|
|
|
|
|
Malaria Situation in the Amazon Region in the 1990sBy the early 1990s, countries in the Amazon region of South America began to experience a reemergence of malaria. While Plasmodium vivax continued to be the most prevalent species, P. falciparum was increasing at alarming rates. A number of factors were thought to be associated with this increase including the migration of large numbers of nonimmune persons into malaria-endemic areas, establishment of such highly competent malaria-transmitting mosquitoes as Anopheles darlingi, climatic fluctuations, such as seen with El Niño, and low levels of funding for malaria control programs. Of further concern was the presence of strains of P. falciparum resistant to chloroquine and sulfadoxine-pyrimethamine.
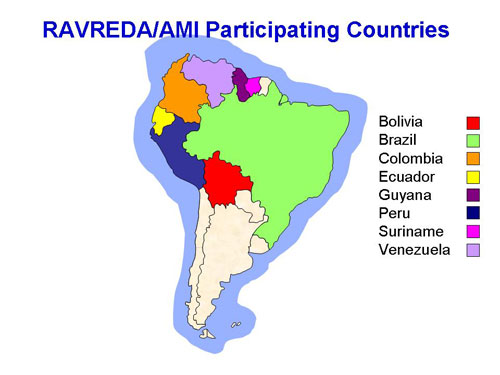
History of RAVREDA/Amazon Malaria Initiative (AMI)In 1998, representatives from CDC attended an expert meeting held in Manaus, Brazil, to adapt the World Health Organization’s standardized in vivo malaria drug efficacy protocol for the Americas. At the meeting, researchers interested in antimalarial drug resistance in the Americas formed an information network. Later that year, researchers from the Instituto Nacional de Salud in Peru, in collaboration with malariologists from CDC, embarked on a series of drug studies to assess different drug combinations containing artemisinin derivatives for uncomplicated P. falciparum malaria. In 2001, the Pan American Health Organization (PAHO) convened a meeting in Salvador, Brazil, on drug resistance in the Amazon region. Participating countries included Bolivia, Brazil, Colombia, Ecuador, Guyana, Peru, Suriname, and Venezuela. Countries in attendance agreed to use the adapted, standardized in vivo protocol within a newly created regional network to monitor antimalarial drug resistance. The network was named Red Amazónica para la Vigilancia de la Resistencia a las Drogas Antimaláricas (RAVREDA) (Amazon Network for the Surveillance of Antimalarial Drug Resistance). Funding for RAVREDA was made available by the United States Agency for International Development (USAID) under the name Amazon Malaria Initiative (AMI).
RAVREDA/AMIRAVREDA/AMI has four main objectives:
Its members are Bolivia, Brazil, Colombia, Ecuador, Guyana, Peru, Suriname, and Venezuela. Three partners provide technical assistance: CDC www.cdc.gov/malaria, Rational Pharmaceutical Management Plus/Management Sciences for Health www.msh.org/projects/rpmplus/index.html, and the United States Pharmacopoeia www.usp.org. USAID www.usaid.gov and PAHO www.paho.org serve as coordinating agencies. RAVREDA/AMI Accomplishments
CDC ContributionsIn the first few years after RAVREDA/AMI was established, CDC provided technical assistance in the areas of antimalarial drug efficacy and effectiveness, and mosquito control. Highlights include:
After initial in vivo efficacy studies were completed and most member countries had changed their antimalarial drug policies, the countries began to evaluate other components of their national malaria control programs.
CDC, along with other technical RAVREDA/AMI partners, was asked to share its expertise on various topics: evaluation of patient adherence to antimalarial regimens; development of strategies to reduce transmission through vector control, including evaluation of insecticide-treated mosquito net efficacy and insecticide resistance; evaluation of the burden of malaria in pregnancy; and evaluation of the quality of care provided at health facilities. In addition, CDC continued to support building laboratory capacity in bioavailability assays and, through studies in the field and training several health personnel, in molecular epidemiology. CDC encourages and supports direct collaboration among partner countries, as well as sustainability of malaria control activities. CDC envisions continued collaboration with RAVREDA/AMI partners to strengthen malaria control activities and reduce the burden of malaria in the region.
Page last modified : December 22, 2006 Content source: Division of Parasitic Diseases National Center for Zoonotic, Vector-Borne, and Enteric Diseases (ZVED)
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


| Home | Policies and Regulations | Disclaimer | e-Government | FOIA | Contact Us | ||||||
|