Annual Report on Prevention of Mother-To-Child Transmission of the HIV Infection (June 2004) PDF version PDF version Reaching Mothers
The President's Emergency Plan for AIDS Relief Annual Report on Prevention of Mother-To-Child Transmission of the HIV Infection
Submitted by the Office of the U.S. Global AIDS Coordinator, U.S. Department of State, June 2004 TABLE OF CONTENTS
Silver Lining: A Success Story from Guyana Examples of Program Activities in Key Areas
One Child at a Time: A Success Story from Mozambique Facing Programmatic Challenges: Looking to the Future
Country Results for U.S. Government-Supported Activities The Power of the Individual “Femme Active”: A Success Story from Côte d’Ivoire
“One of our best opportunities for progress against AIDS lies in preventing mothers from passing on the HIV virus to their children. Worldwide, close to 2,000 babies are infected with HIV every day, during pregnancy, birth or through breast-feeding. Most of those infected will die before their 5th birthday. The ones who are not infected will grow up as orphans when their parents die of AIDS. New advances in medical treatment give us the ability to save many of these young lives. And we must, and we will.” President George W. Bush
Since the launch of President George W. Bush’s International Mother and Child HIV Prevention Initiative in 2002, the United States Government has focused significant resources on reaching HIV-positive, pregnant women with short-term anti-retroviral (ARV) prophylaxis to prevent the transmission of HIV to their babies during delivery and in early infancy. The Initiative targeted fourteen countries in Africa and the Caribbean1, and the Caribbean region, committing $500 million over five years. The President’s Initiative is focused on two areas:
The President’s Emergency Plan will build on the significant work already accomplished under the International Mother and Child HIV Prevention Initiative, now integrated into the Emergency Plan, by:
During the initial phase of PMTCT programming, ARV treatment was not widely available. As such, the emphasis was on saving those babies at risk for infection during childbirth and early infancy through short-course ARV prophylaxis. Now, through the work of the Emergency Plan, programs are being scaled up to provide long-term ARV therapy to communities at large. Long-term treatment of pregnant women with ARV is a key advance in preventing the transmission of HIV from mothers to their newborns. The treatment of pregnant women with combination ARV therapy during and after pregnancy has been shown to reduce the transmission of HIV from mothers to children by more than 90 percent compared to a 50 percent reduction with short-course preventive prophylaxis, particularly in the absence of prolonged breastfeeding. In addition, there is hope that the treatment can reduce transmission during breastfeeding. Beyond preventing the transmission of HIV to newborns, the Emergency Plan goal of treating two million adults and children with ARV therapy over five years offers hope to mothers and fathers that they can remain healthy to preserve their families and protect their children from the terrible prospect of becoming orphans. And in the unfortunate instance when a baby is born infected, the availability of ARV treatment provides the opportunity for the child to remain healthy for as long as possible. The United States Leadership Against HIV/AIDS, Tuberculosis, and Malaria Act of 2003 requires an annual report that addresses the activities of relevant executive branch agencies regarding PMTCT. (Title III, Subtitle B, Sec. 313). From October 1, 2002, the start of the first fiscal year for the President’s International Mother and Child HIV Prevention Initiative, through March 31st 2004, U.S. Government agencies, particularly the U.S. Agency for International Development (USAID) and the U.S. Department of Health and Human Services (HHS), under the leadership of the U.S. Global AIDS Coordinator, report significant progress on establishing PMTCT services in the 14 focus countries and in providing technical assistance, training, and laboratory support to the Caribbean region. _______________ Highlights The U.S. Government has supported the implementation of national PMTCT guidelines in each of the focus countries to ensure that PMTCT programs are integrated into each national governmental system of health care, and that the programs adhere to agreed upon standards of implementation. In addition, within each country, the U.S. Government in collaboration with the host government has developed a unified, comprehensive strategy to support the national PMTCT plan and to help provide scaled-up PMTCT services. These U.S. Government strategies document the work plans and budgets of the collaborating agencies and their implementing partners and have been approved by the Ministry of Health in each country. Additionally, the Caribbean Regional program has collaborated with the U.S. Government team to outline regional program objectives for fiscal year 2004, which include the creation of eight centers of excellence, training for 400 health care providers, and the development of regional PMTCT and PMTCT Plus care plans. Limitations in human resources and sites able to provide PMTCT services are major impediments to implementing national PMTCT programs. The President’s Mother and Child Initiative focused on the need to develop capacity in order to effectively scale-up programs. Through the President’s International Mother and Child HIV Prevention Initiative and the Emergency Plan for AIDS Relief, the U.S. Government provided $143 million for PMTCT activities and programs from October 1, 2002, to March 31, 2004. As a result, 14,700 health workers were trained in the provision of PMTCT services and 900 health facilities received financial and technical support, which enabled the provision of a minimum package of PMTCT services, including (1) voluntary counseling and testing for pregnant women, (2) ARV prophylaxis to HIV-infected women to prevent HIV transmission, (3) counseling and support for safe infant feeding practices, and (4) family planning counseling and referral. The focus on training and developing sites for PMTCT lays the foundation for scaling-up national programs, thus making a substantial step towards the Emergency Plan goal of averting seven million new HIV infections. The emphasis on building capacity has led to significant results. During this 18-month reporting period, U.S. Government support directly contributed to 378,000 pregnant women receiving PMTCT services, including voluntary counseling and testing. To date, 34,000 HIV-positive women have received short-course ARV prophylaxis in a PMTCT setting. Estimates based on internationally agreed upon algorithms show that by providing U.S. Government-funded ARV prophylaxis to 34,000 women, 4,800 infant infections have been averted3. The U.S. Government acts as a part of each country’s national effort. During the reporting period, the national programs in focus countries, including U.S. Government-supported activities, provided an estimated 660,000 pregnant women with PMTCT services and provided short course ARV prophylaxis to approximately 76,000 women in 2,600 sites. The U.S. Government-supported progression towards comprehensive, combination ARV treatment for mothers, newborns, other children in the family, and fathers has begun in nearly 60 sites across the 14 target countries.
_______________
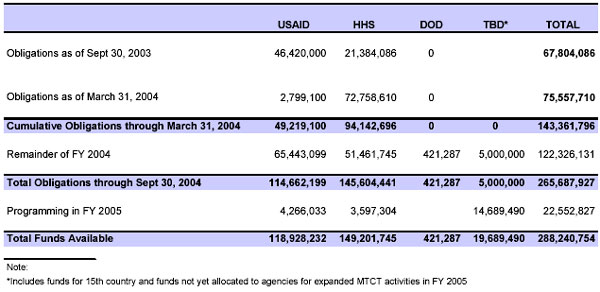
Opportunities The President’s Initiative is already changing the shape of HIV prevention and treatment in the focus countries. In just 18 months, country capacity has been significantly improved; countries that were previously thought to be incapable of providing ARV treatment are scaling up programs that reach pregnant women, their children, and families. With $68 million obligated by the end of fiscal year 2003, countries began the process of building the health care infrastructure needed to respond to the demands of PMTCT and ARV treatment. In the first six months of fiscal year 2004, almost the same amount has been obligated for PMTCT programming. Following a review of country plans, the U.S. Global AIDS Coordinator has recently approved the use of an additional $122 million in PMTCT funds in fiscal year 2004. With increased funding levels, and as the capacity of countries improves, we expect to see a rapid uptake in the numbers of women reached for PMTCT services and families impacted by PMTCT PLUS activities. For example, in Mozambique—a country twice the size of California, with a population of 18 million and a national HIV prevalence rate of 13.6 percent—Emergency Plan funding in 2004 will enable the Ministry of Health to roll out PMTCT services in 31 new sites (50 percent of the total Ministry target for 2004), reaching 64,000 additional pregnant women and treating about 4,200 HIV-positive women and their newborns. In Zambezia Province alone—densely populated, with an adult prevalence rate of 12.5 percent and the worst overall health statistics in the country— three NGO partners, including one faith-based organization, will provide PMTCT services in ten new sites this year. Mozambique is a clear example of how quickly we can expect to see an increase in clients served as U.S. Government funds reach partners on the ground. Silver LiningA PMTCT Success Story from Guyana
Brenda, a mother of one child, is 25 years old and is attending her first antenatal visit in her second pregnancy. During group counseling, the health visitor discussed the transmission of HIV from mothers to infants and ways to reduce this transmission. In the individual session, Brenda who is about twelve weeks pregnant, went through pre-test counseling on HIV, and agreed to be tested.
Brenda did not attend clinic for two months, and later explained to the health visitor that she was experiencing great difficulties in finding a stable place to live, since she had severed her relationship with her partner, who is now residing abroad. During her second visit, the nurse shared her test results for syphilis and hepatitis B, as well as her HIV test result, which was stamped “HIV antibodies detected” in red on the form.
Brenda experienced different emotions; first disbelief then hurt, which was manifested in wailing. It took a while before health workers could calm her, by reassuring her that she could live a healthy life with HIV. Brenda then informed her mother and siblings who, although they were experiencing grief, provided the support she needed to go through the U.S. Government–supported PMTCT program.
Brenda continued her antenatal care, where she received further counseling on infant feeding, safe sex practices, as well as family planning. She also joined a support group of HIV positive mothers at the health center. Four hours before delivery, Brenda received the single-dose anti-retroviral prophylaxis, and the baby received a pediatric dose of nevirapine. As a result, her baby is now HIV free.
After giving birth, Brenda became an advocate and community educator for the Network of People Living with HIV/AIDS in Guyana. She is now permanently employed on a project being implemented by that organization. “Today, I can use myself as an example to talk to other women about HIV/AIDS,” said Brenda, “I am not ashamed of my condition, and feel that I can use my experience to help others.” Brenda is one of 2,788 women in Guyana who have received PMTCT services so far as a result of U.S. Government support. Examples of Program Activities in Key Areas Activities over the last 18 months have centered on strengthening and creating partnerships for service delivery, establishing coordination mechanisms, assisting in the development of national service delivery guidelines, and building infrastructure. These initial successes provide a solid foundation for reaching the HIV transmission reduction goals outlined by President Bush and supported by the Congress.
Service Delivery The President’s Initiative has played a key role in expanding the delivery of PMTCT services in the 14 focus countries and the Caribbean regional program. For example:
A key feature of the President’s Initiative has been the development and implementation of training programs targeted to front-line service providers. During the first year of the Initiative, efforts to build human capacity occurred in all of the focus countries and the one regional program. Select examples include the following:
“Sustainability” is the watchword of the President’s Emergency Plan activities. The transfer of knowledge and expertise to host-country partners is essential to the long-term success of PMTCT and ARV treatment programs for mothers, newborns, and families. In addition to the training programs described above, the U.S. Government has used several other successful strategies in the 14 focus countries and the Caribbean Regional program to ensure a continuing source of reliable information and expertise in diverse settings. Some highlights are as follows:
Partnerships Building and strengthening partnerships and funding mechanisms to coordinate and carry out PMTCT efforts involves bringing together stakeholders, such as Ministries of Health, NGOs, and faith-based organizations for collaborative activities. The process of bringing together diverse sectors with a common goal of reducing the mother-to-child transmission of HIV is working to enhance the early implementation efforts of the Emergency Plan for AIDS Relief. Partnerships among these organizations have taken a variety of forms, from formal funding agreements to coordinating committees. For example:
U.S. Government agencies have been instrumental in providing technical assistance to Ministries of Health for the development or refinement of national PMTCT policies and guidelines. Technical assistance and coordination from the U.S. Government were crucial to the creation of these documents, which in turn set the stage for many other PMTCT activities in these countries. For example:
Commodities, Drugs, Staff, and Lab Infrastructure Support Direct financial and technical support from the U.S. Government has been vital to the acquisition of commodities for PMTCT programs in many of the focus countries. Examples of support include the following:
Key challenges to reducing the rate of mother-to-child transmission of HIV are to ensure that women, families, and communities are aware of the availability and benefits of PMTCT services, receive encouragement to practice healthy and responsible behaviors, and have access to needed care. Accordingly, the President’s Initiative has played a key role in designing and implementing behavior-change communication (BCC) strategies in a number of focus countries during the initial program period. Illustrative examples include the following:
Accountability Critical to ensuring that the President’s Initiative has the desired impact is the collection of strategic information though the monitoring of core indicators, the surveillance of disease trends, and the implementation of special studies and operational research. Some examples of accountability activities supported by the U.S. Government include:
One Child At A TimeA PMTCT Success Story from MozambiqueAlzira Mendes went to the Munhava health center in her neighborhood in the port city of Beira in February 2003 for her first antenatal check-up. Overall HIV prevalence in Sofala province was 26.5 percent in 2002, and prevalence among pregnant women seen at Beira sentinel surveillance sites ranged from 27 to 35 percent that year. A widow at 29 years old, Alzira was six months pregnant with her third child. During her visit, the nurses presented information about HIV and a new program to prevent mother-to-child transmission. Alzira had heard about HIV before this antenatal visit, but she had never chosen to be tested. On this day in February, she decided it was important for herself and her baby to know her HIV status. Flora Vaz, the PMTCT nurse, counseled Alzira about HIV transmission and prevention and about the significance of the HIV test. Nurse Flora used a rapid HIV test and had Alzira’s results within a short time. Upon hearing that she was HIV-positive, Alzira’s first thought was for her baby: how could she prevent the transmission of HIV to her child? Nurse Flora explained that to reduce the chance of transmitting HIV to her child, upon the onset of labor, an HIV-positive woman should come to the maternity ward and take nevirapine, and the baby also should receive one dose of nevirapine within 72 hours of birth. Alzira was happy to enter this program to improve the health of her baby. Nurse Flora also referred Alzira to the Day Hospital at the Beira Central Hospital, which provides care and treatment for HIV-positive individuals. During the final three months of her pregnancy, Alzira participated in a “Positive Mothers” group at the PMTCT program in Munhava. During weekly meetings, HIV-positive pregnant women receive information and counseling about breast-feeding, nutrition, preparing food for their babies, social constraints when living with HIV, stigma, and the importance of having their partners tested. Participants also receive food supplements. In May, Alzira's labor began in the early morning. She immediately went to the health center, received nevirapine, and after a few hours of labor, delivered a baby boy, Apolinário, who also received nevirapine. Following the birth, Alzira joined a support group for HIV-positive moms and their babies at the health center. Both Alzira and Apolinário also continued to go to the Day Hospital for care. When Apolinário was five months old, the Day Hospital tested his viral load to determine his HIV status. Alzira cried with joy and relief when she heard that the viral load was negative, which indicated that her baby was not likely to be infected. Since Alzira is not breast feeding, there is an excellent chance that the baby will still prove HIV-negative at 18 months, when a definitive antibody test can be done. Because of her participation in the PMTCT program, she has given her child an opportunity at a life without HIV. This PMTCT program, fully integrated within the Mozambican public health services, is implemented by Health Alliance International (HAI) in central Mozambique. In 2004, through U.S. Government funding, HAI will be offering integrated PMTCT services in 12 new sites, treating about 3,000 pregnant women and newborns to avert new HIV infections, and providing new hope and services to thousands like Alzira and Apolinário. Facing Programmatic Challenges: Looking to the Future Remarkable strides have been made in the first 18 months of the President’s Initiative and, while challenges have emerged, U.S. Government country teams have responded with creative solutions that can be leveraged as models for scale-up as they are proven to be successful. Among the most critical challenges facing the President’s Initiative are:
The challenges of capacity development cannot be overstated. In the initial stages of the President’s Initiative, there has been heavy emphasis on the development of innovative approaches to the problem of human capacity, particularly among healthcare providers. Some examples of such efforts are:
PMTCT service uptake has not been uniform across all of the focus countries. However, U.S. Government experts have worked closely with country teams to assess the issues and to determine the contributing factors and propose solutions. Some contributing factors that have already been identified include lack of knowledge about PMTCT, stigma associated with being diagnosed with HIV, and opt-in policies for HIV testing that require clients to affirmatively request HIV testing. Sample solutions to low uptake include:
Linkages to Treatment and Care With a long-term vision of building healthy families, the President’s Initiative strongly supports the linkage of PMTCT and PMTCT Plus programs with routine primary health care, HIV care, and reproductive health programs. Recognizing that country programs operate with limited resources, linking services will reduce missed opportunities for achieving critical health goals. Some examples of successful linkages include:
Scale-up Results from several countries indicate that PMTCT pilot projects have had an impact on the numbers of babies infected at or after delivery. The challenge for the 14 focus countries is now to scale-up PMTCT services from pilot projects to national programs that routinely provide PMTCT and PMTCT Plus as part of the healthcare system. One example of how the U.S. Government is supporting scale-up activities in the focus countries can be found in Kenya. To ensure consistent availability of drugs in a scaled-up national program, U.S. technical partners in Kenya are helping to develop an agreement between the Kenya Medical Supplies Agency (public sector medical stores) and the Mission for Essential Drugs and Supplies (NGO medical stores) to establish a “virtual shared inventory.” This approach will ensure that drugs with a less than optimal remaining shelf life will be sent to facilities that can rapidly use them, thus eliminating interruption in drug supplies at both central stores and dispensing sites. Home Deliveries In the focus countries of the Emergency Plan for AIDS Relief, home delivery is common and often the only option. In an effort to ensure that women delivering their babies at home are given access to short-course ARV prophylaxis, and that their babies receive nevirapine within 72 hours of birth, the U.S. Government is supporting innovative models for reaching this subpopulation. In Tanzania, almost 500 traditional birth attendants have been trained to serve as members of the nevirapine outreach groups (NOGs) that follow-up on patients in the community to provide referrals for HIV testing and delivery services for those women who are HIV-positive. Also, these birth attendants are trained to administer a dose of nevirapine if the patient experiences difficulty taking the prescription. Reaching Men and Communities Among the most sensitive issues impacting PMTCT services is the level of involvement of male partners. The engagement of men is critical not only for the well-being of pregnant women and newborns, but also for the entire family unit. When men are invested in the PMTCT process, women have partner support during antenatal care and ARV prophylaxis, and men can be encouraged to learn their own HIV-status through counseling and testing. The U.S. Government has provided support to ensure that men and communities on the whole are educated about the importance of PMTCT services, and to disseminate the message that preventing infections in children is a family and community effort. Some examples of these activities include:
The President’s Emergency Plan for AIDS Relief has an ambitious vision: to turn the tide of the global HIV/AIDS pandemic. This vision, however, will not become reality without dramatic progress in reducing transmission of HIV from mothers to children. The President’s International Mother and Child HIV Prevention Initiative is thus critical to the success of the overall Emergency Plan. Accordingly, the United States has rapidly mobilized its resources. After 18 months of swift and effective action, the President’s PMTCT effort has already produced striking results. So far, the United States has successfully supported the delivery of PMTCT services to 378,000 women in the focus countries, and ARV prophylaxis to 34,000 women. As a result, it is estimated that 4,800 children who would have been infected have been born free of HIV. These results have been achieved during the early, start-up stages of the program. Yet in addition to these immediate benefits, the President’s Initiative has also looked to the future. The United States has invested in the capacity of affected countries to care for their own mothers and children, training 14,700 health workers to deliver PMTCT services, and building capacity at 900 different PMTCT treatment sites. Because the U.S. has made these necessary investments, the provision of services will grow even more rapidly in the days to come. The President’s Initiative is on track to meet its ambitious five-year goal of reducing mother-to-child transmission by 40 percent in the focus countries. The U.S. Government will achieve this goal by providing PMTCT services to one million women, and by providing ARV prophylaxis to 80 percent of HIV-positive women who deliver children. However, we can and must do more than prevent the transmission of HIV from mothers to their newborns. The Emergency Plan has the goal of treating two million HIV-infected persons in the focus countries, including pregnant women and their families. Such longer-term treatment substantially increases the effectiveness of short-course ARV prophylaxis to prevent infections while preserving the health of the mothers, fathers and children. This treatment thereby sustains the family and protects children from the tragedy of becoming orphans. The continued scale-up of the PMTCT effort will make a critical contribution to meeting the Emergency Plan’s overall treatment goals. Even with the impressive results of the PMTCT effort to date, now is not the time for complacency. As long as mothers continue to pass the tragic legacy of HIV/AIDS to their children by transmitting HIV to them or leaving them orphaned, the United States has a moral obligation to sustain the intensity of this effort. Our work today lays a strong foundation to protect the future generations of children from the horrors of HIV/AIDS. Our successes reinforce our commitment to continue reaching mothers, saving children, and building healthy families. Country Results for U.S. Government-Supported Activities
The Power of the Individual – “Femme Active”A PMTCT Success Story from Côte d’IvoireMeet Semi-Lou Bertine – a beautiful young HIV-positive Muslim woman who discovered her HIV-status at the U.S. Government-supported Koumassi clinic in downtown Abidjan. She is also the very loving partner and mother to her husband and HIV-negative child. In the few short years since Semi-Lou learned her HIV-status, she has become a leader within her community and a wonderful example of “positive” living. With initial support from the counselors and the doctors at the Koumassi clinic she founded an HIV-support association called “Femme Active” (Active Women) to ensure other women and their partners receive psychosocial support from their peers. Semi-Lou’s group has also been very active in supporting HIV-positive women and their families to access the comprehensive treatment services available through referral. Through her dynamism and leadership, this organization has rapidly grown in size to more than 300 members and is an active participant in the national network of organizations of persons living with HIV/AIDS in Côte d’Ivoire. After successfully seeking support from the U.S. Government for training some of its members in grant writing, program management, provision of peer-counseling and support and home-based care, the organization has now applied for additional funding from the U.S. Government to expand the quality and coverage of the support, care and advocacy services they provide with their own meager resources. Semi-Lou has also eloquently spoken out on national television and radio and at various public forums about positive living, PMTCT, and fighting discrimination and addressing stigma. She is also contributing to a US Government supported documentary that shares the story of four persons living with HIV in Côte d’Ivoire. Despite more than two decades of HIV in Côte d’Ivoire, the people prepared to publicly acknowledge their HIV-infected status remain rare—this documentary will help to break down the barriers of stigma and discrimination. On a recent pool outing with members of Femme Active, it was wonderful to see young families supporting each other, including the men who were gathering the courage to be tested themselves while being supportive of their HIV-positive wives, as well as the compassionate support for the rare families with HIV-positive children. And all this because
And what is even more amazing is that Semi-Lou, Ami, Rose, Cyriaque, Nathalie, Christine and the many others like them are inspiring more and more HIV-infected persons to unite, care for each other, advocate for treatment and expanded services, and fight the fear and ignorance that is the basis of stigma and discrimination. Together anything is possible…. |