|
|
| Editorial Team |
Dr. Nestor Nydayimirije
Dr. Miriam Nanyunja
Dr. Eddy Mukooyo
Mr. Peter Kintu
|
WHO (Chairman)
WHO
Min. of Health
WHO
|
|
Editorial
This issue if the IDSR/Health Information Bulletin marks 2 years of continuous publication and dissemination. At the beginning if the third year, we continue to advocate for adequate feedback and information sharing with all partners in the area of integrated disease surveillance and response.
Despite the level of preparedness, emerging and re-emerging diseases continue to pose a big threat to the surveillance system. However, with strong intercountry cooperation, as exhibited in the great Lakes Ministerial Meeting, preparedness and response to these threats will be ensured.
Strengthened laboratory services and timely reporting are positive steps towards in the building of a strong surveillance system, and this should be sustained.
Dr. Oladapo Walker - WR Uganda
Back to top
Great Lakes Ministerial Meeting:
inter-country cooperation moves ahead
THE MINISTERS OF HEALTH of the Great Lakes Countries endorsed a Protocol of Cooperation in August 1997in Kigali, Rwanda. The signatories to this protocol included Burundi, Democratic Republic of Congo,Rwanda, United Republic of Tanzania and Uganda. The protocol provided a framework for strengthening epidemiological surveillance and laboratory services, effective control of epidemics and selected public health interventions, synchronization of cross border mass vaccination campaigns and regular and timely exchange of disease information.
A ministerial meeting on epidemic prevention and control in the Great lakes countries, preceded by a 3-daymeeting of experts, was held in Kampala from 26 to 27June 2003. Based on an independent consultant’s report on the review of the implementation of the Kigali protocol, the 5 day meeting (23–27 June 2003) was organized to review and amend the protocol of cooperation, and develop a future plan of action based on this review.
The main objective of the meeting was to strengthen epidemiological surveillance and control of epidemics in the Great Lakes Countries.The participants to the meeting were the Ministers of Health, senior officials from Ministries of Health in charge of epidemiology and surveillance, and partners (UNICEF, USAID, Italian Cooperation, JICA). Kenya attended as an observer.
The success of this cooperation protocol has pulled Kenya to join the GL countries in signing the revised protocol. WHO was represented by the Director of Programme Management, WHO Country Representatives and the technical units at country, regional and global levels.
Given the key outputs from this meeting, which included the amended protocol of cooperation, a four year plan of cooperation (2004-2007) and inclusion of Kenya in the GL bloc, there is a good indication that inter-country cooperation is moving ahead in GL region.
|
| A group photo of Ministers, DPM, WRs and participants. |
Back to top HMIS Reporting Levels in Uganda
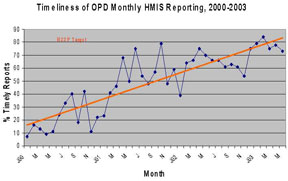
TIMELINESS AND COMPLETENESS of Health Management Information System (HMIS) reporting have been considered key process indicators for the implementation of the Health Sector Strategic Plan (2000/1 – 2004/5), with the 5-year target set at 80%. At the Ministry of Health (MoH) level, timeliness in reporting is defined as receipt of the monthly report by the 28th day of the following
month. Although completeness is usually taken to be the proportion of district reports received at the centre,the proportion of health facilities reporting out of the total number of units in the districts gives a better picture.
During the past 3 years, HMIS has been strengthened through the monthly reporting of out-patient data from the districts to the central level. There has been a general improvement in reporting from a national average of21% in 2000, 53% in 2001, 63% in 2002 and 79% in the first quarter of 2003. The graph below shows the trend in timeliness of monthly HMIS reporting from the districts to the MoH.
|
| Source: Resource Centre, MoH |
In 2000, the number of districts submitting monthly reports in time was very small (<50%). However, with improved feedback from MoH to the districts and availability of revised HMIS tools, reporting improved significantly during most of 2001. The revision of the tools led to more integration and fewer reporting forms, thereby saving on time of the health workers who used to fill and report several forms to several departments in the MoH. The feedback package included a summary showing the performance of all districts in terms of reporting and some key disease trends. This feedback would not only be sent to the district health team, but would also be copied to the district political leaders (Chief Administrative Officer, District Chairperson and Secretary for Health) and would sometimes be discussed in the district councils.
During 2002, there was some decline in the level of timely reporting. This was mainly caused by the limited availability of HMIS reporting tools in most of the districts.
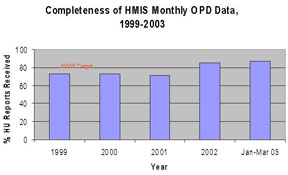
Similarly, there has been general improvement in completeness of the data reported to the Ministry of Health from 72% in 1999 to 85% in 2002 and this improvements continuing to be registered in 2003 (see graph below).
|
| Source: Resource Centre, MoH |
HMIS tools have usually been supplied by the Ministry of Health for maintenance of uniformity and standardization. Despite of increased knowledge and motivation of health workers on the use of HMIS, non-availability of funds for printing HMIS tools contributed to the decline in reporting. Also, the established reporting process from the districts used to be bogged down by the many reception points in the Ministry of Health which could sometimes lead to late processing or even loss of some forms. Towards the end of 2002, funds were secured to print and disseminate enough HMIS materials. Production and dissemination of these tools to all districts is currently on-going. The main health databank at MoH has also been equipped with improved communication means (fax, telephone and e-mail) so that all reports from the districts are received and processed at one point.
With support from WHO and other partners, training and support supervision, focusing on HMIS data management and analysis has been conducted in a number of districts between 2001 and 2003. This training targets HMIS/surveillance focal persons, in-charges of health facilities and records assistants who normally collect and process health data in the districts, sub-districts and health facilities.
The rapid implementation of the Integrated Disease Surveillance and Response (IDSR) strategy in Uganda is also responsible for the registered improvements in HMIS reporting. The strategy has strengthened ownership of the HMIS since all programmes plan supervision, monitoring and training together, resulting in an improved integrated reporting system. The results of these interventions can be evidenced by the improved levels of reporting during the first quarter of 2003. Although there are some bottlenecks, the HMIS is established and functioning in Uganda. In-patient data collection and reporting remains a big problem. However, with more support from development partners, especially in terms of human resource development at all levels, a good quality HMIS will be achieved.
Back to top New Epidemic Threats in the Great Lakes Region
COMMUNICABLE DISEASES comprise more than 75% of the disease burden in the Great Lakes sub-region. Outbreaks and epidemics of the “known” diseases (cholera, meningococcal meningitis, measles and dysentery) have been experienced in the past 5 years. Integrated disease surveillance and response implementation has been initiated in all countries in the sub-region and is quite advanced in some countries. However, there is often inadequate capacity for disease confirmation, response and surveillance due to limited laboratory capacity, logistics, human resources, etc. In addition, new and re-emerging epidemic threats have been experienced in the Great Lakes sub-region. These include emerging infections like the Severe Acute Respiratory Syndrome (SARS) and re-emerging infections, for instance Yellow Fever, Ebola and Marburg Fever. These burden further the weak alert and response systems in the countries.
Yellow Fever:
Regarding the re-emerging infections, a yellow fever outbreak in Southern Sudan was notified in April 2003. The affected areas border Uganda and Kenya. Due to proximity to the affected area, presence of appropriate vectors (as shown by entomological studies), limited access due to insecurity and continued cross border movements from and to the epifocus, Ugandan and Kenyan northern border districts are at high risk to the yellow fever outbreak. A vaccination campaign has been on-going in Southern Sudan since June 2003. Vaccination
campaigns are being planned by Kenya and Uganda in a limited number of border sub-counties/districts.
Some of the problems that have hindered appropriate preparedness and response to the yellow fever threat include inaccessibility insecurity in the affected areas and logistical constraints.
SARS:
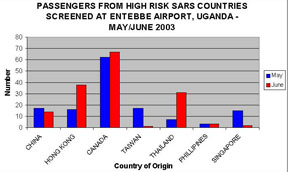
Concerning new threats, severe acute respiratory syndrome (SARS), a new disease caused by a new emerging virus of the coronavirus family started in China in November 2002. SARS spread to more than 10 countries within a few months. Identification of the causative agent and diagnostic methods (ELISA, PCR) was done quite quickly and work on vaccine development is ongoing. Prevention of spread has not been easy due to inter-country movements of patients, yet screening has not been done in all countries. Uganda started a screening exercise at the international airport and another busy border point with Kenya during May and June 2003 in an attempt to control the spread of this new epidemic. The graph below shows the number of passengers from high risk countries screened at Uganda’s international airport.
In the Africa Region, two probable cases were reported in South Africa(1) and Nigeria(1). Uganda had a “suspected case” but results were confirmed negative. SARS is a real threat for all countries in the great lakes region. There is need to develop national capacity for response to SARS. There are, however, a number ponder:
 |
Have screening mechanisms been established at different entry points of the different countries? |
|
In case of a suspected case, are the countries in position to handle (appropriate isolation facilities and logistics, contact tracing, case management, health worker protection, and blood screening and safety) |
|
| Source: National SARS Task Force, MoH/Uganda |
As we struggle to strengthen the national systems for control and response to epidemics and outbreaks for the “traditional” epidemic-prone diseases, we are faced with even more challenging global threats of emerging and re-emerging infections. The main challenge is to strengthen our systems further to ensure appropriate response to these threats. The following proposals are advanced.
|
Uniform/similar screening guidelines in the GL countries emerging and re-emerging infections. |
|
Standard response guidelines/checklists should be developed and used by the countries. |
|
Mobilisation of required resources (financial, logistical, human, etc.) jointly as a bloc, for strengthening of the national surveillance systems to enable them cope with these new threats, in addition to the traditional diseases. |
|
More investment in improving laboratory services in every country, and establishment of a specialised laboratory in the region. |
|
Development of an inter-country communication strategy |
|
Strengthening community component of IDSR through establishing community alert systems to enable early detection. |
Back to top
Progress in National Public Health Laboratory Services
DURING THE SECOND QUARTER OF 2003, public health laboratories played a significant role in rapidly investigating epidemics in the region, leading to appropriate public health actions. For example, a yellow fever outbreak at the border between Kenya and Sudan was rapidly confirmed; a suspected yellow fever outbreak in a district north of Kampala, Uganda was quickly investigated and found negative.
During the same period, reporting has improved. D. R. Congo, Tanzania and Uganda have improved in data management, through use of EpiInfo 2000 or Excel software. The table below shows summarized data received at the sub-regional inter-country team office during the reporting period.
Summary of National Public Health Laboratory Reports for Great Lakes and Horn of Africa Epidemiological Blocs during the 2nd quarter of 2003
ECHANTILLONS
/AGENTS PATHOGENS* |
PAYS/COUNTRY** |
| BurundiI |
D.R.C |
Ethiopia |
Rwanda
(Only April report) |
Tanzania |
Uganda |
LCR
/CSF |
Nombre d’e chantillons analyses/Number processed |
8 |
1 |
2 |
0 |
1 |
11 |
| N. meningitidis --A |
0 |
0 |
0 |
0 |
0 |
6 |
| N. meningitidis --C |
0 |
0 |
0 |
0 |
0 |
0 |
| N. meningitidis --W135 |
0 |
0 |
0 |
0 |
0 |
0 |
| Autres/Other agents pathogenes, specifier |
0 |
0 |
2 Str . Pneum-oniae |
0 |
0 |
1 Str. Pneum-oniae |
Selles
/Stools |
Nombre d’e chantillons analyses/Number processed |
357 |
19 |
127 |
15 |
10 |
107 |
| V. cholerae, 01, El Tor, Ogawa |
0 |
0 |
0 |
0 |
0 |
14 |
| V. cholerae, 01, El Tor, Inaba |
0 |
0 |
0 |
0 |
10 |
0 |
| Shigella dysenteriae type 1 |
0 |
0 |
2 |
0 |
0 |
3 |
| Autres/Other shigellae |
0 |
5 |
0 |
0 |
0 |
5 |
| Salmonella typhi |
4 |
0 |
0 |
0 |
0 |
0 |
| Autres/Other Salmonellae |
0 |
9 |
0 |
2 |
0 |
1 |
| Polio Virus |
0 |
0 |
8 |
0 |
0 |
0 |
| Entero virus |
0 |
0 |
1 |
4 |
0 |
0 |
Sang
/Blood |
Nombre d’e chantillons analyses / No. processed |
891 (incl. mal bs) |
0 |
20 |
54 |
0 |
0 |
| Bacteries, specifier /specify |
0 |
0 |
0 |
0 |
0 |
0 |
Virus, specifier /specify |
0 |
0 |
0 |
0 |
0 |
0 |
|
*No other specimens were collected. **Kenya and Eritrea did not report during this period.
Source: National Public Health Laboratories.
Notably yellow fever data are not presented, the reason being virology services are not yet integrated in National Public Health Laboratory Systems. Integration is an area that merits immediate attention for rational and efficient use of the few available resources.
Another dimension is that accuracy of reporting enables a quick view of coverage by public health laboratories. The map below shows the districts/provinces of origin of specimens reported by National Public Health Laboratories. Boundary maps for Eritrea and Ethiopia were not available, hence are not included.
|
| Districts/provinces of origin of specimens reported by N PH L District/province of origin |
Back to top
|