Health Administration 21:24-31. Gates, D.M.; Fitzwater, E.; and Meyer, U. (1999). "Violence Against Caregivers in Nursing Homes." Journal of Gerontological Nursing 25(4):12-22. Gilmore-Hall, A. (2001). "Violence in the Workplace: Are You Prepared?" American Journal of Nursing 101(7):55-56. Hansen, B. (1996). "Workplace Violence in the Hospital Psychiatric Setting." AAOHN Journal 44(12):575-580. Hunter, E. (1997). "Violence Prevention in the Home Health Setting." Home Healthcare Nurse 15(6):403-409. Joint Commission on Accreditation of Healthcare Organizations. (2002). "Comprehensive Accreditation Manual for Hospitals." Oakbrook, IL: JCAHO. Kinkle, S.L. (1993). "Violence in the Emergency Department: How to Stop it Before it Starts." American Journal of Nursing93(7):22-24. Morgan, L. (1999). "In Harm's Way: Health Care Professionals Face Increasing Abuse in the Workplace." Nurseweek, August 2, 1999. www.nurseweek.com/features/99-8/violence.html Morrison, E., and Herzog, E. (1992). "What Therapeutic and Protective Measures, As Well As Legal Actions, Can Staff Take When They Are Attacked by Patients?" Journal of Psychosocial Nursing 30(7):41-44. Morrison, E.F. (1993). "Toward a Better Understanding of Violence in Psychiatric Settings: Debunking the Myths." Archives of Psychiatric Nursing(7) 6:328-335. Nadwairski, J.A. (1992). "Inner-City Safety for Home Care Providers." Journal of Nursing Administration 22(9):42-47. National Security Institute. (1995). "Guidelines for Workplace Violence Prevention Programs for Health Care Workers in Institutional and Community Settings." nsi.org/library/work/violenc1.html Ore, T. (2002). "Occupational Assault among Community Care Workers." Journal of Healthcare Management 18(1):72-89. Rippon, T.J. (2000). "Aggression and Violence in Health Care Professions." Journal of Advanced Nursing 31(2):452-460. Rusting Publications. (2001). "What Hospital Security Should be Doing Now to Better Prepare for Future Terrorist Activity." Hospital Security and Safety Management 22(6):5-10. Schulte, J.M., et al. (1998). "Violence and Threats of Violence Experienced by Public Health Workers." Journal of the American Medical Association 280(5):439-442. Simonowitz, J.A. (1995). "Violence in Health Care: A Strategic Approach." Nurse Practitioner Forum 6(2):120-129. Simonowitz, J.A.; Rigdon, J.E.; and Mannings, J. (1997). "Workplace Violence: Prevention Efforts by the Occupational Health Nurse." AAOHN Journal 45(6):305-316. Smith-Pittman, M.H. and McKay, Y.D. (1999). "Workplace Violence in Health Care Environments." Nursing Forum 34(3):5-13. www.cinahl.com/cgi-bin/jrlgetarticle?nfor3403 Snyder, W., III. (1994). "Hospital Downsizing and Increased Frequency of Assaults on Staff." Hospital and Community Psychiatry 45:378-379. Sygnatur, E.F. and Toscano, G.A. (2000). "Work-Related Homicides: The Facts." Compensation and Working Conditions 5(1). www.bls.gov/opub/cwc/2000/spring/art1full.pdf University of Iowa, Injury Prevention Research Center. (2001). "Workplace Violence: A Report to the Nation." www.publichealth.uiowa.edu/IPRC/NATION.PDF Worthington, K. and Franklin, P. (2001). "Workplace Violence: What to Do if You're Assaulted." American Journal of Nursing 101(4):73. Worthington, K. (2000). "Violence in the Health Care Workplace." American Journal of Nursing 100(11):69-70. Yassi, A., et al. (1998). "Causes of Staff Abuse in Health Care Facilities: Implications for Prevention." AAOHN Journal 46(10):484-491. Footnote 1 Public Law 91-596, December 29, 1970; and as amended by P.L. 101-552, Section 3101, November 5, 1990. (Back to text) Footnote 2 "Each employer shall furnish to each of his employees employment and a place of employment which are free from recognized hazards that are causing or are likely to cause death or serious physical harm to his employees." (Back to text) Footnote 3 29 U.S.C. 653(b)(4). (Back to text) Footnote 4 CDC/NIOSH. Violence. Occupational Hazards in Hospitals. 2002. (Back to text) Footnote 5 OSHA's Safety and Health Program Management Guidelines (54 Federal Register(16):3904-3916, January 26, 1989). (Back to text) Footnote 6 Section 11 (c)(1) of the OSH Act applies to protected activity involving the hazard of workplace violence as it does for other health and safety matters: "No person shall discharge or in any manner discriminate against any employee because such employee has filed any complaint or instituted or caused to be instituted any proceeding under or related to this Act or has testified or is about to testify in any such proceeding or because of the exercise by such employee on behalf of himself or others of any right afforded by this Act." (Back to text) Footnote 7 29 U.S.C. 158(a)(2). (Back to text) Footnote 8 829 CFR Part 1904, revised 2001. (Back to text) |
||||||||||||||||||||||||
| www.osha.gov | www.dol.gov | |
|
Contact Us | Freedom of Information Act | Customer Survey Privacy and Security Statement | Disclaimers |
||
| Occupational Safety & Health Administration 200 Constitution Avenue, NW Washington, DC 20210 |
||