|
|
| Editorial Team |
Dr. Nestor Nydayimirije
Dr. Josephine Nambooze
Dr. Jimmy Kamugisha
Dr. Eddy Mukooyo
Mr. Peter Kintu
Ms Diana Nakintu
|
WHO (Chairman)
WHO
Min. of Health
Min. of Health
WHO
WHO |
|
Editorial
Completeness of reporting is one of the key factors in Integrated Disease Surveillance and Response. In Uganda, the Ministry of Health in conjunction with WHO has gone a long way in IDSR implementation. The results are as follows: As we gradually go to the end of the year of our bulletin, the reporting from the districts for the first time is almost approaching one hundred percent with weekly epidemiological reports. We still have work to do with our monthly reporting systems. In addition to this, Uganda is possibly the first country in the Africa Region to carry its epidemiological reports in a news paper so as to alert the public. This is not advocacy, but an attempt to carry the whole country along with respect to epidemic preparedness. This indeed is a great achievement as it encourages the districts to send in timely reports. The efforts that have been put into this have been tremendous. Next, we now have to work on reporting on our health indicators. These usually come in with the quarterly reports. However, with the type of progress we are making, this is possible .
Dr. Oladapo Walker - WR Uganda
Back to top
Home-based Management of Fever and IDS
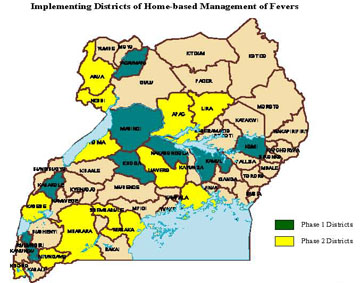
DURING 2002, a strategy for home-based management of fevers will be launched in Uganda, with a goal of contributing to the reduction of morbidity and mortality due to malaria in children under five years.This will involve availing chloroquine and sulphadoxine pyrimethamine at the community and household level. Later, the strategy will be used to introduce interventions on insecticide treated bed nets, intermittent presumptive treatment of pregnant mothers and targeted spraying in epidemic-prone areas.
One of the specific objectives of the strategy is to strengthen data collection on mortality and morbidity in all districts of Uganda. A simple register will be developed for community-based distributors to record the type of treatment given, age, whether treatment was given within or after 24 hours of fever onset. The reports will be analysed and findings linked to the monthly summaries of the HMIS.The following aspects will be achieved:
 |
The community-based health information system (CBHIS) inbuilt into the strategy will entail collecting data on the number of cases which usually stay in the communities and are not normally captured in the health facility records. This will enable health planners to get a better picture about the extent of morbidity in the community of not only malaria but also a projection with other diseases. |
|
The programme will strengthen the collection of vital statistics at the community level, especially on deaths and this will strengthen the current HMIS which is still weak in generating mortality data from the health facilities. Although the causes of death might not be specified, knowing the numbers will be a good starting point in this direction. |
|
Validation and explanation of the reporting problems and provision of reliable assumptions for making morbidity projections will be possible. This will be based on comparisons of surveillance data from implementing and non-implementing districts. |
|
Finally, it is expected that this strategy will generate information which is normally not captured by the current HMIS e.g. factors that affect compliance to treatment, factors that facilitate or prevent prompt care seeking, etc. |
|
| Implementing Districts of Home-based Management of Fevers |
Back to top
Weekly Epidemiological Reporting in Uganda
IN LATE 1998, a system of reporting on epidemicpotential diseases on a weekly basis was established at the Epidemiological Surveillance Division (ESD), Ministry of Health. From this arrangement, it would be possible to track and forecast possible epidemics in the country, and respond timelily when they occur. Districts were supposed to report to the ESD on number of cases and deaths of suspected epidemics on a weekly basis. This reporting system which was aimed at generating .hot data. started with a few district reports, but has now generally improved to cover the entire country. The list of reported diseases was expanded from 5 to 12 notifiable diseases (AFP, cholera, neo-natal tetanus, meningitis, dysentery, measles, malaria, guinea-worm, suspected rabies, plague, typhoid fever and yellow fever).
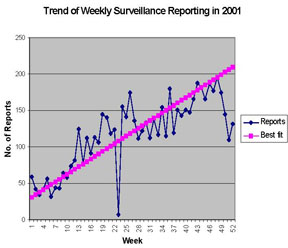
By December 2001, 36 out of the 56 districts (64%) were reporting. During the first quarter of 2002, over 90% of the districts have been submitting weekly reports to the ESD.
During 2001, with WHO support, an EpiInfo database was set up at the ESD to monitor trends on key notifiable diseases. This database is updated on a weekly basis as the reports from the districts are received. It contains the number of cases and deaths reported per week. From the database, it is possible to monitor trends of case-fatality rates for the different diseases. It is also possible to project the likely epidemiological situation of the country in the near future based on the available data and some assumptions (e.g. the completeness of reporting). The database is regularly analysed by the ESD Statistician and as a way of feedback, key results are published in form of a Weekly Epidemiological Newsletter and disseminated to all stakeholders. A recent devel- opment during the first quarter of 2002 has been the publication of a summary of the epidemiological situation in local newspapers on a weekly basis to raise public awareness on epidemic preparedness. This has been a commendable initiative and effort from the ESD.
|
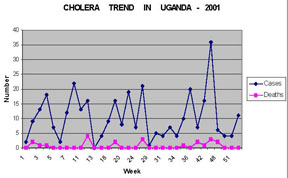
An example of a trend constructed from the ESD
database.
Source: Epidemiological Surveillance Division, MoH. |
|
| Source: Epidemiological Surveillance Division, MoH |
Currently, the main challenge is to ensure completeness of the reports at peripheral level. It has been observed that not all health units in the districts report to the district medical office on time and often some data may not be included in the district weekly report.
Zero reporting is being emphasized and has been successful through the acquisition of a radio-call and an operator who works full time to ensure that all districts submit standardized reports. The challenge remains the sustainability of this service given that the radio-call operator is not on the payroll of the ESD.
Another challenge is the incompleteness of reporting at district level which makes it difficult to utilise the available database for immediate action and forecasting epidemics. This calls for continous efforts and sensitisation to make health workers at district level appreciate the importance of complete reporting. Districts however do not have the required funds for this and are restricted by the budget ceilings provided to them during planning exercises. To sustain these commendable joint efforts in strengthening disease surveillance, the following recommendations can be made:
|
All programmes should utilise the information provided by ESD to respond timely and follow-up the suspected outbreaks. |
|
More support should be given to ESD to maintain and improve these good results. |
Back to top
Suspected Meningococcal Meningitis in Western Uganda
DURING THE FIRST QUARTER of 2002, suspected cases of meningococcal meningitis were observed in Western Uganda, particularly in Masindi and Hoima districts. Most of the cases presented with sudden onset of fever, neck stiffness and later convulsions. Deaths in the community were reported to occur within 2 days. Appropriate investigations and response were instituted by the Ministry of Health in the affected districts.
During a recent joint WHO/MoH investigation in Hoima district, the main findings included:
|
One sub-county had been affected, the first suspected case seen during the week ending 24th February. |
|
By the end of March, a cumulative number of 31 suspected cases had been reported, including 25 at the hospital or health centres and 6 verified from the community by the District Medical Office based on verbal autopsies. |
|
A total of 9 deaths due most likely to meningitis had been registered (3 from the hospital and 6 from the community). Although between 10 and 20 deaths were reported by local leaders and community members, only 6 of these were verified. |
|
13 samples had been tested by the lab in Hoima hospital and 3 showed gram negative diplococcus, but sero-typing was not done. |
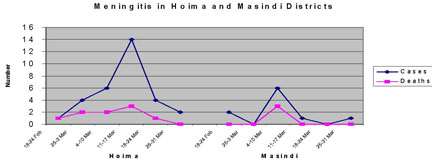
The peak in Hoima district was reached during the week of 11th. 17th March and in Masindi a week earlier. The most affected sub-county in Hoima (Kyabigambire) borders with Masindi district. 52% and 48% of the cases were male and female respectively. The majority of the suspected cases (55%) were aged between 6-18 years, the school-going age; no case below 5 years was seen. Analysis on treatment outcome indicated that 76% had either improved or still on treatment, 12% had escaped and 12% had died by the end of March.
|
Source: Epidemiological Surveillance Division -
MoH and District Medical Office - Hoima. |
In the hospital and health centres, case definitions and treatment guidelines were available, except that the lower cadres (nurses, nursing aides) may not have internalised them. The drug supplies to handle meningitis were available in Hoima hospital where a special ward had been set up and all suspected meningitis cases from the health centres/community were referred to the hospital. Considering Hoima records and according to WHO guidelines, threshold levels for a meningitis epidemic were reached, however, most of the cases were based on verbal autopsies and clinical findings. Although gram negative diplococcus were observed in 3 samples at the Hoima hospital lab, full laboratory confirmation for neisseria meningitidis was not done on time. However, during the last week of March, neisseria meningitidis sero-type A was isolated by the Central Public Health Laboratory in one of the samples received from Hoima District.
A mass vaccination campaign was immediately started by the District Health Team in schools where suspected cases were reported. Although some vaccination exercise had been carried out in Masindi, it was not done properly according to scientific evidence.
In situations of suspected meningitis outbreaks, active surveillance is strongly recommended to identify and report any new cases. Before initiating treatment, cerebrospinal fluid samples should be taken immediately for laboratory confirmation. Furthermore, it is necessary to strengthen community health workers to improve on reporting from the communities, especially line listings of the suspected cases. It is also important to do sero-type confirmation before conducting mass immunisation exercises. The importance of involving all political and civic leaders in particularly surveillance, social mobilisation and public information is emphasized.
Back to top Laboratory investigation of outbreaks in Uganda
LABORATORY CONFIRMATION of epidemics is one of the main components of Integrated Disease Surveillance and Response (IDSR). MOH/WHO in Uganda are strengthening capacity to provide timely confirmation through developing regional laboratories, and setting up mechanisms for specimen referral to laboratories with competence to confirm priority pathogens. During the period Jan-Dec 2001, outbreaks were investigated as shown in the table.
Notably all the 4 outbreaks of meningitis were investigated. However, 2 were false outbreaks and the remaining 2 could not be confirmed as CSF specimens could not be obtained from patients already started on therapy. Gram stained slides had been discarded by the laboratories in health units. Major challenges with meningitis are the fastidious nature of meningococci whose survival before reaching the laboratory is difficult to assure; additionally the seriousness of the disease often leads to administration of treatment before laboratory investigations. Regarding plague, lack of secure laboratory facilites dedicated to plague have led to presumptive confirmation using Wayson
stain.
In future, mechanisms for timely shipment of cerebrospinal fluid and plague specimens to laboratories with ability to perform cultures will be addressed. Source: Central Public Health Laboratory, ESD and Uganda Virus Research Institute.
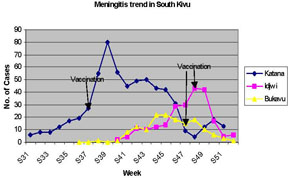
Back to top Meningitis Epidemic in South Kivu - DRC
MENINGITIS OUTBREAK in the province of South Kivu in the Democratic Republic of Congo (DRC) was first reported in Katana health zone on 11th September 2001 (week 31). After confirmation of the epidemic with the support of Cemubac project, the province declared the epidemic in week 34. While the epidemic was almost reaching the peak in Katana (weeks 38 and 39), first cases were reported in Idjwi and Bukavu health zones, both located on the border with Rwanda on the shores of Lake Kivu. The spread of the epidemic in these locations was threatening both the neighbouring Rwanda and Burundi.
In Katana, after the peak in week 39, the epidemic significantly decreased until week 48 and then another small peak was observed during week 50.
In Bukavu health zone, the first case was reported in week 38.The peak of the epidemic in Bukavu (4 cases per 100,000) was observed in weeks 44 and 45. Although the epidemic threshold was not reached, there was a high potential risk of a very huge epidemic if the vaccination was not done on time. The attack rate which is lower than the epidemic threshold is probably due to inadequate denominators used. The epidemic was controlled by the end of the year (weeks 51 and 52).
In Idjwi, the epidemic was reported in week 40 and the peak was observed in week 48. It then decreased significantly up to week 51
The case-fatality rate was higher than WHO/AFRO acceptable level in Katana (12.4%) and respectively 8.8% and 7.1% in Bukavu and Idjwi. The high CFR in Katana was observed in the first days due to late admission of patients. The provincial epidemic management committee was put in place and initiated some measures like social mobilisation, mass vaccination campaign targeting the schools and camps of regrouped people. Active surveillance and reporting was established daily and weekly for monitoring epidemic trend and the vaccination campaign.
Technical support was provided by WHO and NGOs (e.g. MSF-Holland, IRC), and vaccines were mobilised from WHO and neighbouring countries (Rwanda and Burundi). It was recommended to South Kivu Province to disseminate and use the new alert and action thresholds for meningococcal meningitis.
Lastly, countries in the sub-region should be on high alert during 2002 due to the high risk of possible outbreaks of meningococcal meningitis.
|
| Source: MoH, South Kivu Province - DRC. |
Back to top
|