DRAFT
Problem Statement for the AHIC QWG Requirements Analysis
Problem Statement
What health information technology requirements, competencies, and skill sets are needed to collect, aggregate and analyze longitudinal measures that look at patient care quality across entire episodes of care?
Potential Solution
Current quality measurement efforts are based on measures, such as those developed by the HQA and AQA, that are focused on evaluating the delivery of care in one setting (i.e., inpatient, physician office, etc.). These measures look at quality of care using a lens focused on an individual ailment within an isolated encounter. As recognized in the Quality Work Group (QWG) Vision, the health care community recognizes the need to shift measurement from this siloed viewpoint to one that will help assess quality of care across the spectrum of care settings assesses quality from a longitudinal / episodic perspective.
Proposal for Guiding QWG Efforts
We propose that the QWG focus their efforts for the next six months on identifying how health information technology can support longitudinal measurement. This involves identifying how data could be collected, aggregated, and analyzed in the future. This approach will help focus QWG efforts to collect and analyze testimony and develop targeted recommendations to the Secretary of HHS to ensure that health information technology supports longitudinal measurement. More importantly, it will help to inform public and private sector dialogue about the alternative approaches for using technology to advance the QWG vision.
One aspect of the quality measurement and improvement infrastructure that can be addressed by looking at longitudinal measurement is the integration of multiple data sources to inform measures. Currently, most longitudinal quality measurement use claims data as a primary data source. There are severe limitations with this approach as measures that use claims data are limited in their clinical perspective and measure results can only be applied retrospectively to achieve improvements in care delivered in the future. As the industry increases its use of EHRs and explores methods to integrate other data sources such as pharmacy dispensing information, lab data, and data across organizations, there will be a transition from predominantly sole-source measurement to multi-source measurement. By focusing on longitudinal measurement, QWG efforts can help define the critical path towards making this transition from primarily sole-sourced to multi-source measurement. Our focus is on defining the intermediate and long term states and identifying the enablers and barriers to achieving this vision.
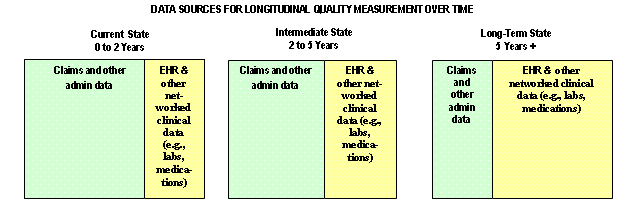
Image Description: In the current state, from zero to two years, claims and other admin data are the source of about two-thirds of the data, and EHR and other networked clinical data, for example, labs, medications, are the source of about one-third of the data. In the intermediate state, from two to five years, claims and other admin data are the source of about 60 percent of the data, and EHR and other networked clinical data, for example, labs, medications, are the source of about 40 percent of the data. In the long-term state, five years and longer, claims and other admin data are the source of about one-third of the data, and EHR and other networked clinical data, for example, labs, medications, are the source of about two-thirds of the data.
Proposed Approach
The scope of the requirements includes all diseases, however to guide the initial stages of the requirements analysis we believe it will be useful to choose sample conditions to make the conversations concrete. We propose that the QWG select one acute and one chronic illness to develop general business and high-level system requirements for each of these two major categories of illness. These requirements will detail how HIT can be used to help answer questions such as:
-
What methods could be used to identify patients that are included in populations under study for quality?
-
What methods could be used to collect information to inform longitudinal analysis? How should the numerator and denominator for longitudinal measures be defined? What role will claims data play in the future? Where is it most important to have clinical data from EHRs?
-
What methods could be used to aggregate this data? What types of competencies will be required? Could those competencies reasonably be found in the multiple communities?
-
What methods could be used to analyze it?
-
How can concurrent feedback be achieved? Episode construction is currently done through a retrospective analysis of claims data. In the future, could prospective and/or concurrent episode construction be possible due to more widespread use and functionality of EHRs? Could a feedback loop reasonably be used to create health system alerts to improve care before episodes are complete?
If QWG determines this approach is feasible, it can be further fleshed out and used as a construct or framework that can guide and focus QWG activities both in the immediate future and the longer-term.
Immediate efforts will focus on gathering enough requirements through an environmental scan, interviews, and testimony to inform the recommendations due to the Secretary of HHS in Fall 2007 and will be the focus area for our first requirements analysis cycle. Subsequent requirements analysis cycles will continue focusing on the topics outlined above, looking at them through the lens of longitudinal measures, but will focus on specific areas in more detail as dictated by the QWG and by the amount of investigation required to develop sound recommendations.
The longer-term analysis, i.e., the simulation or “what if” analysis, will look at the quality measurement and improvement infrastructure and help assess and recommend paths to achieve the envisioned future state by looking at the use of varying options for the infrastructure.
Appendix A: Example Scenario for Consideration Diabetes
Longitudinal measurement is particularly important when considering chronic illnesses, though there are also many cases where longitudinal measurement is needed for acute care as well. Diabetes is an example of a chronic illness where quality measurement from a longitudinal perspective would significantly increase the ability to manage the patient’s treatment and ensure high quality care is being delivered. Diabetes treatment is often provided by multiple physicians through multiple visits, and in both inpatient and outpatient care settings. The patient may have separate physicians for related eye exams, foot exams, for monitoring blood levels, such as HbA1c. Additionally, the patient may have been hospitalized due to diabetes-related complications such as heart disease, stroke, kidney failure, blindness and/or circulation problems.
Current diabetes care measurement only looks at treatment from a single lens, either inpatient or outpatient, and focuses on only one aspect of the full spectrum of treatment a diabetes patient may require. For example, measurement of HbA1c control for an individual visit is useful, but in order to really assess diabetes control, looking at HbA1c levels over the course of the year can provide valuable information regarding how well the patient is managing their illness and will help the physician determine what course of actions to take to help control the diabetes.