|
|
|
|
|
A 65 year old Caucasian woman has lived for 30 years in Nigeria. She has taken chemoprophylaxis with primaquine, on a weekly basis. Whenever suspecting a malaria attack, she has treated herself with chloroquine or artesunate. Question 1: Among the chemoprophylaxis regimens below, which THREE would be most suitable for Nigeria?
Question 2: If someone develops a suspected malaria attack while in Nigeria, but cannot get laboratory confirmation within the next 24 hours, which ONE of the options below would be the best for presumptive treatment? (Assume that the person was not taking any chemoprophylaxis.)
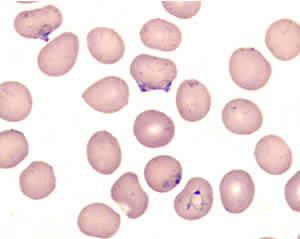
This woman has recently arrived in the United States. Six days after her arrival, she falls and fractures her right wrist. The fracture is treated with a splint and analgesics. Four days later she wakes up at 3 am with nausea, retching and vomiting. She is taken by her daughter to a hospital where she is found to be febrile to 103.4°F. This, combined with the history of stay in Nigeria, prompts a blood smear that shows Plasmodium falciparum with an estimated parasitemia of 3%. Admission is advised but declined, and the patient goes home under the care of her daughter (a physician), with prescriptions for oral quinine and doxycycline. She starts taking the drugs but vomits again. The following day her daughter finds her to be lethargic, hardly able to lift a cup or to answer questions. The patient is brought to another hospital. There, she is found to be febrile, obtunded and unresponsive to painful stimuli. Laboratory findings include: leucocytes 6,300/µL, platelets 40,000/µL, Hb 11 g/dL, creatinine 0.5 mg/dL, glucose 116 mg/dL. Seven hours later, she passes dark urine, which is +++ for blood, +++ for protein, with 10-20 RBCs. Other laboratory findings at that time include: hemoglobin 8.6 g/dL; reticulocytes 2.4%; total bilirubin 6.2 mg/dL; LDH 444 U/L; AST 39 U/L; ALT 16 U/L; alkaline phosphatase 61 U/L. A blood smear shows the following:
Question 3: What is the most likely diagnosis?
Question 4: Which of the following would be suitable for treatment? (more than one might apply)
An intravenous drip of quinidine is started. During the perfusion a prolongation of the QT interval is noted (QT/QTC 444/534 ms), which resolves upon readjustment of the quinidine drip. Shortly after the start of the IV drip the patient's neurologic status improves. Thus, while preparations had been made for an exchange transfusion, this is not carried out. Two units of whole blood are transfused. The parasitemia decreases to 2% the day after admission. On day 2 post admission, the parasites have cleared. On day 4 post-admission the patient has completely recovered. Main points:
Page last modified : April 23, 2004 Content source: Division of Parasitic Diseases National Center for Zoonotic, Vector-Borne, and Enteric Diseases (ZVED)
|
|
||||||||||||||||||||||
| Home | Policies and Regulations | Disclaimer | e-Government | FOIA | Contact Us | ||||||
|