| |
| Editorial Team |
Dr. Josephine Nambooze
Dr. Nestor Nydayimirije
Dr. Jimmy Kamugishsa
Dr. Eddy Mukooyo
Mr. Peter Kintu
Ms. DianaNakintu |
WHO
WHO
Min. of Health
Min. of Health
WHO
WHO |
|
Editorial
Analysis and utilisation of health information at all levelscontinues to be a key aspect on WHO‘s agenda.During theyear 2001, WHO country office strongly supported Ministryof Health in strengthening health management informationsystems and the key results include rapid improvements inreporting from the districts and generation of adequateinformation for detection of epidemics. We remain committed to supporting feedback mechanisms aimed atutilisation of information for action and continue to advocate for improved information technology in the districts. It is hoped that this third issue of the IDS/HIS bulletin willstimulate discussions for designing interventions in thehighlighted problem areas. Through this medium, WHOcontinues to urge development partners for more supportto the health ministry in order to fulfil its mandate of reducingmorbidity and mortality levels. We dedicate this issue to the late Dr. Kassi Manlan.
Dr. Oladapo Walker - WR Uganda
Back to top Malaria Morbidity and the RBM process
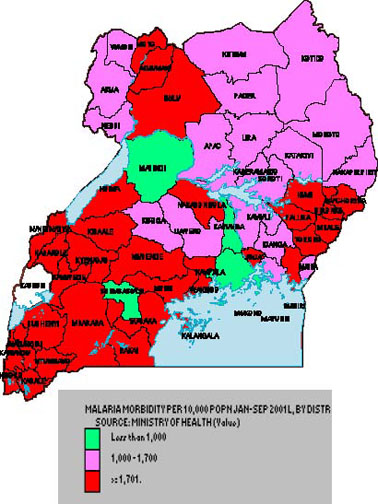
MALARIA continues to be a major disease burden in Uganda. Updated returns from the first three quarters of the year 2001 showed more than 50% of the districts with an iNCIDence of more than 1,700 per 10,000 population, with high concentration in western and southwestern districts of the country. However, the burden is still huge and calls for a bigger effort to avert malaria epidemics in the region. Malaria epidemic was predicted in 13 districts. The predicted epidemic was well contained and controlled.
A review and planning workshop for roll-back malaria (RBM) in the East Africa and Great Lakes Epidemiological Bloc was held in November 2001 in Kampala, Uganda. The main aim was to bring together malaria focal persons in the sub-region, build partnerships between country programmes and enhance communication. Some key recommendations for WHO were as follows:
 |
speeding up the process of drug policy change in the subregion,
through supporting countries to mobilise political
commitment and adapt the regional framework to guide
the process of change at country level. |
|
supporting countries to strengthen national capacity to
develop forecasting and early detection systems, by
utilising HMIS |
|
liaising with the WHO pesticide evaluation unit to provide
advice to countries on mosquito susceptibility tests and
the appropriate insecticides for mosquito nets in the subregion. |
 |
| Through strengthening partnerships in the RBM process and effective malaria data utilisation, early detection and response to malaria epidemics in the region will be enhanced. |
Back to top
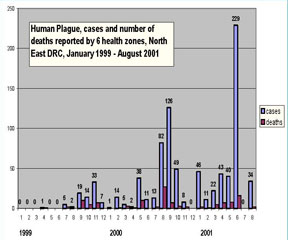
Plague epidemic in GL sub-region
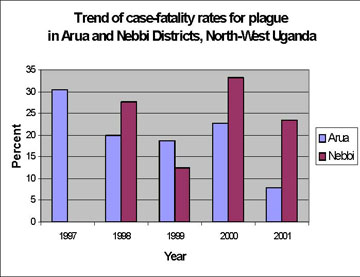
PLAGUE is an endemic problem in the border districts of D.R. Congo and Uganda. In 2001, the case fatality rates for plague were 7.8% and 23.4% in Arua and Nebbi districts respectively in North-Western Uganda, and 9.6% in the 5 health zones of the Eastern Province of the DR Congo. The main reference laboratory for plague confirmation in the region is the UVRI, Entebbe. Transportation of these samples, especially from Eastern DRC has always been a problem. This stretches the surveillance system. Confirmatory testsdone on a sample of cases from Nebbi district in Uganda in October 2001 demonstrates that the most prevalent type of plague was bubonic (46.2%), followed by septicaemic (30.8%) and pneumonic (23.1%). Postmortems confirmed Yersinia pestis bacilli on Wayson stain.
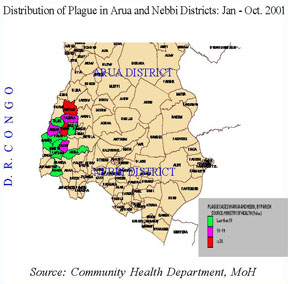 |
| Source: Community Health Department, MoH |
Some of the control measures currently employed include:
|
Community mobilisation through health workers and via local FM radios, alerting communities on the signs and symptoms of the disease, and the need for early reporting and treatment of cases. Advice against visiting affected areas and cautioning public gatherings especially funerals. |
|
Case treatment and prophylaxis. Drugs (tetracycline) are supplied to contacts in the villages, however this sometimes covers only those found at the burial
sites. It is usually not clear how many people in these villages could have already got into contact with the infection and who may become new cases. There is need to target all the affected villages. |
|
Flea control. House spraying with Fendona was done in some parishes where cases of bubonic plague were identified. |
|
Case Reporting: The data on suspected plague cases reported from January 1999 to August 2001 in 6 health zones in Ituri district, Eastern D.R. Congo, indicate that increased iNCIDence of the disease in Rethy (288 cases), Logo (97) and Rimba (40) health zones. In 1999 and 2000, peak iNCIDence occurred between August and November although a few cases were reported in February and May. Half of the cases (i.e. 109 of the first 240 reported in the 6 health zones in 2001) are younger than 5 years old. |
 |
| Source: Community Health Department, MoH |
Over the past years, rodents and reservoirs in the 2 natural plague foci in DRC (i.e. health zones in Ituri and Lubero districts) have been studied extensively. Ecological factors cited by local health personnel in disease causation, including high altitude, high population density and rainy seasons which force rodents in the disease reservoirs to run to drier areas in domestic settings.
 |
| Source: OMS Province Orientale, CSLP Bunia |
Back to top OPD Utilisation in Uganda
OPD UTILISATION, a key output indicator for monitoring utilisation of health services, was low in Uganda over the past 5 years. The average OPD utilisation per capita for both government and NGO health services in Uganda was about 40%. The target set in the health sector strategic
plan 2001-2005 (HSSP) is 60%. During 2001, the first year of HSSP implementation, the national average OPD utilisation per person stood at about 50%, 28 (50% of the districts have achieved the HSSP target of 60%. This will further be improved by increased support to districts, especially in the area of drug supply and management, health personnel recruitment and retention, efficiency in the flow of funds earmarked for health services and improved operationality of health sub-districts. These factors directly affect the organisation of health services and hence, the utilisation of these services in the country.
 |
| Source: Resource Centre, MoH |
Back to top Sanitation in Uganda
GOOD SANITATION is key in the prevention and control of epidemic diseases and is a major determinant of health outcomes. The Environmental Health Programme of the Ministry of Health has set out to:
|
strengthen collaborative mechanisms at various levels and with relevant agencies for
promotion of safe water and sanitation and occupation health; |
|
promote gender responsive IEC to support community mobilisation on environmental health matters; |
|
promote clean and hygienic living conditions at household level; and |
|
integrate sanitation and hygiene in school health and educational programmes. |
One key indicator for good sanitation is latrine coverage; i.e. the percentage of households with a proper latrine. Latest data from the Ministry of Health (2000) indicate that national latrine coverage stands at about 49% (range Bushenyi 80% and Kotido 6%). The majority of districts with a coverage of below 30% were noted to be in the northern region, especially in areas with civil strife As a key HSSP target, the division aims at increasing safe waste disposal including human excreta in 60% of the households and institutions in Uganda by the end of 2004.
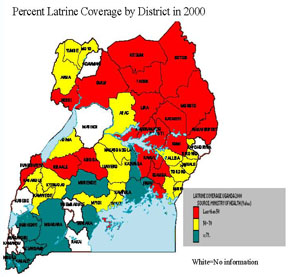 |
| Source: Environmental Health Division, MoH. |
Back to top Tetanus Toxoid Immunisation in Uganda
The main objective of the Uganda National Expanded Programme on Immunisation (UNEPI) is to ensure attainment of the highest levels of coverage such that the EPI target diseases are no longer of public health significance in the country. The programme aims at increasing TT2-5 immunisation coverage of pregnant women to 80% by the end of 2005, as part of maternal and neonatal Tetanus (MNT)elimination. Available data, however, shows low coverage and high drop-out rates for TT2-5 among pregnant women in Uganda. These rates are rather worse among nonpregnant women. During 2001, the national coverage rate for TT2-5 among pregnant women stands at only 28%. However, interpretation of these figures has been difficult as the current surveillance looks at all women in the reproductive age-group without considering their previous Tetanus immunization status (including those who have completed their 5 doses). This therefore calls for a concerted effort between the different programmes especially EPI, Reproductive Health and HMIS to develop a tool for monitoring Tetanus2 and 3 coverage in the entire population.
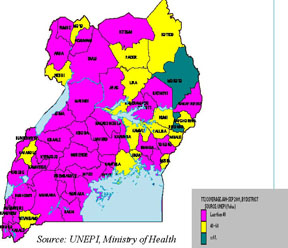 |
| Source: UNEPI, Ministry of Health |
Back to top
Regional Efforts to Control Epidemics In August 1997, health ministers from the GREAT LAKES SUB-REGION agreed to cooperate in epidemic surveillance and response so that their individual efforts could be sustainable by collective action. With this political commitment, the first intercountry
meeting on epidemic-potential disease control was held in October 2000 in Butare, Rwanda. Recently, a similar intercountry meeting was held in October 2001 in Bujumbura, Burundi. This meeting brought together 5 countries in the sub-region (Burundi, Rwanda, Uganda, Tanzania and DR Congo) to review the progress made in implementing the Operational Plan of Collaboration formulated in Rwanda in October 2000. A new Operational Plan of Cooperation for the period 2001-2002 was agreed upon by the member states, with the following key aspects:
|
strengthening surveillance through information exchange,
dissemination of standardized tools, community participation,
and clarifying dialogue for control of zoonosis, |
|
strengthening Laboratory Networking through capacity
building, provision of standard technical guidelines,
restocking reference laboratories, and setting up lab
networks at country level, |
|
enhancing epidemic management through organisation of
cross-border meetings. The next inter-country meeting
is scheduled for October 2002 in D.R. Congo. |
|
| At the opening of the Inter-country meeting in Bujumbura, Burundi, October 2001 (second left is the late Dr. Kassi Manlan, then WR Burundi) |
Back to top |