|
 |
About Us
Division of Adolescent and School Health: School Health Programs, 2008
NOTE: This is a special Web-adapted version of the
Division of Adolescent and School Health's
Program
At-A-Glance. This web page is updated as needed and
reflects the most current data. The
pdf file
[645K] is updated only once per year.
Schools: The Right Place for a Healthy Start
|
| HEALTH
RISKS FACED BY YOUNG PEOPLE |
|
More than 1 in 5 high school students in the United States are
current smokers. Almost 80% of high school students do not eat
the recommended 5 servings of fruits and vegetables
a day.
Only 1 in 3 high school students participate in daily
physical education classes.
More than 1 in 3 children and adolescents are overweight
or at risk of becoming overweight.
Every year, more than 830,000 adolescents become pregnant, and
more than 9 million cases of sexually transmitted diseases occur
among young people aged 15� years.
Nearly 5,000 cases of HIV/AIDS are reported each year among
young people aged 15� years in areas with confidential
reporting.
Young people miss nearly 15 million school days a year
because of asthma. 37% of deaths among adolescents aged 10�
years are due to motor-vehicle crashes. 1 in 5 young people
aged 9� years have symptoms of mental health problems that
cause some level of impairment in a given year. |
|
|
|
Establishing healthy behaviors during childhood is easier and more
effective than trying to change unhealthy behaviors during adulthood.
Schools have a critical role to play in promoting the health and safety
of young people and helping them establish lifelong healthy behavior
patterns because
- Each school day is an opportunity for the nation抯 55 million
students to learn about health and practice the skills that promote
healthy behaviors.
- The nation抯 125,000 schools provide many opportunities for
students to practice healthy behaviors such as eating healthy foods
and participating in physical activity.
Risk Behaviors Established Early in Life
Six priority health risk behaviors contribute to the leading causes of
death, disability, and social problems in the United States. These
behaviors, often established during childhood and early adolescence, are
School health programs need to focus on these priority health risk
behaviors, as well as other key health issues such as
asthma and
mental health, that have a great
impact on the overall health and well-being of students. Health programs
also can make an important contribution by promoting protective
factors梥uch as a positive relationship with a caring adult and
participation in after-school activities梩hat foster positive health and
academic outcomes.
Back to Top
School Health Programs Can Reduce Risk Behaviors and Improve Learning
Research has shown that school health programs can reduce
the prevalence of health risk behaviors among young people and can also
have a positive impact on academic performance.
The following findings demonstrate the effectiveness of school health
programs:
- A tobacco use prevention program conducted in southern California reduced by about 26% the number of
students who started smoking cigarettes
during grades 7�
- Students participating in a culturally appropriate diabetes
prevention program in San Antonio, Texas, showed more favorable changes
in fasting glucose levels, dietary fiber intake, and fitness levels
compared with students who did not participate in the program.
- Inner-city children in Baltimore, Maryland, who participated in a school breakfast program,
increased their nutrient intake and were more likely to improve their
academic and psychosocial functioning than those who did not participate
in the program.
- A comprehensive intervention in public elementary schools that serve
high-crime areas in Seattle, Washington, was significantly associated
with increased student commitment to school, reduced misbehavior in
school, and improved academic achievement. The program involved teacher
training, parent education, and social competency training for students.
Students who participated in the intervention reported fewer risk-taking
behaviors such as violence or heavy drinking.
- Implementation of a multicomponent, school-based physical activity
and nutrition program slowed the increase in rates of obesity and
overweight among low-income Hispanic elementary students in El Paso,
Texas, compared with similar students not exposed to the program. The
program included a classroom curriculum, a family component, and
enhanced physical education and school meal programs.
- Girls enrolled in South Carolina high schools who participated in a
multicomponent, school-based physical activity program increased their
participation in regular vigorous physical activity compared with girls
who did not receive the program. The program included tailored physical
and health education classes, role modeling by faculty and staff,
increased communication about physical activity, promotion of physical
activity by the school nurse, and family- and community-based
activities.
Back to Top
CDC: Advancing and Supporting School Health Programs
Coordinated School Health Programs
A coordinated school health program (CSHP) brings together school
administrators, teachers, other staff, students, families, and community
members to assess health needs; set priorities; and plan, implement, and
evaluate school health program activities. A CSHP typically is led by a
school health coordinator, guided by a school health council or team,
and focused on integrating efforts across eight interrelated components
that already exist to some extent in most schools. These components are
- Health Education.
- Health Services.
- Nutrition Services.
- Health Promotion for School Staff.
- Physical Education.
- Mental Health and Social Services.
- Healthy and Safe School Environments.
- Family/Community Involvement.
A CSHP works to improve the quality of each of these components and
develop and implement activities that cut across multiple components to
meet the needs of students and staff. It features a systematic planning
process that builds on accurate data and sound science, and aims to
eliminate gaps and redundancies.
School health programs are most effective and efficient when all of
the components are addressed together in a coordinated approach
supported by school health councils, collective planning, administrative
support, identified leaders, parents, and community members. CDC has
identified priority actions that states need to take to develop
effective school health programs.
Back to Top
CDC's Leadership Role
CDC is committed to ensuring that all people, especially those at
greater risk for health disparities, will achieve their optimal lifespan
with the best possible quality of health in every stage of life. With
new health protection goals that support healthy people in healthy
places across all life stages, CDC is setting the agenda to enable
people to enjoy a healthy life by delaying death and the onset of
illness and disability by accelerating improvements in public health.
With fiscal year 2008 funding of $13.6 million for CSHP, $41 million
for school-based HIV prevention programs, and $3 million for
school-based asthma management programs, CDC抯 Division of Adolescent
and School Health (DASH) is leading the way in helping schools implement
policies and practices that prevent health risks among children and
adolescents. DASH currently funds education and health agencies in 22
states and 1 tribal government to work together to help schools in their
states implement CSHPs, with a particular focus on promoting physical
activity, healthy eating, and a tobacco-free lifestyle. DASH also funds
50 state education agencies (including the District of Columbia), 1
tribal government, 6 territorial education agencies, and 16 large urban
school districts for school-based HIV prevention, and 10 large urban
school districts for school-based asthma management.
DASH supports the efforts of funded state, territorial, and local
agencies to implement science-based, cost-effective programs by
- Monitoring priority health risk behaviors and school health
policies and programs through the Youth Risk Behavior Surveillance System,
the School Health Policies and Programs
Study, and School Health Profiles.
- Analyzing research findings to develop guidelines for addressing
priority health risk behaviors among students and developing tools,
such as the School Health Index: A Self-Assessment
and Planning Guide, to help schools implement these guidelines.
- Expanding knowledge of how to address youth health risks through
research studies on determinants of health risk behaviors and
evaluations of innovative school-based approaches to health
promotion.
- Supporting the efforts of more than 25 national non-governmental
organizations to build the capacity of states, territories, and
cities to implement effective school health programs. Some of these
groups also are funded to build the capacity of community-based
organizations to implement effective, science-based programs to help
youth in high-risk situations (e.g., those in juvenile justice
facilities or not enrolled in school) avoid critical health risks
such as HIV infection.
CDC Funding for Coordinated School Health Programs, Fiscal Year 2008
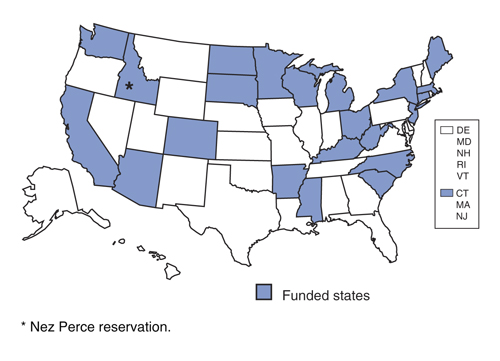
A text description of this map is available.
Back to Top
Making a Difference in the Health of Young People
CDC currently funds 22 states and 1 tribal government for CSHPs; 50 states,
6 U.S. territories, 16 cities, and 1 tribal government for HIV prevention education;
10 cities for
asthma-friendly schools; and 29 national
nongovernmental organizations to support HIV prevention education and CSHPs. (See
state, territorial, and local agencies and tribal governments and national nongovernmental organizations
for more information). The following are examples of some of these
programs.
Success Stories
- Michigan and
Indiana ("MICHIANA")
To ensure that school districts receive the intensive training and
support needed to develop, implement, and sustain CSHPs, the
American Cancer Society, the departments of health and education in
Indiana and Michigan, and other partners worked together to develop
the MICHIANA School Health Leadership Institute. Eight school
districts in Michigan and 10 in Indiana have participated in the
5-year institute. Participants learned how to build organizational
capacity to promote school health programs. Since the institute
began in 2003, participating school districts have raised more than
$11 million in grant funding to support and sustain school health
efforts. In Indiana, all 10 districts passed policies creating
tobacco-free campuses and limiting the sale of unhealthy foods in
cafeterias and vending machines, initiated a school breakfast
program, and mandated physical activity every day for students in
kindergarten through fifth grade. Four districts also created
dedicated staff positions to support the CSHP. In Michigan, all
eight districts passed 100% tobacco-free campus policies and formed
district-wide coordinated school health councils. Five districts
implemented policies to offer healthy vending machine choices, and
three school-based health centers opened.
- North Carolina
Since 2001, the North Carolina Departments of Public Instruction and
Health have jointly sponsored three School Health Leadership
Assemblies to help school superintendents and local health directors
identify ways to improve academic outcomes by improving student
health. These training sessions have reached 43% of the state抯
school superintendents and 59% of local health directors, who
collectively represent 860,000 students. As a result of
participating in these assemblies, superintendents and health
directors have supported the creation of a school health advisory
council in every school district; led more than 40 of their local
education agencies (LEAs) in adopting 100% tobacco-free schools
policies; and encouraged local participation in both the Youth Risk
Behavior Survey and the School Health Profiles. In addition,
participants supported the state抯 School Nurse Funding Initiative,
which has enabled all LEAs in the state to have at least two school
nurses.
- New York City
In an effort to deliver a high-quality and up-to-date HIV/AIDS
prevention education program, the New York City Department of
Education spearheaded a major initiative to update its HIV/AIDS
Curriculum, originally published in the mid-1990s. The revised
curriculum is science-based, skills-driven, standards-based, and
integrated into the overall educational program. During 2006�07,
the department抯 Office of Health and Family Living trained more
than 2,000 teachers, administrators, and parents how to deliver the
revised curriculum to students in more than 1,400 schools. The
curriculum also was adapted for students with special needs, and 77
special education teachers were trained.
- Rhode Island
Rhode Island抯 搕hrive� program梥upported in part by CDC funding and
the state department of health梙as helped school districts establish
health and wellness subcommittees mandated by new state law. The
program provides schools with information and resources, including a
tool kit with guidelines, model policies, and data, to help them
implement the requirements of the federal Child Nutrition and WIC
Reauthorization Act of 2004. Building on the increased awareness of
school health and wellness issues, state legislators also passed
laws in 2006 and 2007 requiring all schools to offer healthier
beverages and snacks.
Back to Top
Future Directions
Because every child needs preparation for a healthy future, CDC
recommends that all states establish coordinated school health programs.
CDC will maintain its commitment to supporting school health programs
and HIV prevention education nationwide and plans to improve the quality
and expand the reach of these programs. As part of this commitment, CDC
will continue to provide key leadership, resources, and experienced
staff to help states, cities, and national organizations create and
maintain the most effective school health programs possible.
"Schools could do more than perhaps any other single
institution in society to help young people, and the adults they will
become, to live healthier, longer, more satisfying, and more productive
lives."
桟arnegie Council on Adolescent Development
Back to Top
Documents on this page are available in
Portable Document Format (PDF). Learn more about viewing and printing
these documents with Acrobat
Reader.
|
|