Childhood Cancer
What Is Cancer?
When Your Child Is Diagnosed
Talking with Your Child
What About Treatment?
Common Medical Procedures
Common Health Issues
When to Call the Doctor
Moving on With Life
What Does the Future Hold?
When the Cancer Cannot Be Cured
Resources
Types of Childhood Cancer
Childhood Cancer
Young People with Cancer gives you information on all stages of
your child's illness. It tells you what to expect and suggests ways
to prepare for different situations. It can guide you to become your
child's best advocate or supporter. You know your child better
than anyone else - your child's personality, how your child copes
with unknown situations and fear, what makes your child laugh or
cry. You know what works best - how to humor and talk to your
child and how to help your child relax. Try to remember that you
are a key part of your child's treatment.
This booklet was reviewed by health professionals and, most
important, by parents of children with cancer. Although this booklet
does not tell you everything about cancer in children, it is a
start, and it directs you to other sources of information. You may
want to share this booklet with friends and relatives who want to
learn more about what you and your child are going through. Use
this booklet to learn:
- what cancer is and what the different kinds of cancer are
- how to find the best treatment
- about cancer treatment and side effects
- about common medical procedures
- how to talk to your child about cancer
- how to handle your own feelings, your child's feelings, and
the feelings of others
- about common health issues
- what the future holds and
- where to get more information.
Because this booklet contains so much information, it may be
useful to refer to the different sections as you need them. You can
use the Table of Contents to find the sections of most interest to
you. Words that you may not be familiar with are underlined the first time they appear. You can click on these words to see their definitions. The definitions are taken from the National Cancer Institute's Cancer.gov dictionary 1.
More children than ever are surviving childhood cancer. Over
the last 30 years, survival into adulthood increased from 30 percent
to 80 percent. There are new and better drugs and methods to
help children deal with the side effects of treatment. And children
who have had cancer now have a better quality of life throughout
childhood and into adulthood; fewer long-term ill effects follow
the treatment.
Yet, in spite of all this good news, cancer is still a serious
disease. You are not alone in facing your fears; help is available.
A treatment team - doctors, radiation therapists, rehabilitation
specialists, dietitians, oncology nurses,
and social
workers, among
others - can help you and your child deal with the disease. They
will also help ensure that your child gets the best treatment available
with as few ill effects as possible. Resources such as this booklet
provide information on childhood cancers and their treatment,
suggestions on how to make your child as comfortable and as
pain-free as possible, and advice on how to make time for family
and friends.
What Is Cancer?
Cancer is a group of many related diseases that begin in cells,
the body's basic unit of life. To understand cancer, it is helpful to
know what happens when normal cells become cancerous.
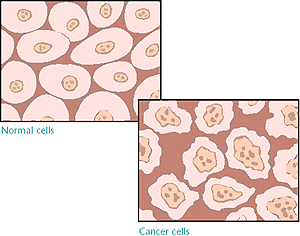
The body is made up of many types of cells. Normally, cells
grow and divide to produce more cells only when the body needs
them. This orderly process helps keep the body healthy. Sometimes,
however, cells keep dividing when new cells are not needed.
These extra cells form a mass of tissue called a growth or
tumor.
Tumors can be
benign
or
malignant.
- Benign tumors are not cancer. They can often be removed
and, in most cases, they do not come back. Cells from
benign tumors do not spread to other parts of the body.
Most important, benign tumors are rarely a threat to life.
- Malignant tumors are cancer. Cells in these tumors are
abnormal and divide without control or order. They can
invade and damage nearby tissues and organs. Also, cancer
cells can break away from a malignant tumor and enter the
bloodstream or the lymphatic system. That is how cancer
spreads from the original cancer site to form new tumors in
other organs. Cancer that has spread is called
metastatic cancer.
Most cancers are named for the organ or type of cell in which
they begin. When cancer spreads (metastasizes), cancer cells are
often found in nearby or regional
lymph nodes
(sometimes called
lymph glands). If the cancer has reached these nodes, it means
that cancer cells may have spread to other organs, such as the
liver, bones, or brain. When cancer spreads from its original location
to another part of the body, the new tumor has the same
kind of abnormal cells and the same name as the primary tumor.
For example, if lung cancer spreads to the brain, the cancer cells
in the brain are actually lung cancer cells. The disease is called
metastatic lung cancer (not brain cancer).
Children can get cancer in the same parts of the body as adults
do, but some types of cancer are more common in children. The
most common form of childhood cancer is
leukemia. Leukemia is
cancer of the blood. It develops in the
bone marrow, which is a
spongy substance that fills the inside of the bones and makes
blood cells. Other cancers often found in children are brain
tumors, childhood
lymphomas, Hodgkin's disease, Wilms'
tumors, neuroblastomas, osteogenic sarcomas, Ewing's sarcomas,
retino-blastomas, rhabdomyosarcomas and hepatoblastomas. The
Appendix contains information on the major types of
childhood cancer.
Children's cancers do not always act like, get treated like, or
respond like adult cancers. Avoid reading about adult cancer to
learn about your child's prognosis. Childhood cancers can occur
suddenly, without early symptoms, and have a high rate of cure.
You can find more details about these types of cancer in other
National Cancer Institute (NCI) booklets. NCI's What You Need to
Know About... brochures have information about specific types of
cancer. (See page 96 for more information on available booklets.)
To receive copies from the NCI-supported Cancer Information
Service (CIS), call 1-800-4-CANCER (1-800-422-6237) or TTY at
1-800-332-8615. Also, many NCI publications may be viewed or
ordered on the Internet at http://cancer.gov/publications.
When Your Child Is Diagnosed

After your child's cancer has been diagnosed, a series of tests will be done to
help identify your child's specific type of cancer. Called staging, this series
of tests is sometimes done during diagnosis. Staging determines how much cancer
is in the body and where it is located. To stage solid tumors, the doctor looks
at the size of the tumor, the lymph nodes affected, and where it has spread. To
stage leukemia, the doctor checks the bone marrow, liver, spleen, and lymph
nodes around the sites where the leukemia can hide. Staging must be done to
determine the best treatment. Many different tests can be used in staging, such
as
x-rays,
MRIs,
CT (or CAT)
scans, and others. See
Common Medical Procedures 2
for a description of the various tests.
As soon as your child is suspected to have or is diagnosed with cancer, you
will face decisions about who will treat your child, whom to ask for a second
opinion (if desired or if the diagnosis is not clear), and what the best
treatment is. After your child's staging is complete, the treatment team
develops a plan that outlines the exact type of treatment, how often your child
will receive treatment, and how long it will last.
 Your child's doctor and the treatment team will give you a lot of details about
the type of cancer and possible treatments. Ask your doctor to explain the
treatment choices to you. It is important for you to become a partner with your
treatment team in fighting your child's cancer. One way for you to be actively
involved is by asking questions. You may find it hard to concentrate on what
the doctor says, remember everything you want to ask, or remember the answers
to your questions. Here are some tips for talking with those who treat your
child:
Your child's doctor and the treatment team will give you a lot of details about
the type of cancer and possible treatments. Ask your doctor to explain the
treatment choices to you. It is important for you to become a partner with your
treatment team in fighting your child's cancer. One way for you to be actively
involved is by asking questions. You may find it hard to concentrate on what
the doctor says, remember everything you want to ask, or remember the answers
to your questions. Here are some tips for talking with those who treat your
child:
-
Write your questions in a notebook and take it to the appointment with you.
Record the answers to your questions and other important information.
-
Tape record your conversations with your child's health care providers.
-
Ask a friend or relative to come with you to the appointment. The friend or
relative can help you ask questions and remember the answers.
|
Questions to Ask the Doctor and Treatment Team
When your child's treatment team gives you information about your child's
cancer, you may not remember everything. That is natural. It is a lot of
information, and your emotions will get in the way as you try to take it all
in. Use the three techniques listed above - write, tape record, and ask a
friend for help - to help you retain the information you need to be an
effective partner with your child's treatment team. Make sure you know the
answers to these questions:
About the diagnosis
-
What kind of cancer does my child have?
-
What is the stage, or extent, of the disease?
-
Will any more tests be needed? Will they be painful? How often will they be
done?
About treatment choices
-
What are the treatment choices? Which do you recommend for my child? Why?
-
Would a
clinical trial
be right for my child? Why?
-
Have you treated other children with this type of cancer? How many?
-
What are the chances that the treatment will work?
-
Where is the best place for my child to receive treatment? Are there
specialists - such as surgeons, radiologists, nurses, anesthesiologists, and
others - trained in
pediatrics? Can my child have some or all of the treatment in our
home town?
About the treatment
-
How long will the treatment last?
-
What will be the treatment schedule?
-
Whom should we ask about the details of financial matters?
-
Will the treatment disrupt my child's school schedule?
About side effects
-
What possible side effects of the treatment can occur, both right away and
later?
-
What can be done to help if side effects occur?
About the treatment location
-
How long will my child be in the hospital?
-
Can any treatment be done at home? Will we need any special equipment?
-
Does the hospital have a place where I can stay overnight during my child's
treatment?
About school and other activities
-
Is there a
child-life worker
specialist (a professional who is responsible for making the hospital and
treatment experience less scary for the child) to plan play therapy,
schoolwork, and other activities?
-
When can my child go back to school?
-
Are there certain diseases my child cannot be around? Should I have my child
and his or her siblings immunized against any diseases?
-
Will my child need tutoring?
-
Is information available to give to the school system about my child's needs as
he or she receives treatment?
|
Before your child starts treatment, make sure you feel comfortable with your
choice of the doctor and hospital to treat your child's cancer.
Who Should Treat My Child?
 It is best for your child to be treated by a health care provider who
specializes in the diagnosis and treatment of children's cancers - a pediatric
oncologist.
It is best for your child to be treated by a health care provider who
specializes in the diagnosis and treatment of children's cancers - a pediatric
oncologist.
Once you have chosen a doctor and discussed a diagnosis and treatment plan, but
before treatment has started, you may want to get a second opinion - that is,
you may want to ask a different doctor to review the diagnosis and plan. Some
insurance companies require a second opinion; some may pay for it if you ask. A
second opinion may also be obtained during the course of treatment if it is not
working as hoped. Most doctors support a parent's decision to get a second
opinion and many even suggest you do so. To find specialists to get a second
opinion, you might -
-
Ask your child's doctor to suggest a specialist for a second opinion.
-
Get the names of doctors who specialize in treating childhood cancer from the
local medical society, a nearby hospital, or a medical school. You can find the
telephone numbers for these organizations in your telephone directory or the
Yellow Pages.
-
Contact an NCI Comprehensive Cancer Center for a second opinion and possible
treatment. Considered "Centers of Excellence," these cancer centers' programs
have been reviewed and selected by NCI. They offer the most up-todate diagnosis
and treatment of cancer and are devoted to both basic and clinical research. To
obtain information about the location of the different cancer centers, call the
CIS at 1-800-4-CANCER (1-800-422-6237) or TTY at 1-800-332-8615.
-
Contact the Pediatric Oncology Branch, NCI, located in Bethesda, Maryland, to
ask for a second opinion appointment. They can be reached at 1-877-624-4878.
What Is a Standard Therapy Versus a Clinical Trial?
Your child's doctor may recommend a
standard therapy
or a clinical trial. Standard therapy is the best treatment available outside
of clinical trials for a specific type and stage of cancer.
A cancer clinical trial is a research study. In a clinical trial, a new
treatment is used with a group of patients to find out:
-
if it is safe
-
if it destroys the cancer
-
if it has side effects and how severe they might be
-
if it is better than standard therapy.
These new treatments are first tested in the laboratory and on animals. If a
treatment shows promise of being better than the standard therapy, it is tested
with patients in a clinical trial.
Most clinical trials are carried out in steps called phases. Each phase answers
different questions about the treatment. Patients may be eligible for studies
in different phases, depending on their general condition and the type and
stage of their cancer.
-
Phase I studies
test new treatments in humans to determine if the treatment can be given safely
and if it has harmful side effects. Researchers look for the best dose and the
best way to deliver the treatment. Because less is known about the possible
risks and benefits in Phase I, these studies usually include only a limited
number of patients who would not be helped by other treatments.
-
Phase II studies
focus on learning whether the new treatment actually has an anticancer effect.
As in Phase I, only a small number of people take part because of the risks and
unknowns involved.
-
Phase III studies
compare the results of people receiving the new treatment with results of
people receiving standard therapy. In most cases, studies move into Phase III
testing only after a treatment shows promise in Phases I and II. Phase III
studies may include hundreds of people around the country.
-
Phase IV studies
evaluate the side effects of the new treatment - once it has been approved and
is being marketed - that were not apparent in the Phase III trial. Thousands of
people are involved in a Phase IV trial.
Clinical trials have played an important role in producing new and better
treatments. About two-thirds of children with cancer are treated in clinical
trials
You and your child's doctor can learn about clinical trials from PDQ® -
NCI's cancer information database. PDQ® contains:
-
descriptions of current clinical trials, including information about the
purpose of the study, who is eligible for the study, details of the treatment
program, and the names and addresses of doctors and places conducting the study
You may ask your doctor to obtain
information from PDQ®, or you may call the NCI-supported Cancer Information
Service (CIS) at 1-800-4-CANCER (1-800-422-6237) or TTY at 1-800-332-8615 to
ask for a PDQ® search 3. Read more
about
PDQ® 4 on the NCI Web site, Cancer.gov 5. To find
out about NCI trials taking place on the main campus of the National Institutes
of Health in Bethesda, Maryland, you may also call the NCI's Pediatric Oncology
Branch at 1-877-624-4878.
Where Should My Child Be Treated?
Once the treatment is planned, you will need to decide where your child will be
treated. Treating children is different from treating adults. Whenever
possible, it is best for your child to begin treatment at a hospital or
treatment center where many children have been treated for cancer. Selecting a
hospital and staff specializing in treating childhood cancer will help your
child receive the best available treatment right from the beginning. To obtain
information about hospitals and treatment centers that specialize in treating
childhood cancer, call the CIS at 1-800-4-CANCER (1-800-422-6237) or TTY at
1-800-332-8615.
Talking with Your Child
Your first question may be, "Should I tell my child about the cancer?" You may
want to protect your child, but children usually know when something is wrong.
Your child may not be feeling well, may be seeing the doctor often, and may
have already had some tests. Your child may notice that you are afraid. No
matter how hard you try to keep information about the illness and treatment
from your child, others - such as family, friends, and clinic or hospital staff
- may inadvertently say things that let your child know about the cancer. In
addition, it will upset your child to find out that you were not telling the
truth; your child depends on you for honest answers.
Telling your child about his or her cancer is a personal matter, and family,
cultural, or religious beliefs will come into play. It is important to be open
and honest with your child because children who are not told about their
illness often imagine things that are not true. For example, a child may think
he or she has cancer as punishment for doing something wrong. Health
professionals generally agree that telling children the truth about their
illness leads to less stress and guilt. Children who know the truth are also
more likely to cooperate with treatment. Finally, talking about cancer often
helps to bring the family closer together and makes dealing with the cancer a
little easier for everyone.
Parents have many questions about talking with their children about the
diagnosis. Perhaps you have asked some of these yourself.
When Should My Child Be Told?
Because you are probably the best judge of your child's personality and moods,
you are the best person to decide when your child should be told. Keep in mind,
though, that your child is likely to know early on that something is wrong, so
you may want to tell your child soon after the diagnosis. In fact, most parents
say it is easiest to tell them then. Waiting days or weeks may give your child
time to imagine worse things than the truth and develop fears that may be hard
to dispel later. Certainly, it would be easier for your child if he or she is
told before treatment starts.
Who Should Tell My Child?
The answer to this question is personal. As a parent, you may feel that it is
best for you to tell your child. Some parents, however, find it too painful to
do so. Other family members or the treatment team - doctor, nurse, or social
worker - may be able to help you. They may either tell your child for you or
help you explain the illness.
Thinking about what you are going to say and how to say it will help you feel
more relaxed. But how do you decide just what to say? Family and close friends,
members of the treatment team, parents of other children who have cancer,
members of support groups (you can find information about them at the end of
this booklet), and clergy members can offer ideas.
Who Should Be There?
Your child needs love and support when hearing the diagnosis. Even if the
doctor explains the illness, someone your child trusts and depends upon should
be present. Having the support of other family members at this time can be very
helpful.
What Should My Child Be Told?
How much information and the best way to relate this information depends on
your child's age and what your child can understand. Being gentle, open, and
honest is usually best.
The following sections describe what most children in various age groups are
likely to understand. These guidelines are general; each child is different.
Your child may fit into more than one or none of these categories.

-
Up to 2 Years Old
Children this young do not understand cancer. They understand what they can see
and touch. Their biggest concern is what is happening to them right now. They
worry most about being away from their parents.
After children are a year old, they think about how things feel and how to
control things around them. Very young children are most afraid of medical
tests. Many cry, run away, or squirm to try to control what is happening.
Because children begin to think about and understand what is going on around
them at about 18 months, it is best to be honest. Be truthful about trips to
the hospital and explain procedures that may hurt. You can tell your child that
needle sticks will hurt a minute and that it is okay to cry. Being honest lets
your child know that you understand and accept his or her feelings and helps
your child trust you.
When you can, give your child choices. For example, if a medicine is taken by
mouth, you might ask if your child would like it mixed in apple juice, grape
juice, or applesauce.
-
2 to 7 Years Old
When children are between the ages of 2 and 7, they link events to one thing.
For example, they usually tie illness to a specific event such as staying in
bed or eating chicken soup. Children this age often think their illness is
caused by a specific action. Therefore, getting better will "just happen" or
will come if they follow a set of rules.
These approaches might help when talking with a child in this age group:
-
Explain that treatment is needed so the hurting will go away or so the child
can get better and play without getting so tired.
-
Explain that the illness or treatment is not punishment for something the child
has done, said, or thought.
-
Be honest when you explain tests and treatments. Remind the child that all of
these things are being done to get rid of the cancer and to help him or her get
well.
-
Use simple ways to explain the illness. For example, try talking about the
cancer as a contest between "good" cells and "bad" cells. Having treatment will
help the good cells to be stronger so that they can beat the bad cells.
-
7 to 12 Years Old
Children ages 7 to 12 are starting to understand links between things and
events. For example, a child this age sees his or her illness as a set of
symptoms, is less likely to believe that something he or she did caused the
illness, understands that getting better comes from taking medicines and doing
what the doctor says, and is able to cooperate with treatment.
You can give more details when explaining cancer, but you should still use
situations your child may be used to. You might say that the body is made of up
different types of cells, and these cells have different jobs to do. Like
people, these cells must work together to get the job done. You might describe
the cancer cells as "troublemakers" that get in the way of the work of the good
cells. Treatment helps to get rid of the troublemakers so that other cells can
work well together.
-
12 Years and Older
Children over 12 years old can often understand complicated relationships
between events. They can think about things that have not happened to them.
Teenagers tend to think of illness in terms of specific symptoms, such as
tiredness, and in terms of limits or changes in their everyday activity. But
because they also can understand the reason for their symptoms, you can explain
cancer as a disease in which a few cells in the body go "haywire." These
"haywire" cells grow more quickly than normal cells, invade other parts of the
body, and get in the way of how the body usually works. The goal of treatment
is to kill the "haywire" cells. The body can then work normally again, and the
symptoms will go away.
Children are naturally curious about their disease and have many questions
about cancer and cancer treatment. Your child will expect you to have answers
to most questions. Children may begin to ask questions right after diagnosis or
may wait until later. Here are some common questions and some ideas to help you
answer them.
Why Me?
A child, like an adult, wonders "Why did I get cancer?" A child may feel that
it is his or her fault, that somehow he or she caused the illness. Make it
clear that not even the doctors know exactly what caused the cancer. Neither
you, your child, nor his or her brothers or sisters did, said, or thought
anything that caused the cancer. Stress also that cancer is not contagious, and
your child did not "catch" it from someone else.
Will I Get Well?
Children often know about family members or friends who died of cancer. As a
result, many children are afraid to ask if they will get well because they fear
that the answer will be "no." Thus, you might tell your child that cancer is a
serious disease, but that treatment - such as medicine, radiation, or an
operation - has helped get rid of cancer in other children, and the doctors and
nurses are trying their best to cure your child's cancer, too. Knowing that
caring people - such as family, doctors, nurses, counselors, and others -
surround your child and your family may also help him or her feel more secure.
What Will Happen to Me?
When your child is first diagnosed with cancer, many new and scary things will
happen. While at the doctor's office, hospital, or clinic, your child may see
or play with other children with cancer who may not be feeling well, have lost
their hair, or have had limbs removed because of cancer. Your child may wonder,
"Will these things happen to me?" Yet, your child may be too afraid to ask
questions. It is important to try to get your child to talk about these
concerns. Explain ahead of time about the cancer, treatment, and possible side
effects. Discuss what the doctor will do to help if side effects occur. You can
also explain that there are many different types of cancer and that even when
two children have the same cancer, what happens to one child will not always
happen to the other.
Children should be told about any changes in their treatment schedule or in the
type of treatment they receive. This information helps them prepare for visits
to the doctor or hospital. You may want to help your child keep a calendar that
shows the days for doctor visits, treatments, or tests. Do not tell younger
children about upcoming treatments far ahead of time if it makes them nervous.
Why Do I Have to Take Medicine When I Feel Okay?
With cancer, your child may feel fine much of the time but need to take
medicine often. Children do not understand why they have to take medicine when
they feel well. You may want to remind your child of the reason for taking the
medicine in the first place. For example, a child could be told: "Although you
are feeling well, the bad cells are hiding. You must take the medicine for a
while longer to find the bad cells and stop them from coming back."
What About Treatment?

To plan the best treatment, the doctor and treatment team will look at your
child's general health, type of cancer, stage of the disease, age, and many
other factors. Based on this information, the doctor will prepare a treatment
plan that outlines the exact type of treatment, how often your child will
receive treatment, and how long it will last. Each child with cancer has a
treatment plan that is chosen just for that child; even children with the same
type of cancer may receive different treatments. Depending on how your child
responds to treatment, the doctor may decide to change the treatment plan or
choose another plan.
Before treatment begins, your child's doctor will discuss the treatment plan
with you, including the benefits, risks, and side effects. Then you and the
treatment team will need to talk with your child about the treatment. After the
doctor fully explains the treatment and answers your questions, you will be
asked to give your written consent to go ahead with treatment. Depending on
your child's age and hospital policy, your child may also be asked to give
consent before treatment.
The treatment plan may seem complicated at first. But the doctor and treatment
team will explain each step, and you and your child will soon become used to
the routine. Many parents find it helpful to get a copy of the treatment plan
to refer to as the treatment proceeds. It also helps them in arranging their
own schedules. Do not be afraid to ask questions or speak up if you feel
something is not going right. Your child's doctor is often the best person to
answer your questions, but other members of the treatment team can give you
information, too. If you feel as though you need extra time with the doctor,
schedule a meeting or phone call. Remember, you are part of the treatment team
and should be involved in your child's treatment.
The types of treatment used most often to treat cancer are
surgery,
chemotherapy,
radiation therapy,
immunotherapy, and
bone marrow or
peripheral blood stem cell transplantation . Doctors use these
treatments to destroy cancer cells. Depending on the type of cancer, children
may have one kind of treatment or a combination of treatments. Most children
receive a combination of treatments, called
combination therapy.
Treatments for cancer often cause unwanted or unpleasant side effects such as
nausea, hair loss, and diarrhea. Side effects occur because cancer treatment
that kills cancer cells can hurt some normal cells, too. As your child begins
treatment, you may want to keep the following in mind.
-
The kinds of side effects and how bad they will be depend on the kind of drug,
the dosage, and the way your child's body reacts.
-
The doctor plans treatment so that your child has as few side effects as
possible.
-
The doctor and treatment team have ways to lessen your child's side effects.
Talk with them about things that can be done before, during, and after
treatment to make your child comfortable.
-
Lowering the treatment dosage slightly to eliminate unpleasant side effects
usually will not make the treatment less able to destroy cancer cells or hurt
your child's chances of recovery.
-
Most side effects go away soon after treatment ends.
Remember that not every child gets every side effect, and some children get
few, if any. Also, how serious the side effects are varies from child to child,
even among children who are receiving the same treatment. The doctor or
treatment team can tell you which, if any, side effects your child is likely to
have and how to handle them. If you know what side effects can occur, you can
recognize them early.
| For many solid tumors, surgery is an essential part of the treatment. Surgery
is a local therapy to remove the tumor. Tissue around the tumor and nearby
lymph nodes may also be removed during the operation. Sometimes radiation or
chemotherapy is used first to shrink the tumor before it is removed. Shrinking
the tumor makes the surgery easier.
|
Helping Your Child Face Fears About Surgery
Your child is likely to have many worries about surgery. Your child may ask:
-
What is it like to be put to sleep?
-
Will I feel a lot of pain?
-
Will my body be changed?
-
How will I feel about my body after the operation?
-
Will my parents be with me when I wake up?
Here are some suggestions that might help your child face surgery:
-
Give honest answers to your child's questions.
Your child may lose trust in you if what you say does not match what really
happens. Your child needs to trust you.
-
Learn as much as you can about your child's operation.
To give the correct answers to your child's questions, you will need to find
out as much as possible about what will happen. The doctors and other members
of the treatment team can give you the facts you need to prepare your child.
-
Visit the operating and recovery rooms before the surgery.
To help children get ready for surgery, many hospitals encourage them to visit
the rooms where they will be during surgery and recovery. They can meet and
talk with the people who will be there. For instance, young children may be
shown a surgical mask and given one to try on or to put on a toy or another
person.
-
Talk with your child about feelings and concerns.
Above all, try to get your child to talk about any feelings or concerns he or
she has about the surgery.
Possible Side Effects of Surgery
Side effects from surgery depend on the location of the tumor, the type of
operation, the child's general health, and other factors. Common side effects
include pain, headaches, nausea, and constipation. These effects may be from
the surgery, pain medicine, or lack of exercise. The doctor will give your
child medicine, as needed, to help ease these side effects and other symptoms.
Children and Amputations
In the past, amputations were often necessary to remove bone tumors in the arms
and legs. Depending on the type of tumor, however, doctors more and more can
use procedures that spare the limb and make amputation unnecessary. Fewer
children suffer the loss of a limb. Your child's treatment team will explain
the options available to you.
For some children, however, amputation remains the best choice. These children
have special concerns. They wonder what it will be like not to have an arm or
leg. Will they be able to do everyday things? How will they do them? How will
others act toward them? They may feel a lack of wholeness after surgery.
Sometimes it is more difficult for parents than for children to adjust to an
amputation. Generally, younger children adjust more quickly. Adolescents have
special concerns. They may be more sensitive about the way they look to others.
They also may worry about how the amputation will affect developing and keeping
relationships, participating in sports activities, getting married, and having
children.
It may be helpful for your child to see how others have adjusted to an
amputation. Meeting other children who have had amputations and who are doing
well can be very helpful. Your child will learn that he or she can have a full
and active life - most children can participate in the same activities they did
before having an amputation. They can still walk, run, ride a bicycle, ski,
swim, and even mountain-climb. It may also help for the treatment team to show
your child an artificial limb, or
prosthesis, and other devices or aids that will help with movement.
After surgery, your child will be aware of a bulky dressing or bandage at the
site of the surgery. Your child may feel "phantom pain," an eerie but common
feeling. Sensations such as cold, itching, and pain are felt in the limb as if
it were still part of the body. Doctors do not know what causes phantom pain.
The best explanation is that the brain has been accustomed to receiving
messages from the nerves in the limb that has been amputated. It takes time for
the brain to get used to the nerve fibers that remain and the new messages from
the stump. Sometimes a light massage and changing the position of the stump
will offer some relief. The doctor will usually start medication ahead of time
to ease your child's pain and can also order some medicine to treat the phantom
pain when it happens.
As part of the rehabilitation, a physical therapist will help your child with
exercises to strengthen the muscles needed to support a temporary prosthesis.
These exercises are often hard and can be painful, so your child needs to be
encouraged and supported during this time. Once the muscles become stronger,
the doctor may order a temporary prosthesis for your child. The prosthesis is
made by a prosthetist, a person skilled in making artificial limbs. The
temporary prosthesis will be bulkier and heavier than the permanent one. The
way it looks may be disappointing, but the added heaviness will further
strengthen the stump and the bulkiness will protect it. Once the stump is fully
healed, and your child is able to move the limb well with the temporary
prosthesis, fitting for the permanent prosthesis will begin.
Health professionals will be available to help your child and family throughout
the entire process - from making treatment choices to adjusting to the
permanent prosthesis. Drawing upon the strength and comfort of family members
and joining a support group may also help you cope.
|
Chemotherapy is the use of "anticancer drugs" to treat cancer. Chemotherapy is
systemic therapy, which means that the drugs flow through the
bloodstream to nearly every part of the body to kill cancer cells wherever they
may be. Because some anticancer drugs work better together than alone,
chemotherapy may consist of more than one drug. This approach is called
combination chemotherapy.
|
Depending on the type of cancer your child has and which drugs are used,
chemotherapy may be given in one or more of these ways:
-
By mouth (oral medication) - The drugs are swallowed in liquid or pill
form. If your child has trouble swallowing pills, you can break the pills into
smaller pieces, or you may crush and mix them with applesauce, jam, pudding, or
other food that your child likes.
-
Intravenously (IV) - The drugs are injected by needle into a vein or
into an IV line.
-
Intramuscular injection (IM) - The drugs are injected by needle into the
muscle. Your child will know it as a "shot."
-
Subcutaneous injection (SC) - The drugs are injected by needle just
below the skin. Your child will also know this as a "shot."
-
Intrathecal injection (IT) - The drugs are injected by needle into the
spinal fluid
Although your child may be able to receive chemotherapy treatments at home, he
or she will probably need to go to the hospital or doctor's office to receive
IV drugs or injections. Depending on the medicine, your child may need to stay
in the hospital, perhaps overnight or longer. 
Oral Chemotherapy
When possible, involve your child in this treatment. For example, you may want
to keep a special calendar to help your child track when medicine should be
taken. Older children, particularly adolescents, may want to be responsible for
taking and keeping track of their medication. Even so, you still need to make
sure that the medicine is being taken as ordered. Be sure to notify the doctor
if your child misses any doses of medication or if he or she vomits them up.
Intravenous Chemotherapy
Your child will get the drug through a thin needle put into a vein, usually on
the hand or in the arm. In babies and very small children, the needle may be
placed in a vein in the scalp. Although getting chemotherapy usually does not
hurt, it may be painful when the IV needle is put in, and the drugs may cause a
burning feeling. If the drug leaks from the vein, it may burn the skin, so care
must be taken to make sure the IV line is firmly in place. The nurse or doctor
must act right away if the needle comes out of the vein.

Another way to give IV chemotherapy is through a
catheter. The catheter remains in place during the course of treatment so that drugs
can be given without having to place a needle into the vein over and over
again. The most commonly used are central venous catheters. While the child is
under general or local anesthesia, the catheter is usually put into a large
vein in the chest by making a small incision (cut) near the collarbone. Two
types of central venous catheters are commonly used.
-
One type of catheter is an external venous catheter (for example, a Broviac or
Hickman catheter). In this type of catheter, the plastic tube extends outside
the body.
-
The second type (for example, a Port-a-Cath catheter) is placed under the skin
and needs to have a needle placed into it each time it is used. This type of
catheter may be more appealing to adolescents or for families who cannot take
care of a catheter that needs special daily care.
In addition to chemotherapy, pain medicine and blood transfusions can be given
through the catheter, and blood can be drawn from the body through the
catheter.
Side Effects of Chemotherapy
Side effects can occur when the anticancer drugs affect not only the cancer
cells but healthy cells as well. Different drugs produce different side
effects. Ask your doctor or nurse what side effects your child is most likely
to have and when they are likely to occur. Side effects are either acute (they
happen right away) or delayed (they happen days, weeks, or years after
chemotherapy). The most common side effects of chemotherapy are listed in the
following chart.
You may also find these NCI materials useful:
You can receive copies from the NCI-supported Cancer Information Service (CIS)
by calling 1-800-4-CANCER (1-800-422-6237) or TTY at 1-800-332-8615. Also, many
NCI publications may be viewed or ordered
online 8.
Side Effects of Chemotherapy:
DIGESTIVE TRACT PROBLEMS
| Side Effect |
What You Can Do |
|
| Nausea and Vomiting |
-
Ask your child's doctor about medicines to control nausea and vomiting and/or
sedatives to help your child sleep through nausea.
-
Ask your doctor if it is alright to give your child milk or antacids before
taking oral anticancer drugs. Certain oral anticancer drugs should not be taken
with milk.
-
Feed your child light foods 3-4 hours before treatment.
-
Encourage your child to eat small amounts of food often and slowly.
-
Avoid serving sweet, greasy, and spicy foods or foods that have strong odors.
-
Serve your child cold meals, such as sandwiches, instead of hot foods.
-
Encourage your child to take liquids first, and then wait 30-60 minutes before
eating solids. Most children tolerate liquids better than solids.
-
Have your child rest after meals.
-
If your child is vomiting, do not give anything to eat or drink until it is
under control. Once the vomiting is under control, give small amounts of clear
liquids (for example, water, broth, milk-free ices, and gelatin desserts).
Begin with 1 teaspoon every 10 minutes; gradually increase the amount to 1
tablespoon every 20 minutes; and, finally, try 2 tablespoonfuls every 30
minutes. When your child can keep down clear liquids, try denser liquids (for
example, strained cereal, pudding, yogurt, milkshakes, cream soups). Give small
amounts as often as your child can keep them down. Gradually work up to solid
foods.
|
| Diarrhea |
-
Contact your doctor if your child's diarrhea is severe; that is, more than
three loose stools per day.
-
Avoid giving your child fatty foods.
-
Try serving foods that are high in proteins and calories but low in fiber, such
as plain or vanilla yogurt, rice with broth, or noodles.
-
Serve your child foods and liquids that are high in sodium and potassium. Foods
high in potassium that do not cause diarrhea are bananas, peach and apricot
juices, and boiled or mashed potatoes.
|
| Constipation |
-
Call your doctor if your child goes more than 2 days without having a bowel
movement.
-
Encourage your child to drink more fluids, such as apple juice.
-
Make sure your child gets some exercise.
-
Serve your child high-fiber foods, such as wholegrain breads and cereals; brown
rice; dried fruits, such as raisins and prunes; and raw fresh vegetables.
|
| Heartburn or stomach ache |
-
Ask your child's doctor about giving your child an antacid.
-
Avoid serving your child
foods that are
fried, greasy or very spicy.
|
|
MOUTH PROBLEMS
| Side Effect |
What You Can Do |
|
| Sore mouth or throat, mouth sores |
-
Ask your child's doctor for medicine (sprays, special mouthwashes, and
lozenges) for your child's mouth.
-
Give your child a sponge toothbrush or cotton swab to brush his or her teeth.
-
Have your child rinse his or her mouth every 2-3 hours and after meals, using
baking soda solution or water.
-
Avoid serving very cold, hot, spicy, or acidic foods.
-
Try serving soft foods.
-
Contact your child's doctor if your child has mouth sores, painful areas, or
patches of red or white in the mouth.
|
| Change in taste - foods have less
taste or a bitter metallic taste |
Try well-seasoned foods or tart foods such as oranges,
lemonade, or lemon tart. (Do not try these foods if your child has a sore
mouth, throat, or gums.) Pizza and taco chips frequently become children's
favorite foods.
|
|
SKIN AND HAIR PROBLEMS
| Side Effect |
What You Can Do |
|
| Hair loss |
-
Use a mild shampoo.
-
Cut your child's hair short.
-
Avoid using hair dryers and electric curlers.
-
Use a wide-tooth comb.
-
If you are planning to have your child wear a wig, select it before all your
child's hair comes out.
-
If you want to cover your child's head, try a variety of hats and scarves.
-
Protect your child's scalp from sun and cold.
|
| Redness of skin |
Call your doctor if redness, pain, or swelling occurs.
|
| Dry, itching skin |
Use mild soap and moisturizers. (If the child is receiving
radiation therapy, check with your child's doctor before using moisturizer.)
|
| Moist skin |
Wash your child's skin 2-3 times each day. Pat dry with a
clean towel and lightly powder with cornstarch. |
| Rashes |
Call your child's doctor, who may order medication.
|
| Sun sensitivity |
-
Avoid sun exposure.
-
Use an SPF 30 or higher sun-blocking lotion.
|
| Swelling, redness, or pain at the
needle site where chemotherapy drugs are given |
Certain drugs given intravenously can cause burns and sores
on your child's skin if they leak out of the vein. Tell your doctor or nurse
right away if leaking occurs.
|
|
KIDNEY AND BLADDER PROBLEMS
| Side Effect |
What You Can Do |
|
| Bladder irritation and infection |
-
Give your child plenty of fluids, especially on the day of treatment and on
days before and after treatment. The amount of fluids depends on your child's
size, so discuss this with your child's doctor.
-
Avoid giving drinks with caffeine.
-
Report to the doctor if your child has pain or burning when urinating, frequent
urination, a feeling of having to urinate right away, reddish or bloody urine,
or if he or she is not able to urinate.
|
| Change in urine color and strong
urine odor |
Some drugs cause the urine to turn orange, red, or bright
yellow and to have a strong odor. Ask the doctor if a change in urine color is
likely.
|
|
NERVE PROBLEMS
| Side Effect |
What You Can Do |
|
| Damage to nerves |
Certain chemotherapy can damage nerves, causing difficulties
with walking and talking or jaw pain. Call the doctor if any of these problems
occurs.
|
|
BONE PROBLEMS
| Side Effect |
What You Can Do |
|
| Stress fractures |
Some chemotherapy can weaken bones and cause stress
fractures. Notify the doctor if your child develops pain in the arms or legs or
if your child develops a limp.
|
|
SYSTEMIC PROBLEMS (involving the entire body)
| Side Effect |
What You Can Do |
|
| Fever |
Call the doctor if your child's temperature goes over
100.4°F or 38°C. Do not give your child any over-the-counter
medications to reduce the fever unless told to do so by the doctor.
|
| Flu-like symptoms |
Call the doctor. Symptoms may occur a few hours to a few days
after chemotherapy. They include muscle aches, headache, tiredness, slight
fever, chills, and poor appetite. These symptoms also may be from either an
infection or the cancer.
|
| Infection |
Many anticancer drugs lower the number of white blood cells,
making it harder for the body to fight infection. Here is what you can do:
-
When possible, avoid taking your child into crowds. Also, avoid being around
people with colds, flu, or any other contagious diseases, or anyone who has had
a recent immunization with a vaccine containing live viruses (regular measles;
German measles, or rubella; mumps; polio; and chickenpox).
-
Call the doctor if your child is exposed to known infectious illnesses (for
example, measles or chickenpox).
-
If the white blood count falls too low, the doctor may postpone the next
treatment or give a lower dose of drugs for a while.
|
| Anemia/fatigue |
Chemotherapy can lower the bone marrow's ability to make
red blood cells, causing anemia. Here is what you can do:
-
Look for weakness, tiredness, dizziness, chills, or shortness of breath.
-
Call the doctor if your child develops any of these symptoms.
|
| Blood clotting problems (bleeding) |
Chemotherapy can affect the body's ability to make
platelets, the blood cells that help the blood to clot. Without enough
platelets, your child may bleed or bruise more easily than usual; a blood
transfusion may be needed. Here is what you can do:
-
Look for bruises, small red or purple spots under the skin, bleeding from the
gums or nose, reddish or pinkish urine, or black or bloody bowel movements.
-
Call the doctor if your child develops any of these symptoms.
|
| Swelling/fluid retention |
-
Call the doctor if you notice swelling or puffiness in your child's face,
hands, feet, or abdomen.
-
Your child's doctor may recommend limiting table salt and salty foods and/or
order medicine to get rid of the extra fluid.
|
| Allergic reaction |
-
Look for fever, fainting, rash, difficulty breathing.
-
Call the doctor immediately. This side effect can be serious, but it is not
common.
|
|
Long-term Side Effects of Chemotherapy
Ask your child's doctor and treatment team about health problems that may occur
later as a result of the chemotherapy. A few chemotherapy drugs can cause
lasting damage to the body's organs. For example, heart problems sometimes show
up years after treatment, and children who have been treated with these drugs
may need regular checkups by a cardiologist. Your child's later ability to have
children may also be affected by chemotherapy. Finally, depending on the
specific chemotherapy your child received, your child may be at risk of
developing a second cancer.
| Radiation therapy is treatment with high-energy rays to damage or
destroy cancer cells. Like surgery, radiation therapy is a local therapy. The
rays are aimed at the part of the body that has cancer, and the treatment
destroys cancer cells in the treated area. Doctors may use radiation therapy
before surgery to shrink a tumor. After surgery, radiation therapy may be used
to stop the growth of cancer cells that remain.
|
How Does Radiation Therapy Work?
All human body cells, including cancer cells, contain a substance called DNA.
DNA tells the cells how to form and grow. In radiation therapy, the radiation
harms the DNA inside the cancer cells, causing them to die before more cells
are made. Tumors will shrink as the cancer cells die.
Getting Ready for Radiation Therapy
Before treatment begins, a doctor who specializes in radiation therapy will
talk with you and your child about treatment. The doctor also will mark the
exact area on your child where the radiation will be given. Marking ensures
that the treatment is given in the same place each time. These marks, or small
tattoos, are not painful to receive - the skin is only pricked - and they need
to stay in place all during treatment. Although the skin may become tender
during radiation, it is important to avoid using any soaps or lotions near the
markings or the part of the body receiving the radiation without the approval
of the radiation team. Lotions are often okay if removed hours before
treatment.
Because you would be exposed to radiation, you will not be allowed to stay in
the room with your child during the treatment. Your child will not be
radioactive during or after radiation therapy, so no one need fear being close
to your child.
What Will Happen During Radiation Therapy?
Radiation therapy does not cause pain. It is much like having a regular x-ray
taken, except that your child needs to hold still longer. Because some young
children are often unable to be still, the doctor may give a young child
medicine to help him or her relax or to put him or her to sleep. The parts of
your child's body that are not being treated will be covered by special shields
made of lead to protect those body parts from the radiation.
Lessening Your Child's Fears
Some children may find the machines scary. Most radiation departments will give
you and your child a tour of the area before the first treatment, so both of
you can see what the machines look like. Younger children may be afraid of
being left alone in the room. You can tell your child that you will be right
outside. In some hospitals, you may be able to see your child receive treatment
through closed-circuit television or viewing windows; your child may feel
better just knowing that you are watching.
Side Effects of Radiation Therapy
The high doses of radiation that kill cancer cells can also hurt normal cells.
When this happens, side effects occur. With radiation therapy, the side effects
depend on the treatment dose and the part of the body being treated.
The following chart gives information on the most common side effects of
radiation therapy.
Side Effects of Radiation Therapy:
ALL RADIATION SITES
| Side Effect |
What May Help |
|
| Tiredness/fatigue |
Make sure your child gets extra sleep and rest. |
| Redness. blistering of skin |
-
Leave the irritated skin open to the air.
-
Clean your child's skin as directed.
-
Use ointments only if the doctors approve.
-
Keep your child out of the sun as much as possible.
-
Use at least an SPF 30 sun-blocking lotion.
|
| Hair loss (occurs only in the area
being treated) |
-
Your child's hair should grow back within weeks to 3 months after treatment
ends, but some areas receiving higher doses may not grow back.
-
Use a mild shampoo.
-
Cut your child's hair short.
-
Avoid hair dryers and electric curlers.
-
Protect your child's scalp from cold and sun.
-
Use a wide-tooth comb.
-
If you plan to have your child wear a wig, select it before all your child's
hair comes out.
-
If you want to cover your child's head, try different hats and scarves.
-
Ask your child's doctor for medicine
|
|
HEAD AND NECK RADIATION SITES
| Side Effect |
What You Can Do |
|
| Sore mouth |
(sprays, mouthwashes, and lozenges) for your child's mouth.
-
Give your child a sponge toothbrush or cotton swab to brush his or her teeth.
-
Have your child rinse his or her mouth every 2-3 hours and after meals using
baking soda solution or water.
-
Avoid mouthwashes that have a high alcohol content, which may irritate mouth
sores.
-
Avoid serving very cold, hot, spicy, or acidic foods.
-
Try serving soft foods.
-
Contact the doctor if your child has mouth sores, painful areas, or patches of
red or white in the mouth.
|
| Dry mouth |
-
Drink plenty of water.
-
Suck on sugar-free hard candy or ice pops, or chew sugar-free gum.
-
Rinse with a mouthwash recommended by the doctor.
-
Serve foods with sauces, gravies, and salad dressings to make them moist and
easier to swallow.
-
Drink liquids with meals.
|
|
STOMACH AND ABDOMEN RADIATION SITES
| Side Effect |
What You Can Do |
|
| Nausea and vomiting |
-
Ask your child's doctor about medicines to control nausea and vomiting and/or
sedatives to help your child sleep through the nausea.
-
Feed your child light foods 3-4 hours before treatment.
-
Encourage your child to eat small amounts of food often and slowly.
-
Avoid serving sweet, greasy, and spicy foods and foods with strong odors.
-
Serve your child cold meals, such as sandwiches, instead of hot foods.
-
Encourage your child to take liquids first, and then wait 30-60 minutes before
eating solids. Most children tolerate liquids better than solids.
-
Have your child rest after meals.
-
If your child is vomiting, do not give anything to eat or drink until it is
under control. Once the vomiting is under control, give small amounts of clear
liquids (for example, water, broth, milk-free ices, and gelatin desserts).
Begin with 1 teaspoon every 10 minutes; gradually increase the amount to 1
tablespoon every 20 minutes; and finally, try 2 tablespoonfuls every 30
minutes. When your child can keep down clear liquids, try denser liquids (for
example, strained cereal, pudding, yogurt, milkshakes, cream soups). Give small
amounts as often as your child can keep them down. Gradually work up to solid
foods.
|
| Diarrhea |
-
Contact your doctor if your child's diarrhea is severe, that is, more than
three loose stools per day.
-
Avoid giving your child apple juice.
-
Avoid giving your child fatty foods.
-
Try foods high in proteins and calories but low in fiber, such as plain or
vanilla yogurt, rice with broth, or noodles.
-
Serve your child foods and liquids high in sodium and potassium. Foods high in
potassium that do not cause diarrhea are bananas, peach and apricot juices, and
boiled or mashed potatoes.
-
Make sure your child drinks plenty of liquids.
|
|
Long-Term Side Effects of Radiation Therapy
Radiation therapy also may affect your child in the future. For example,
radiation to the brain may cause learning and coordination problems, especially
in very young children. Thus, it may be helpful to consider neuropsychological
testing following treatment. Radiation therapy may also affect your child's
growth or may cause a second cancer to form in the treated area years after
treatment. Therefore, the doctor may delay radiation therapy or, if possible,
choose another treatment, such as chemotherapy. Your child's treatment team has
no way to know exactly what, if any, long-term effects your child may have, but
they can help you know what the possible effects might be.
The immune system - the body's system for defending itself - knows when
substances that should not be there, such as bacteria and viruses, are in the
body and then attacks them. The system also knows when cells have changed, such
as when cells become cancerous, and then attacks them.
Immunotherapy, also known as
biological therapy, was developed to take advantage of the body's own ability to fight disease.
In immunotherapy, substances called
biological response modifiers (BRMs)
are given to cancer patients. BRMs are substances that are normally made by the
body to fight cancer and other diseases. Scientists can make large amounts of
BRMs to use in cancer treatment. These BRMs destroy cancer cells and change the
way the body reacts to a tumor. They may also help the body replace
noncancerous cells destroyed by chemotherapy.
Several types of BRMs are used to treat cancer. Four are discussed here:
cytokines,
interleukins,
colony-stimulating factors, and
monoclonal antibodies.
-
Cytokines are proteins formed in small amounts by all human cells to help
control the working of cells.
Interferon, one type of cytokine, helps the immune system slow the
rate of growth and division of cancer cells, causing them to become sluggish
and die. In children who have cancer, these agents have been tested against
leukemia, osteosarcoma, brain tumors, and neuroblastoma.
-
Interleukins, another type of cytokine, are made by lymphocytes. Interleukin-2,
one of the most studied interleukins, causes certain kinds of white blood cells
to grow and destroy tumors.
-
Colony-stimulating factors are proteins that cause bone marrow cells to develop
platelets, red blood cells, and white blood cells.
-
Monoclonal antibodies recognize specific
antigens, substances that the body senses do not belong or regards
as "outsiders," on the surface of cancer cells. These antibodies can be
directed against a certain cell type. They can be used to attack and damage or
destroy cancer cells. They may also be used to deliver anticancer drugs or
radiation directly to specific cancer cells. This technique is still being
developed and is used only in clinical trials.
Side Effects of Immunotherapy
Depending on the exact type of treatment, immunotherapy often causes flu-like
symptoms such as chills, fever, muscle aches, weakness, loss of appetite,
nausea, vomiting, diarrhea, and, at times, a rash. Sometimes the patient will
bleed or bruise easily. Depending on how serious these problems are,
hospitalization may be needed during treatment. These side effects usually go
away after treatment ends. Ask your child's doctor about coping with the side
effects.
Some children who have leukemia or other types of cancer may need a bone marrow
transplant (BMT) or a peripheral blood stem cell transplant (PBSCT). In these
treatments, the blood cells in the diseased or damaged bone marrow - the spongy
material that fills the inside of bones and makes blood cells - are replaced
with healthy cells (stem cells), which will grow new healthy cells.
Stem cells are immature cells that produce the three types of blood cells:
-
white blood cells, which fight infection
-
red blood cells, which carry oxygen to and remove waste products from organs
and tissues
-
platelets, which enable the blood to clot.
Most stem cells are found in the bone marrow, but some - called peripheral
blood stem cells (PBSCs) - are collected from the bloodstream. Umbilical cord
blood also contains stem cells. If your doctor proposes a stem cell transplant
for your child, the stem cells may come from a donor's bone marrow,
bloodstream, or umbilical cord blood or from your child's own bone marrow or
bloodstream.
Healthy stem cells grow in two ways:
-
They divide to form more stem cells.
-
They mature into white cells, red cells, and platelets.
When transplanted into a cancer patient, stem cells can rescue the damaged
blood-forming system.
Two circumstances create the need for a transplant. The first is when the
cancer itself has injured the bone marrow. BMT and PBSCT are commonly used in
the treatment of leukemia and lymphoma. The second circumstance is when a
treatment requires such large doses of chemotherapy or radiation therapy that
the child's bone marrow is damaged during treatment. Chemotherapy and radiation
therapy target all cells that divide rapidly. Cancer cells divide more rapidly
than most healthy cells and so are destroyed by the therapies. Bone marrow
cells, however, also divide more rapidly than other healthy cells, so
high-dosage treatment can have a damaging effect on them as well.
A BMT or PBSCT can be done in three ways: as an autologous transplant, an
allogeneic transplant, or a syngeneic transplant.
-
Autologous transplant - The child's own stem cells or PBSCs cells are
used. They can be obtained from the bone marrow or from blood, using the
apheresis procedure. Stem cells are collected while the child is in
remission. To make sure that any cancer cells that remain are
destroyed, the marrow may be treated with anticancer drugs. After the marrow or
PBSCs are collected, the child receives high-dose chemotherapy, usually over 2
to 6 days, and, frequently, total body irradiation, during which the whole body
is radiated, in one dose or in many doses over several days, to get rid of the
cancer. The collected marrow or PBSCs are then returned to the child through a
vein, as in a blood transfusion.
-
Allogeneic transplant
- The marrow or PBSCs from a sibling, parent, or someone not related to the
child are used for the transplant. The transplant material must be as closely
matched to the patient's blood cells as possible. Cord blood transplant is
allogeneic.
-
Syngeneic transplant
- The perfectly matched marrow or PBSCs from an identical twin are used for the
transplant.
Before the transplant, a catheter is usually inserted into a large vein in the
chest for transplanting the marrow or PBSCs, as well as for giving blood,
antibiotics, and other drugs and for drawing blood. The child is given high
doses of anticancer drugs and/or radiation. When the cancer cells - along with
some healthy bone marrow cells - are destroyed, the new, healthy marrow or
PBSCs can be given. The healthy marrow or PBSCs are given through the catheter
and travel through the bloodstream to the bone marrow where they start to make
red and white blood cells and platelets.
It usually takes 14 to 30 days after the transplant for the transplanted stem
cells to make enough white blood cells to fight infection and to make other
blood cells. During this time, your child will be at higher risk for
infections, anemia, and bleeding. Complete recovery of your child's immune
system can take 1 to 2 years after an autologous, allogeneic, or syngeneic
transplant. Your child may need to remain in a hospital room that is kept as
free as possible from anything that may cause an infection. Supportive care,
which includes receiving blood transfusions and antibiotics, will be given.
Supportive Care
Children having a BMT or PBSCT usually stay in the hospital for 1 to 2 months
(sometimes longer), although outpatient BMT can be done for children who have
brain tumors. Children receiving BMT or PBSCT may need
supportive care.
For more information on side effects from chemotherapy and radiation therapy,
see the charts in those sections.
Graft-Versus-Host Disease
Graft-versus-host disease (GVHD) may occur in patients who receive bone marrow
or peripheral stem cells from a donor. In GVHD, donated stem cells realize they
are in a different body, so they may attack the patient's tissues, such as the
liver, skin, or digestive tract. GVHD can be mild or very severe and can occur
any time after the transplant - even years later. The doctor may give drugs to
reduce the risk of GVHD and to treat the problem if it occurs.
Supportive Care for BMT and PBSCT
| Problem |
Supportive Care Provided |
|
| Low counts of all types of blood cells |
-
Isolation from people with infectious diseases
-
Transfusion with blood products, including platelets and red blood cells
-
Treatment with proteins that increase the number of white blood cells
|
| Infections |
-
Intravenous antibiotics
-
Isolation from other people
|
| Gastrointestinal Infections |
-
Low-bacteria diet
-
Mouth care
-
Liquid antibiotics
|
| Difficulty eating enough food |
Intravenous nutrition-giving nutrients through a vein |
|
Complementary and alternative medicine (CAM) includes a broad range of healing
philosophies, approaches, and therapies. A therapy is generally called
complementary when it is used in addition to conventional treatments; it is
often called alternative when it is used instead of conventional treatment.
(Conventional treatments are those that are widely accepted and practiced by
the mainstream medical community.)
It is important that the same scientific evaluation used to assess conventional
treatments be used to evaluate complementary and alternative therapies.
Conventional cancer treatments have generally been studied for safety and
effectiveness through clinical trials, which are research studies with people.
Some complementary and alternative therapies have not been studied in clinical
trials.
|
Questions to Ask Your Child's Health Care Provider About Complementary and
Alternative Therapies
-
What benefits can be expected from this therapy?
-
What are the risks associated with this therapy?
-
Do the known benefits outweigh the risks?
-
What side effects can be expected?
-
Will the therapy interfere with conventional treatment?
-
Is this therapy part of a clinical trial? If so, who is sponsoring the trial?
-
Will the therapy be covered by health insurance?
|
Others, which once were not accepted by the mainstream medical community, are
gaining acceptance in cancer therapy - not as cures, but as complementary
therapies that may help patients feel better and recover faster. One example is
acupuncture. Other therapies, such as laetrile, have been studied and found to
be ineffective and potentially harmful.
If you have questions about complementary or alternative therapies, discuss
them with your child's doctor or treatment team.
Being in the hospital is often scary for any child, especially at first. It is
a whole new world to learn about - new people and strange machines, procedures,
and routines. Adding a touch of home by having pictures of family members and
friends, drawings, and other personal things in your child's room can help make
the hospital a less scary place. These homey touches can help start a
conversation between the hospital staff and your child.
One of the scariest things for many children is being separated from their
parents and siblings. Many hospitals and treatment centers help your family and
your child spend as much time together as possible by allowing you to visit
anytime and having beds for parents in the child's room or bedrooms nearby. If
the hospital does not have beds for you, you might ask to sleep in a chair near
your child's bed.
Most hospitals have playrooms for children who are patients. Playrooms often
have toys, games, arts and crafts supplies, and tape players, giving children a
chance to play and talk with each other in much the same way that they do with
their friends at home or in school. The playroom setting allows children to
relax and become more comfortable in the hospital. Playroom staff, trained in
working with children who have serious illnesses, can talk to parents and other
members of the treatment team about the fears or concerns a child may share
through play.
If your child cannot get out of bed to go to the playroom, child-life workers -
trained staff who help coordinate play, schoolwork, and other activities for
the child - may make bedside visits.
For older children who are trying to separate themselves from you and be more
on their own, being in the hospital may thwart their drive for independence. At
a time when young people are normally doing more on their own, cancer makes
them rely on you more. As a result, adolescents may make it known, loudly and
often, that they are unhappy. They may refuse treatment, break hospital rules,
miss outpatient appointments, and rebel in other ways.
Children of any age will often cooperate more if given treatment choices that
do not cause problems with their care. Parents can help children become more
independent by allowing them to share the responsibility for their care. Some
hospitals also make a special effort to help children cope with illness and
being in the hospital, such as allowing teenagers to dress in street clothes
whenever possible and to have friends visit. Some hospitals have equipment that
allows the child to interact with his or her classmates in their classroom.
Common Medical Procedures
Medical tests and procedures are not only used to diagnose
cancer, but also to see how well the treatment is working and to
make sure that the treatment is causing as little damage to normal
cells as possible. Many of these tests will be repeated from time to
time throughout treatment.
Parents and children say that knowing about the tests before
they are done helps them to cope. You may want to ask your doctor
these questions before any testing is done: -
Which tests will my child have? What will my child need
to have this test? An IV? An oral contrast?
- Where and how is each test done?
- Will the tests be painful? If so, what can be done to make
my child more relaxed and in less pain?
- Who will do the tests? Has the staff doing the testing
worked with children?
- What information does the doctor expect to get from the
tests?
- How soon will the results be known? What do the results
mean?
- Will the tests be covered by insurance?

Some of these tests are painful; most are not. For some tests,
your child may need to remain still for as long as an hour. Ask
your doctor what you and the treatment team can do to help your
child become more comfortable during the tests. For procedures
that require your child to remain very still, medicines can be given
to help your child relax or become sleepy. For tests that can be painful, such as the bone marrow aspiration test and spinal tap,
pain medicines are often given. Sometimes a general anesthetic, a
drug that causes your child to lose consciousness and all feeling, is
given.
Relaxation therapy (methods used to make one feel more
relaxed and to feel less pain),
guided imagery (using the imagination
to create mental pictures),
hypnosis (a trance-like state that
can be brought on by a person trained in a special technique),
music, and other techniques can also help to ease your child's discomfort
and fear. When your child is relaxed, the procedures are
less painful. Ask your treatment team to help you guide your child
through relaxation exercises both before and during the procedures.
Often a combination of pain medicine and relaxation techniques
is used.
Your child will want to be with you during the procedures, and
in most situations, that is possible. See Common Health Issues 9. The following chart provides
information about some common medical procedures your child
may have.
Biopsy
| Procedure/Test | Purpose | What is Done |
|
| General |
A biopsy determines if a
tumor is not cancerous
(benign) or cancerous
(malignant). If the
biopsy is "positive,"
cancer is present. If it is
"negative," cancer cells
were not seen. |
A doctor removes part or all of the tumor or part of the bone marrow. A pathologist, a doctor who specializes in recognizing changes caused by disease in humans, looks at the tissue under a microscope. |
| Bone marrow aspiration or bone marrow biopsy |
This type of biopsy
examines the bone
marrow under a microscope
to see if leukemia
is present or if the treatment
is working. For
other cancers, this test
tells whether the disease
has spread to the
bone marrow.
|
For young people, a bone marrow test is most often done in the hip bone. The child lies on his or her stomach with a pillow under the hips. A needle is put through the skin and into the middle of the hipbone, and a small sample of marrow is quickly drawn into the syringe. The most painful part of the test lasts for a few seconds. |
|
Blood Studies
| Procedure/Test | Purpose | What is Done |
|
| Tumor markers |
This type of test searches for substances that may increase in the blood of a person with cancer. It can help to diagnose cancer and to find out how well the child is responding to treatment. |
A sample of blood is usually obtained through a needle inserted in a vein or by pricking the tip of the finger and sqeezing out a few drops of blood. Sometimes blood is obtained via tubes (catheters) that have been surgically placed through the chest and into one of the major blood vessels leading to the heart. |
| Complete Blood Count (CBC) |
A CBC test checks the white blood cells, hemoglobin, hematocrit, and platelet count in a sample blood. |
See above. |
| White blood cell (WBC) count |
A WBC count measures the number of WBCs in the blood and is also used to find certain types of immature cells - called blast cells - typical of leukemia. WBCs protect the body from infection. Chemotherapy and other treatments can lower the number of WBCs, increasing the risk of infection. If the test reveals a low WBC count, treatment may need to be delayed until the count goes up. |
See above. |
| Hemoglobin |
Hemoglobin is the substance in red blood cells that carries oxygen to the body's tissues. Low hemoglobin indicates anemia. Anemia can cause your child to look pale and feel weak and tired. It may be a side effect of chemotherapy or a sign that the cancer has returned. |
See above. |
| Hematocrit |
Hematocrit determines the size, function, and number of red blood cells. A low hematocrit also may mean that anemia is present. |
See above. |
| Neutrophils (also called ANC-absolute neutrophil count) |
This blood study tests for the body's ability to fight bacterial infections. |
See above. |
| Platelet count |
This test measures the number of platelets. Platelets help the blood clot. A low platelet count, which may be due to side effects of medicine or to infection, or may mean that leukemia is present, could cause one to bleed or bruise easily. |
See above. |
|
Lumbar Puncture
| Procedure/Test | Purpose | What is Done |
|
| Lumbar puncture or spinal tap |
This test obtains a sample of spinal fluid - the liquid that surrounds the brain and spinal cord. The doctor looks at the fluid under the microscope to see if any infection or cancer cells are present. It is also used to give anticancer drugs directly to the brain and spinal cord. |
The child, in a curled position, lies on one side or sits. A needle is inserted between the small bones of the spine into the fluid space around the spinal cord. A sample of the spinal fluid is taken. This test can be somewhat painful. |
|
Imaging Tests
| Procedure/Test | Purpose | What is Done |
|
General |
Imaging tests take pictures of images of areas inside the body to see what is happening. |
Tests are generally not painful, but the equipment may be frightening to children. Some machines, such as MRIs, make very loud noises. |
| Angiograms |
An angiogram obtains an x-ray of the blood vessels and shows changes in the blood vessels and in nearby organs. Clogged blood vessels or blood vessels that have moved may mean that a tumor is present. |
A special dye is injected into an artery and travels through the blood vessles. Then a series of x-rays is taken. The dye makes the blood vessels show up on an x-ray. |
| Ultrasound |
Ultrasound obtains a picture of part of the body by using sound waves. The waves echo or bounce off tissues and organs, making pictures called sonograms. Tumors have different echoes than normal tissues, making it possible to "see" abnormal growths. |
A small hand-held device called a transducer is used to send the sound waves to a site in the body. The transducer is rubbed firmly back and forth over the site after the skin has been lubricated with a special gel. |
| Radioisotope scanning |
This test studies the liver, brain, bones, kidneys, and other organs of the body. |
The child either swallows or has an injection of a mild, radioactive material that is not harmful. After a short wait, a scanning device is passed over the body to detect where the radioactive material collects in the body and allows the doctor to locate tumors. Your child will not be radioactive during or after these tests. |
| CT scan (computerized tomography scan) or CAT scan |
This test obtains a three-dimensional picture of organs and tissues; ordinary x-rays give a two-dimensional view. Using pencil-like x-ray beams to scan parts of the body, a CT also gives better pictures of soft tissues than does an x-ray. It provides precise and very useful details about the location, size, and type of tumor. |
While the child lies still, a large machine moves back and forth, taking pictures.
The scan takes 30-90 minutes. Sometimes a special dye is injected into a vein before the scan.
If your child has a central venous line in the chest, it generally cannot be used during a CT scan of the chest.
It is important to prepare your child for an IV in the hand. |
| MRI (magnetic resonance imaging) |
An MRI creates pictures of areas inside the body that cannot be seen using other imaging methods. MRI uses a strong magnet linked to a computer. Because an MRI can see through the bone, it can provide clearer pictures of tumors located near the bone. |
The child lies on a flat surface, which is pushed into a long, round chamber. Your child will hear a loud thumping noise, followed by other rhythmic beats. The test takes 15-90 minutes, during which your child must lie still.
Sometimes a special dye is injected into a vein before the test. |
|
 |
Common Health Issues
Pain relief, nutrition, treatment for infections, immunizations, bleeding,
transfusions, and dental/mouth care are all part of supportive care. The goal
of supportive care is to prevent or lessen the side effects of the treatment
and the disease. With this care, your child can receive the needed therapy with
greater safety and comfort. You may want to talk with your child's doctor or
other members of the treatment team to see how the information provided below
might help your child.
Your child may have pain for a variety of reasons. Pain may be caused by the
cancer itself, or it could be from the treatment, such as surgery to remove a
tumor or side effects of chemotherapy. Sometimes, cancer patients have pain
that has nothing to do with the cancer, such as a toothache or a headache.
-
Not all children with cancer have pain. Those who do are not in pain all of the
time.
-
Medicine and other treatments can almost always relieve cancer pain.
-
Relieving pain will not only make your child more comfortable, but also may
help your child sleep and eat better.
-
Parents often feel helpless when their children are in pain. This reaction is
natural. Knowing what to expect and what can be done to relieve pain can help.
Talk with the doctor and treatment team about whether your child is likely to
have pain, what pain treatment your child can receive, or what to do for your
child if pain occurs.
|
How Is Pain Managed?
The best way to relieve pain is to treat its cause. If a tumor is causing pain,
the doctor may try to remove the tumor or decrease its size using surgery,
radiation therapy, and/or chemotherapy. Other ways to relieve or control pain
include use of:
Preventing pain from starting or getting worse is the best way to control it.
Some people call this "staying on top of the pain." It may also mean that your
child will need a lower dose of a pain reliever than if you wait until the pain
gets bad. Different pain medicines take different lengths of time to work, from
a few minutes to several hours. If your child waits too long to take pain
medicine, the pain may get worse before the medicine helps.
To treat your child's pain, the doctor may start with medicines such as
acetaminophen. If the pain increases, stronger drugs that require a
prescription may be needed. Sometimes,
opioids
are prescribed. Narcotics are the strongest pain relievers available. Studies
show that taking narcotics to relieve cancer pain will not make your child
addicted to drugs. When your child is taking opioids, talk to the doctor,
nurse, or pharmacist before giving him or her any other medications.
Work closely with the treatment team in sharing information about your child.
For example, if you know that your child is afraid of needles, ask the doctor
if your child can be given oral medicine. In older children and adolescents,
the doctor may order a self-controlled drug "pump." This method uses a portable
computerized pump containing pain medicine attached to a needle that is placed
in a vein or attached to the central vein catheter. When pain relief is needed,
the child presses a hand-held button, and the pump injects a preset dose of
medicine into the vein. Pumps are programmed to give preset doses only at
preset intervals, so even if the child presses button more than once during the
preset interval, he or she will not get any more pain medication than is
programmed.
How Will I Know How Bad My Child's Pain Is?
Treating pain in children requires a special understanding of the child and of
the child's age. In some cases, you may need to speak for your child,
especially if your child is younger than 4 years old. For infants and very
young children, you can be of great help by closely watching the expressions on
your child's face and carefully listening to the way your child cries. Take
note of changes in behavior, such as sadness or isolation or decreased
activity. The changes may mean that your child is in pain.
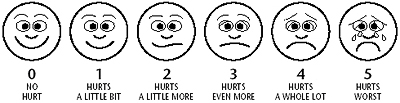
From Wong, D.L., Hockenberry-Eaton, M., Wilson, D., Winkelstein, M.L., Ahmann,
E., DiVito-Thomas, P.A.: Whaley and Wong's Nursing Care of Infants and
Children, ed. 6, St. Louis, 1999, p. 2040. Copyrighted by Mosby, Inc. Reprinted
by permission. |
Sometimes, children have pain, but they may not be able to tell you about it.
They may be afraid to. It is important to ask if your child has pain. Talk with
your child about where and how much pain there is. Use words that your child
knows, such as "boo-boo" or "ouch." A good way to determine the amount of pain
your child has is to use a pain scale. A frequently used pain scale is the
Wong- Baker FACES Pain Rating Scale, which can be used with children as young
as 3 years old. On this scale, each face demonstrates a level of pain, from a
person who feels happy because there is no pain (hurt) or sad because there is
some or a lot of pain. Face 0 is very happy because there is no hurt. Face 1
hurts just a little bit. Face 2 hurts a little more. Face 3 hurts even more.
Face 4 hurts a whole lot, but Face 5 hurts as much as you can imagine, although
you do not have to be crying to feel this bad. Ask your child to choose the
face that best describes the pain. Report the number under the chosen face to
your child's nurse and doctor.
What If the Pain Is Not Being Controlled?
Cancer pain almost always can be greatly lessened or relieved, but no doctor
can know everything about all medical problems. If your child's doctor is
unable to control your child's pain, ask to see a pain specialist. Pain
specialists may be oncologists, anesthesiologists, neurosurgeons, other
doctors, nurses, or pharmacists. A pain control team may also include
psychologists and social workers.
For more information about pain control, you and your child's treatment team
may find these NCI booklets helpful:
Many side effects from cancer treatment may make it hard for your child to eat.
Some physical side effects include loss of appetite, sore mouth, changed sense
of taste, nausea, vomiting, diarrhea, constipation, and weight gain. The
emotional side of cancer treatment may also affect your child's eating habits.
When children are upset, worried, or afraid, they may have eating problems.
Losing his or her appetite and feeling nauseated can be normal when your child
is nervous or afraid. The treatment team, including the nutritionist/dietitian
at the hospital where your child receives treatment, can help you plan the food
to serve at home. Let the team know if you notice that your child is losing or
gaining weight. Ask what has worked for other children. The good news is that
even children who have trouble eating have days when eating is a pleasure. The
following suggestions may help your child feel more like eating:
Serve appealing food.
-
Build meals around your child's favorite foods, but do not force favorite foods
during nausea attacks. Forcing may cause a lasting dislike of the food.
-
Try always to give high-calorie foods (for example, macaroni and cheese with
real butter and cheese, or milkshakes made with ice cream). Add instant
breakfast powders to all milk and milk products.
Adopt a casual attitude about mealtimes.
-
Let your child eat whenever he or she is hungry or offer food often during the
day. Have high-calorie, high-protein snacks handy. Taking just a few bites of
the right foods or sips of the right liquids every hour or so can help increase
your child's intake of proteins and calories. You can freeze portions of a
favorite dish and serve them when your child wants them.
-
Oral medicines may affect your child's appetite. Some are best given in the
morning, some at midday, and some on a full stomach. Ask the doctor when and
how medicines should be given. Tell the doctor if your child has no appetite or
has any other side effects.
-
Try changing the time, place, and surroundings of meals. A picnic, even if it
is in the house, can make mealtime more fun. Watching a favorite TV show or
inviting a special friend to join your child at meal or snack time also can
help your child feel more like eating.
Create a pleasant setting.
-
Make mealtimes calm and relaxed. Do not hurry meals.
-
Praise good eating. Try using small rewards, such as a favorite dessert or a
new toy, to encourage good eating. Siblings should be considered when setting
up a reward system. It is important that siblings are not left out, but be
careful not to encourage healthy siblings to overeat.
-
Avoid arguing, nagging, or punishing. Forcing a child to eat may make things
worse.
If your child's eating becomes a serious problem, ask your child's doctor about
medicines that can improve appetite.
Sometimes children gain extra weight during treatment because of the buildup of
excess water in the body. Do not put your child on a diet. Instead, call the
doctor. If the weight gain is due to extra water, the doctor may recommend
using less salt, because salt causes the body to hold onto water. The doctor
may also order medicines called diuretics to get rid of the excess water.
Children who have cancer need diets high in both calories and protein.
High-calorie foods help prevent weight loss, and protein foods help the body
stay strong and repair itself. To get your child to eat more protein and
calories, try these tips.
-
Offer liquids during the day, but not at mealtimes. Liquids are filling and
take away an appetite for solid foods. Give your child a straw to make drinking
easier.
-
Some types of chemotherapy may change your child's sense of taste for a while.
Well-seasoned foods, such as spaghetti, tacos, and pizza, may seem good at such
times. Sometimes, adding extra salt or sugar, or using less, may make foods
taste better.
-
Avoid empty-calorie foods, such as soft drinks, chips, and candy, that can make
your child's appetite worse without providing good nutrition. Milkshakes,
yogurt, fruit, juices, or "instant breakfasts" provide extra calories and
protein.
You will also find many helpful suggestions in NCI's booklet
Eating Hints for Cancer Patients 13, available from the CIS at 1-800-
4-CANCER (1-800-422-6237) or TTY at 1-800-332-8615. It is also available
online 11.
Infections are common in children who have cancer, especially in children who
are receiving chemotherapy. Chemotherapy lowers the white blood cell count,
which increases the chances of infection. You should report any sign of
infection, such as a fever, to your child's doctor right away.

Infections are usually caused by bacteria or viruses. To find the cause of your
child's infection, the doctor may take samples (cultures) of the throat, blood,
urine, or stool. If the infection is from bacteria, your child will receive
antibiotics. Antibiotics will not work against viruses. Unless a virus has been
identified, however, most children are treated with antibiotics until their
blood counts improve, even if bacterial infection cultures are negative. Your
child may receive other medicines to help ease the symptoms. If the infection
is serious, or the white blood cell count is very low, your child may need to
be treated at the hospital. Your child's doctor may also stop the cancer
treatment for a short time until the infection is gone.
Some viral infections, such as chickenpox, can cause major problems for a child
receiving chemotherapy. Call the doctor right away if your child is exposed to
chickenpox or to anyone who has recently received the chickenpox vaccine. And
ask your child's teachers to let you know if a schoolmate develops chickenpox.
Some families ask teachers to ask schoolmates' families to call them at once if
chickenpox develops in their families.
Once children have had chickenpox, they usually do not get it again, but some
children on chemotherapy who have already had chickenpox may develop shingles.
Shingles is a blister-like skin rash that looks like chickenpox. Instead of
appearing all over the body, however, shingles is in just one area. Call the
doctor right away if you think that your child may have shingles.
Regular or red measles (also known as rubeola or 9-day measles) may also be
more serious for a child on chemotherapy. If your child comes into contact with
this type of measles, you should call the doctor. The doctor may give your
child medicine to prevent or control the infection.
Most vaccines, and especially live virus vaccines (regular measles, German
measles or rubella, mumps, polio, and chickenpox), should not be given to a
child receiving cancer treatment, although some doctors do recommend varicella
(chickenpox) vaccines for children with cancer and for their siblings. Some
immunizations may be dangerous because chemotherapy cancer treatment lowers the
body's ability to protect itself when given these vaccines. In addition,
brothers or sisters should not receive the live polio vaccines while their
sibling is having cancer treatment. You should discuss these matters in detail
with both your child's oncologist and your children's primary care provider
(for example, pediatrician, clinic, or family physician).
Vaccines that are not live may be safe to give during cancer treatment,
including diphtheria, whooping cough, and tetanus immunizations (DPT, DT, or
IPV shots). Flu shots are okay, but you should ask your child's doctor before
any immunizations are given.
Platelets are blood cells that help the blood to clot. A low platelet count may
cause your child to bleed more easily than usual. If your child's platelet
count is low, he or she will need to avoid contact activities such as football,
soccer, or skateboarding. If bleeding occurs, you may try the following:
-
Apply pressure until the bleeding stops - a clean towel, handkerchief, or cloth
firmly pressed to the wound will slow or stop the bleeding.
-
For nosebleeds, have your child sit up; do not let your child lie down. Pinch
the bridge of the nose over the bone for 5 minutes. The pressure must be tight
on both sides to stop the bleeding.
If bleeding continues, call the doctor immediately.
Children who have cancer may need to receive whole blood or blood components
(such as red blood cells). This procedure is called a transfusion. Packed red
cells are often given to control anemia - a condition in which the blood
becomes low in red blood cells or in hemoglobin. A platelet transfusion is
given if the platelet count is low. White cell transfusions are not routinely
given when white blood cell count is low. The doctor may, however, consider
white cell transfusions when a child with a very low white cell count has a
very serious infection that is not responding to antibiotics.
Each person has a certain type of blood. Each person can only receive the blood
of the same type or from the universal donor type "O."
If possible, your child should have a complete oral exam and any needed dental
work before cancer treatment begins. Dental care is important during treatment,
but even checkups should be avoided when blood counts are low. Always check
with the doctor before starting any dental work, and let the dentist know your
child is receiving cancer treatment. Your child may need to take an antibiotic
before any dental work is done to prevent possible infections. In general, a
low dose of amoxicillin is given before even a routine cleaning to patients who
have a central venous catheter.
Keeping the child's teeth, mouth, and gums clean to protect against decay is
especially important. Make sure your child's teeth are brushed after each meal,
using a soft toothbrush. After each use, rinse the brush well with cold water,
shake it well, and allow it to dry. Give your child paper cups to rinse his or
her mouth. Dental floss may be used if care is taken not to cut or irritate the
gums.
Mouth Care During Radiation Therapy
During radiation to the head and neck, less saliva is produced, so the mouth
becomes dry. This dryness can lead to tooth decay. The doctor or dentist may
recommend using a fluoride mouth rinse or order a fluoride gel. Check with your
doctor before buying a mouthwash - many can cause burning pain in a child with
a sore mouth. All children receiving radiation should rinse their mouths often
during the day. One suggested mouth rinse is a mixture of salt and baking soda
(1/2 teaspoon of each in a cup of water). To care for infants and toddlers,
wrap a soft cloth around your finger and gently wipe the teeth and gums with
the mouth rinse. Soft "toothettes" can also be used to apply the rinse to the
child's mouth.
Mouth Care When Blood Counts Are Low
When your child's blood counts are low, mouth care needs to be especially
gentle; your child can get an infection or start bleeding more easily. Use very
soft bristle toothbrushes, cotton or glycerin swabs, or toothettes, and avoid
using water jet devices or dental floss. Call the doctor if you see any red or
white patches, mouth sores, or irritated areas in the mouth.
Mouth Care When Your Child Has Mouth Sores
When mouth sores, bleeding areas, or irritated areas occur, use only the mouth
rinse described above or one the doctor recommends. Your child should rinse the
mouth out well after every meal and before bedtime. Cotton or glycerin swabs or
toothettes (available in drug stores) can help remove pieces of food from the
mouth. If mouth sores become painful, a local anesthetic may help. The doctor
can order an anesthetic and will tell you how often to use it. To make eating
easier, put the anesthetic on the sore gums before meals. For dry lips, try a
lanolin lip ointment to prevent them from cracking and becoming sore.
When to Call the Doctor
If you have worried about knowing when to call the doctor, you are not alone.
Parents want to watch closely for any sign that their child may need to see the
doctor but may not be sure what those signs are. They also may worry about
"bothering" the doctor or treatment team. The best approach is to ask the
doctor when to call about any problems your child may be having. If you are
unsure, this list can be used as a guide for when to call the doctor.
Your child shows signs of infection.
-
Fever (100.4°F or 38°C) or other sign of infection, especially if your
child's white count is low. (The doctor will tell you when it is low.) It is
important to take your child's temperature with an accurate thermometer.
Your child has trouble eating.
-
Mouth sores that keep your child from eating
-
Difficulty chewing
Your child has digestive tract problems.
-
Vomiting, unless you have been told that your child may vomit after the cancer
treatment
-
Painful urination or bowel movements
-
Constipation that lasts more than 2 days
-
Diarrhea
Your child shows changes in mobility or mood.
-
Trouble walking or bending
-
Trouble talking
-
Dizziness
-
Blurred or double vision
-
Depression or a sudden change in behavior
Your child has troublesome symptoms.
-
Bleeding, including nosebleeds, red or black bowel movements, pink, red, or
brown urine, or many bruises
-
Severe or continuing headaches
-
Pain anywhere in the body
-
Red or swollen areas
Your child needs treatment for other health concerns.
-
Before your child receives immunizations or dental care, even scheduled
vaccinations or regular dental checkups
-
Before you give your child any over-the-counter medication
You are in any doubt whatsoever?
You can find more information about these topics in this booklet under
Common Health Issues 14.
Moving on With Life

One of the challenges facing the family of a child who has cancer is going on
with everyday life. Moving forward is not an easy task. It may be hardest
during times of stress: when you find out your child has cancer, when your
child is in the hospital, or when your child is suffering from the side effects
of treatment.
Even when the treatments are going well, the cancer still affects each member
of your family. When your child enters the hospital or goes for treatments,
each member has to adjust in some way. Family members may be apart. Days of
work may be missed. Brothers and sisters may feel left out. Everyone may be
worried and tense.
Despite all this, family life goes on. Brothers and sisters have school and
activities. Parents have jobs. It is hard to keep up with everyday activities
and responsibilities while being with and caring for your child with cancer.
As the mother or father of a child who has cancer, remember that you are not
alone. You can get help from many sources, such as the treatment team, which
includes a social worker who can help you in dealing with your child's illness;
other parents of children with cancer; support groups; or others. (You can find
more information in
resources 15) The information below may also be helpful for you, your
child, the other children in your family, your extended family, and friends.
Your Child
Even with a diagnosis of cancer, your child still has the same needs as other
young people - going to school, having friends, and enjoying things that were a
part of life before cancer. You can help meet these needs by letting your child
live as normal a life as possible. Some activities, however, may need to be
changed at different times during treatment. After chemotherapy or radiation
therapy, your child may be very tired and, therefore, need more rest. This
tiredness is to be expected. Help your child find other things to do, such as
new hobbies, or ask friends to come over to draw or paint.
School and Friends
Encourage your child to stay in touch with friends. Keeping contact is easier
if your child can continue to go to school while being diagnosed and treated,
but staying in school is not always possible. If time off from school is
needed, it is best for your child to return to school as soon as possible.
Children who have cancer need and like to be with others their age, and keeping
up with schoolwork makes them feel good about themselves. Some cancer centers
offer back-to-school programs, which may help children and classmates
understand the diagnosis and know what to expect. You may ask your doctor,
nurse, or child-life specialist to visit your child's classroom.
Children often worry about how their friends and classmates will act toward
them, especially if they have missed a lot of school or return with obvious
physical changes, such as hair loss or a missing limb. Other students are
usually accepting, but they may have questions. Help your child to think of
ways to answer their questions and to tell friends and classmates that they
cannot "catch" the disease. Your treatment team has had experience helping
families with school. Ask them to help your child. Ask your nurse if the team
or hospital has a school reentry program. Such programs send nurses to the
child's classroom to talk about the child's cancer and treatment with
classmates and teachers.
Your child needs to know that many people, including children, are uneasy about
a serious illness. These people may act differently or say hurtful or wrong
things to someone who has cancer.
You may want to talk with your child's teachers and school nurse about the
disease, treatment, days missed, and any needed changes in activity. You and
your family, the doctor, or members of the treatment team can explain your
child's medical condition and answer questions. Teachers and other school staff
may want to use this information to talk with the other students about what to
expect when your child returns to school.
If your child cannot return to school right away, a home tutor may be available
through the school system to help your child keep up with studies, making it
easier to return to school.
|
To help your child and his or her siblings deal with fears and feelings, you
may want to:
-
Say "I love you" often.
-
Assure your children that the cancer and its treatment are not punishments.
-
Encourage your child or children to talk about the cancer and cancer treatment.
Ask your children questions to get the conversation started. Family talks can
help everyone feel less worried. Talking helps the whole family cope with the
illness together.
-
Tell your children that is it okay to feel sad and cry.
-
Encourage activities to help your child feel more relaxed. Drawing, playing
with harmless medical supplies or puppets, and role-playing may help your child
feel better.
In addition, setting limits for behavior and activities is still important and
even comforting to your child. But it is helpful to remember that children,
like adults, have good days and bad days. Help your child feel part of normal
life.
-
Allow your child to make choices as long as they do not cause problems with
treatment.
-
Use the same rules and level of discipline as before the cancer diagnosis and
treatment.
-
Ask your child to continue doing regular chores around the house, when able.
|
Supporting Your Child
Like you, your child is likely to feel uncertain, worried, and afraid at times,
but he or she may find it hard to talk about these fears and may behave
differently than usual. For example, your child may become loud or bossy, be
quieter than usual, have nightmares, have changes in eating habits, not do as
well in school, or go back to earlier behaviors such as bedwetting or
thumb-sucking.
These common behavior changes are just a few of the ones you may see. You may
want to talk about such changes with the doctor, nurse, social worker,
teachers, and school counselor, who have had experiences like yours.
Teenagers who have cancer have special concerns. They frequently complain that
their parents try to protect them too much. Teenagers are at a stage in their
lives when they are naturally trying to be their own bosses and do things for
themselves, but having cancer forces them to depend on you. Giving teenagers a
chance to make their own decisions and choices, when possible, will help.
You
Your child's illness will bring many changes to your life. To help you cope
with these changes, you may want to consider the following suggestions:
-
Make time for yourself.
Try to do some of the things you did before your child got sick. Do not feel
guilty that you need some time for yourself. Also, make a special effort to
find private times to talk with your partner or those who are close to you. Do
not let all your talk be about your child with cancer.
-
Prepare yourself for a lot of waiting.
Find ways to make waiting during clinic visits or while in the hospital less
frustrating. Take something to read or do while your child is asleep or does
not need your attention.
-
Turn to treatment staff or other resources for support.
Treatment centers have trained staff who can talk with you about your concerns.
Make use of these people for support.
-
Contact support groups.
Your treatment center can provide names of support groups at which you can meet
with other parents of children who have cancer. Community resources can provide
support and information. They can tell you how other parents have dealt, or are
dealing, with the same types of situations you are facing.
-
Share the care of your child with your partner or others close to the family.
For example, if your child is in the hospital for a long stay, you and your
partner, or friends or relatives, may want to take turns staying with your
child. Letting them help will not only give each of you a break from the
hospital, but it will help keep you from growing apart when one becomes more
involved than the other in your child's treatment.
Brothers and Sisters
The lives of children who have a brother or sister who has cancer change a
great deal. Siblings may have many different feelings about the brother or
sister who has cancer and the extra attention the child receives. They may feel
sorry for their sibling who is ill. Younger children may feel that they caused
the cancer. Or they may believe that their own needs are being ignored.
When a child is in the hospital and is very ill, the focus is on that child. As
a parent, you may not be able to pay as much attention to your other children
as you did before. You may have to miss many of their special school or sports
events. You may also use up all your energy and patience caring for your child
who has cancer and not have enough energy or time to talk with your other
children, play with them, or help them with their homework. It is natural,
then, for siblings to be annoyed at the attention your child who has cancer is
receiving.
As a result, siblings' behavior may change. They may become depressed, have
headaches, or begin to have problems in school. School counselors and support
groups may be able to offer you helpful advice for dealing with these issues.
In addition, here are some things you can do to help your other children:
-
Talk with them about their feelings.
Talk with them about the special attention your child who has cancer is
getting. Let them know that feeling mad is natural. Try to explain what is
happening and why you may not be around as much as you were before.
-
Talk with them about the cancer, the treatment, and care.
Younger children's fears can be helped by knowing they couldn't have caused the
illness by wishing or by spreading germs from a cold. Treatment and procedures
should be explained as being helpful things and not punishments.
-
Spend time with your other children.
Try to spend some time with them doing the things they like.
-
Encourage them to take part in outside activities.
Make a point of noticing and praising what they do in these activities.
-
Involve them in their brother's or sister's treatment.
Let them come along with you to the clinic or hospital. Having them along will
allow them to see for themselves what the hospital, clinic, and treatment are
like.
-
Talk with them about questions their schoolmates and friends may ask.
Help them think of possible questions and answers so that they will feel
comfortable talking about their brother's or sister's illness.
-
Ask other family members and friends to spend time with the other children in
the family.
For example, an aunt or uncle might go to school events or attend important
games or performances. A neighbor might help them with homework or take them on
outings.

Family and Friends
A diagnosis of cancer affects not only the child, parents, and siblings, but
also grandparents, other relatives, and friends. These people can support and
assist you during this time.
Your employers also may need to be told about your child's illness, so they
will know why you are asking for extra time off from work. If needed, your
child's doctor can write your employer to explain the situation.
You may need to tell people how to help you. Here are some ideas on how to tell
them:
-
Be open and honest.
-
Take the lead to show others how you and your child want to be treated.
-
If they are giving you too much attention, point it out.
-
You may find it tiring to have to repeat details about your child's illness to
many family members and friends. Ask one person to handle calls and questions.
Or, you can leave short messages on a home answering machine.
-
It can be helpful to ask one friend or family member to be the "point person"
to share with people your needs - for example, getting the wash done or
shopping for groceries.
If you are like most parents of children who have cancer, you will be worried
about the costs of treatment and continuing care. You want the best care but
are afraid of the costs and how they will be met. You may not have health
insurance. Or insurance may not cover all costs. Some insurers will not cover
certain costs when a new treatment is under study.
You will need to understand the coverage that your policies offer. Here are
some tips for making the most of your insurance:
-
Get copies of your insurance policies and find out exactly what is covered.
-
Get help if you need it to understand the policy or how to file claims if you
need to. Do not be afraid to ask friends, family members, or a social worker
for help. Private companies and some community organizations also offer help to
deal with insurance.
-
Keep careful records of all expenses and claims. Store bills and insurance
forms together to make it easier at tax time.
-
File claims for all covered costs. Sometimes, people do not take full advantage
of their insurance, either because they do not know about a benefit or are put
off by the paperwork.
-
If your claim is turned down, file again. Ask your doctor to explain to the
company why the services should be covered under your policy. If you are turned
down again, find out if the company has an appeals process.
What Does the Future Hold?
Because of better research and treatment, children who have cancer are living
longer than they used to, and their quality of life is better. Although they
lead normal lives, survivors of cancer have some concerns that other people may
not have. For example, they must take extra-special care of their health and
may have problems obtaining insurance.
Regular exams are very important after treatment for cancer. At these visits,
your child receives both the health care needed by anyone your child's age and
special care based on the type of cancer and treatments and current health.
In general, parents of children who have had cancer treatment should do the
following.
-
Schedule regular checkups.
Children who have been treated for cancer usually return to the doctor every 3
to 4 months at first, and once or twice a year later on. Ask the doctor how
often your child needs to return for followup exams.
-
Be alert to signs of the possible return of cancer.
Doctors have no way to tell for sure whether your child's cancer will return.
If it does return, it could be weeks, months, or years after treatment ends.
Talk with your child's doctor and treatment team about the chances of cancer
returning and the signs of cancer's return.
-
Be alert to signs of lasting effects of cancer treatment.
Cancer treatment may cause side effects many years later. Some cancer
treatments may affect your child's ability to have children in the future;
affect how your child learns and grows physically; or increase your child's
risk of developing a second type of cancer.
-
Be tuned in to any problems your child may have in dealing with feelings about
having had cancer, even years after treatment has ended.
Once all the activity of treatment is over, some children suddenly fully
realize what happened to them. It can be a very upsetting. At this point, they
may need to talk about their feelings and may even need to see a counselor.
-
Promote good health habits.
Eating well and getting enough sleep and exercise will help your child feel
better and be healthy.
To better understand your child's health care needs today and in the future,
ask the doctor and treatment team.
You need information to continue to take care of your child's health. As your
child gets older, he or she also will need this information. You may want to
ask the doctor and treatment team the following questions:
-
How often should my child have checkups?
-
What are the signs of cancer's return or of long-term effects? How likely are
they to occur?
-
What changes may occur that are not danger signs?
-
What kind of diet should my child follow?
-
What are the choices for handling chronic pain, the return of cancer, or the
long-term effects of therapy?
-
What is the best way for me to talk with you about future concerns? (By phone?
At a special appointment? At a regular office visit scheduled in advance to
allow more time?)
-
Who else is available to talk about specific problems?
|
Another concern of parents is what happens to health insurance coverage and
costs after your child has had treatment for cancer. Your child is likely to
continue to be covered under your current insurance, but you may have to pay
more. If you change jobs or apply for a new policy, however, you may have
trouble getting the new coverage for your child, and it may cost more. Older
teenagers who may soon be leaving home and looking for a job need to pay
special attention to insurance needs. Going off their parent's insurance will
mean finding coverage on their own.
One key to making sure your child has insurance coverage is to ask the right
questions before changing jobs and look at what your health insurance coverage
will include if you change policies.
When the Cancer Cannot Be Cured
Although treatments work for many children who have cancer, they do not work
for all. If your child's disease cannot be cured or controlled, you may want to
think about where your child would be most comfortable - in the hospital, at
home, or in a homelike setting. Talk with your child's treatment team about the
different choices available to you and your family. It is important to talk
with your child about what he or she would like. If your child is too young to
speak or does not understand, make a choice based on what you think your child
might want.
Special machines and treatments that can help someone live longer and more
comfortably are often an accepted part of treating a severe illness. For this
reason, many children with terminal cancer and their families choose hospital
care. They want to know that everything in the hospital is available to them.
More and more cancer patients and their families, however, are choosing care
outside of the hospital. As a parent, it is important to know that, with the
help of nurses, doctors, and other health professionals, your child can receive
good care outside the hospital.
Home care is a good choice for many children who have cancer. Home health care
professionals can provide cancer drugs, pain medications, equipment such as
hospital beds or wheelchairs, proper nutrition, physical therapy, and many
complicated nursing and medical care procedures. They also provide emotional
support for you and your child and for brothers, sisters, and other family
members.
Some people choose home care because hospital care can seem cold. Another
advantage of home care is that family and friends, including your child's
friends, can support and help you. Home care involves bringing members of the
home health care team into your house or possibly into the home of a relative
or friend. Depending on the needs and concerns of your child and your family,
the home health team may include all or many of the following professionals:
nurses or nurse practitioners, social workers, dietitians, physical therapists,
pharmacists, oncologists, radiation therapists, clergy, and a psychologist or
psychiatrist. Home health aides also are available to help with bathing,
personal care, or preparing light meals, as needed. In many cases, specially
trained volunteers, called respite care workers, can care for your child when
you need a few hours away from home.
You, your family, and, when possible, your child, will work closely with health
care workers to make sure that your child is comfortable and receives the best
care possible. If 24-hour care is needed, members of the team will work
different shifts to give you and your child around-the-clock support.
Home care is given through various for-profit and not-for-profit private
agencies, public and private hospitals, and public health departments. Your
child's treatment team can give you information on home health care.
Hospice programs provide special care for cancer patients and their families,
either at home or away from home, in separate buildings, or within hospitals. A
team of medical professionals and volunteers works with the family and patient.
The main concerns of hospice caregivers are quality of life and control of
pain.
Hospice caregivers also help family members learn how to care for children who
have terminal cancer. They give emotional, social, and spiritual support during
your child's illness and after your child dies.
About 1,800 hospice programs across the country offer total hospice care. The
National Hospice and Palliative Care Organization encourages and tracks the
quality of hospice care. Children's Hospice International advocates for hospice
care for children. You can find more information about these organizations by
calling the NCI-supported Cancer Information Service (CIS) at 1-800-4-CANCER
(1-800-422-6237) or TTY at 1-800-332- 8615.
During the past several years, health care professionals have become more aware
of the needs of children who have late-stage cancer and of their families. For
example, attending school halfdays or even for an hour a day - if possible -
may make your child happier. Talking with your child about death and dying and
giving your child as many choices as possible shows your child that you are
being open and honest, and shows your support, love, and respect. Paying close
attention to changes in your child's behavior may give you important clues as
to what your child needs and whether he or she wants to talk about dying.
Including all of your children in everyday activities - such as reading, doing
homework, or watching a favorite television program or video together - can
help keep the family close.
Resources

Information about cancer is available from many sources, including the ones
listed here. You may want to check for more information at your local library,
at bookstores, or from support groups in your community
National Cancer Institute Information Resources
You may want more information for yourself, your family, and your doctor. The
following National Cancer Institute (NCI) services are available to help you.
Cancer Information Service (CIS)
Provides accurate, up-to-date information on cancer to patients and their
families, health professionals, and the general public. Information specialists
translate the latest scientific information into understandable language and
respond in English, Spanish, or on TTY equipment.
-
Toll-free: 1-800-4-CANCER (1-800-422-6237)
-
TTY: 1-800-332-8615
www.cancer.gov
NCI's Web site provides comprehensive information about cancer causes and
prevention, screening and diagnosis, treatment and survivorship; clinical
trials; statistics; funding and training; and the Institute's programs and
research activities.
For Additional Information
The Children's Oncology Group (C.O.G.) was formed by the merger of the four
national pediatric cancer research organizations: the Children's Cancer Group,
the Intergroup Rhabdomyosarcoma Study Group, the National Wilms' Tumor Study
Group, and the Pediatric Oncology Group. The primary objective of the
organization is to conduct clinical trials of new therapies for childhood
cancers. Pediatric clinical trials are conducted across the country.
Other Booklets
The National Cancer Institute booklets listed below can be obtained from the
NCI-supported Cancer Information Service (CIS) by calling 1-800-4-CANCER
(1-800-422-6237) or TTY at 1-800-332-8615. Also, many NCI publications may be
viewed or ordered online 8.
Types of Childhood Cancer
| Type |
Description |
Age |
|
| All Leukemias |
Leukemia is cancer of the blood cells. In acute leukemia, the disease comes on
suddenly and gets worse quickly if it is not treated. Most childhood leukemias
are acute. Chronic leukemia is usually milder at the start and gets worse more
slowly. |
|
| Acute lymphoblastic leukemia (ALL) |
Also known as "childhood leukemia" because it is the most
common childhood cancer. |
Usually occurs between 2 and 8 years old. |
| Acute myelogenous leukemia (AML) |
Also called acute nonlymphatic leukemia. |
Usually occurs in people over age 25, but sometimes affects
teenagers and children. |
| Chronic myelogenous leukemia (CML) |
CML is a slowly progressing disease in which too many white
blood cells are made in the bone marrow. Also called chronic myeloid leukemia
or chronic granulocytic leukemia. |
Sometimes occurs in adolescents but almost never affects
children. Most commonly affects adults.
Five percent of childhood leukemias are CML. |
|
| Type |
Description |
Age |
|
| All Lymphomas |
Lymphoma is a tumor of the lymph tissue. Because lymph tissue
is in many parts of the body, lymphomas can start almost anywhere. |
|
| Hodgkin's disease |
Hodgkin's disease is a cancer that tends to affect the lymph
nodes that are close to the body's surface, such as those in the neck, armpit,
or groin area. |
Occurs mainly in young adults and in people over age 65 but
can affect teenagers and children. Lymphomas are the third most common
childhood cancer. Rare under age 5. |
| Non-Hodgkin's lymphoma |
In children, non-Hodgkin's lymphoma affects lymph nodes that
are found deeper in the body. The bowel is the most frequent spot, often in the
area next to the appendix, or in the upper part of the chest. |
Occurs most often in ages 10 to 20. Unusual under age 3. |
| Burkitt's lymphoma |
A type of non-Hodgkin's lymphoma. In Americans, the usual
site is the abdomen. |
Age range is 2-16 years |
|
| Type |
Description |
Age |
|
| Osteosarcoma or osteogenic sarcoma |
Osteosarcoma is the sixth most common malignancy in children
and the most common type of bone cancer in children. Usually affects the thigh
bone (femur), upper arm bone (humerus), or one of the long bones of the lower
leg (tibia). |
Occurs between ages 10 and 25. |
| Ewing's sarcoma |
The most common sites for Ewing's sarcoma are the hipbones,
long bones in the thigh (femur) and upper arm (humerus), and ribs.
|
Occurs between ages 10 and 25. |
| Chondrosarcoma |
Chondrosarcoma forms in cartilage, the rubbery tissue around
the joints. |
Found mainly in adults, although it can occur in children. |
|
| Type |
Description |
Age |
|
| All liver cancers |
Also called hepatoma, liver cancer is a rare disease. When
the tumor is just in the liver and can be removed with surgery, it is highly
curable. Two types of cancer can start in the liver and are identified by how
they look under the microscope. |
|
| Hepatoblastoma |
Hepatoblastoma can be inherited. |
Usually occurs before age 3. |
| Hepatocellular cancer |
Children infected with hepatitis B or C (viral infections of
the liver) are more likely to get this type of cancer. |
Occurs most often in children age 4 or younger and those
between ages 12 and 15. |
|
| Type |
Description |
Age |
|
| All soft tissue sarcomas |
These sarcomas start in soft tissues, which connect, support,
and surround body parts and organs.
|
|
| Rhabdomyosarcoma |
Rhabdomyosarcoma is the most common type of soft tissue
sarcoma. It starts in muscle tissue and can occur anywhere in body. It is most
often found in the head and neck, kidneys, bladder, arms, legs, and trunk. |
Affects children ages 2 to 6 years old. |
|
| Type |
Description |
Age |
|
| Brain cancer |
Brain cancer is the most common solid tumor cancer in
childhood. The most common brain tumors are called gliomas; there are several
types of gliomas.
|
Occurs most often in children from birth to 15 years old. |
| Wilm's tumor or nephroblastoma |
This type of cancer starts in the kidney. It is the most
common type of kidney cancer in children but is very different from kidney
cancer in adults. May be hereditary.
|
Age range 6 months to 10 years - greatest in first 5 years. |
| Neuroblastoma |
Cancer of certain nerve cells of the body is called
neuroblastoma. The second most common solid tumor cancer in children, it
usually starts in abdomen, either in the adrenal glands (located just above
kidneys in back of the upper abdomen) or around the spine. It can also start
around the spinal cord in the chest, neck, or pelvis. |
Occurs most often in babies and very young children. |
| Retinoblastoma |
Retinoblastoma is cancer of the eye. It affects the retina, a
thin membrane in the back of eye that works like a camera, making a picture of
what we see. Some children have retinoblastoma that runs in families. It
usually occurs in only one eye, but sometimes affects both eyes.
|
Occurs mostly in children younger than 5 years old.
|
|
|
|