Introduction
The Cervix
Understanding Cancer
Risk Factors
Screening
Symptoms
Diagnosis
Staging
Treatment
Side Effects of Treatment
Complementary and Alternative Medicine
Nutrition
Follow-up Care
Sources of Support
The Promise of Cancer Research
National Cancer Institute Information Resources
National Cancer Institute Publications
Introduction
This National Cancer Institute (NCI) booklet (NIH Publication No. 05-2047) has important information about
cancer* of the cervix. Cancer of the cervix is also called cervical cancer. You
will read about causes, screening, symptoms, diagnosis, and treatment. You will
also find ideas about how to cope with the disease.
Scientists are studying cervical cancer to find out more about how it develops.
And they are looking at better ways to detect and treat it.
The NCI provides information about cancer, including the publications mentioned
in this booklet. You can order these materials by telephone or on the Internet.
You can also read them on the Internet and print your own copy.
-
Telephone (1-800-4-CANCER): Information Specialists at NCI's Cancer Information
Service can answer your questions about cancer. They also can send NCI
booklets, fact sheets, and other materials.
-
Internet (http://www.cancer.gov): You can use NCI's Web site to
find a wide range of up-to-date information. For example, you can find many NCI
booklets and fact sheets at http://www.cancer.gov/publications.
People in the United States and its territories may use this Web site to order
printed copies. This Web site also explains how people outside the United
States can mail or fax their requests for NCI booklets.
You can ask questions online and get help right away from Information
Specialists through
LiveHelp 1. (Click on "Need Help?" at http://www.cancer.gov.
Then click on "Connect to LiveHelp.")
*Words that may be new to readers appear in italics. "Dictionary" 2 explains these terms. Some words in the "Dictionary" have a "sounds-like" spelling to show how to pronounce them.
The Cervix
The
cervix is part of a woman's
reproductive system. It is the lower, narrow part of the
uterus (womb). The uterus is a
hollow, pear-shaped
organ
in the lower
abdomen. The cervix connects the
uterus to the
vagina. The vagina leads to the
outside of the body.
The
cervical canal is a passageway.
Blood flows from the uterus through the canal into the vagina during a woman's
menstrual period. The cervix also
produces
mucus. The mucus helps
sperm move from the vagina into the
uterus. During pregnancy, the cervix is tightly closed to help keep the baby
inside the uterus. During childbirth, the cervix
dilates (opens) to allow the baby
to pass through the vagina.
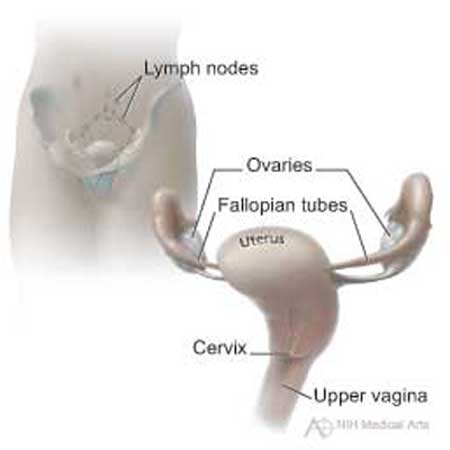 This picture shows the cervix and nearby organs.
This picture shows the cervix and nearby organs.
|
Understanding Cancer
Cancer begins in
cells, the building blocks that
make up
tissues. Tissues make up the organs of the body.
Normally, cells grow and divide to form new cells as the body needs them. When
cells grow old, they die, and new cells take their place.
Sometimes, this orderly process goes wrong. New cells form when the body does
not need them, and old cells do not die when they should. These extra cells can
form a mass of tissue called a growth or
tumor.
Tumors can be
benign
or
malignant:
Benign tumors are not cancer:
-
Benign tumors are rarely life-threatening.
-
Generally, benign tumors can be removed, and they usually do not grow back.
-
Cells from benign tumors do not invade the tissues around them.
-
Cells from benign tumors do not spread to other parts of the body.
-
Polyps,
cysts,
and
genital warts
are types of benign growths on the cervix.
Malignant tumors are cancer:
-
Malignant tumors are generally more serious than benign tumors. They may be
life-threatening.
-
Malignant tumors often can be removed. But sometimes they grow back.
-
Cells from malignant tumors can invade and damage nearby tissues and organs.
-
Cells from malignant tumors can spread
(metastasize)
to other parts of the
body. Cancer cells spread by breaking away from the original
(primary) tumor
and entering the bloodstream or
lymphatic system. The cells invade other organs
and form new tumors that damage these organs. The spread of cancer is called
metastasis.
When cancer spreads from its original place to another part of the body, the
new tumor has the same kind of abnormal cells and the same name as the primary
tumor. For example, if cervical cancer spreads to the lungs, the cancer cells
in the lungs are actually cervical cancer cells. The disease is metastatic
cervical cancer, not lung cancer. For that reason, it is treated as cervical
cancer, not lung cancer. Doctors call the new tumor "distant" or metastatic
disease.
Risk Factors
Doctors cannot always explain why one woman develops cervical cancer and
another does not. However, we do know that a woman with certain
risk factors
may be more likely than others to develop cervical cancer. A risk factor is
something that may increase the chance of developing a disease.
Studies have found a number of factors that may increase the risk of cervical
cancer. These factors may act together to increase the risk even more:
-
Human papillomaviruses (HPVs):
HPV
infection
is the main risk factor for
cervical cancer. HPV is a group of
viruses
that can infect the cervix. HPV
infections are very common. These viruses can be passed from person to person
through sexual contact. Most adults have been infected with HPV at some time in
their lives. Some types of HPV can cause changes to cells in the cervix. These
changes can lead to genital warts, cancer, and other problems. Doctors may
check for HPV even if there are no warts or other
symptoms.
If a woman has an HPV infection, her doctor can discuss ways to avoid infecting
other people. The
Pap test
can detect cell changes in the cervix caused by HPV.
(See the "Screening" 3 section to learn more about the Pap test.)
Treatment of these cell changes can prevent cervical cancer. There are several
treatment methods, including freezing or burning the infected tissue. Sometimes
medicine also helps.
The NCI offers a fact sheet called
"Human Papillomaviruses and Cancer: Questions and Answers." 4
-
Lack of regular Pap tests: Cervical cancer is more common among women who do
not have regular Pap tests. The Pap test helps doctors find
precancerous
cells.
Treating precancerous cervical changes often prevents cancer.
-
Weakened immune system
(the body's natural defense system): Women with
HIV
(the
virus that causes
AIDS)
infection or who take drugs that suppress the immune
system have a higher-than-average risk of developing cervical cancer. For these
women, doctors suggest regular
screening
for cervical cancer.
-
Age: Cancer of the cervix occurs most often in women over the age of 40.
-
Sexual history: Women who have had many sexual partners have a
higher-than-average risk of developing cervical cancer. Also, a woman who has
had sexual intercourse with a man who has had many sexual partners may be at
higher risk of developing cervical cancer. In both cases, the risk of
developing cervical cancer is higher because these women have a
higher-than-average risk of HPV infection.
-
Smoking cigarettes: Women with an HPV infection who smoke cigarettes have a
higher risk of cervical cancer than women with HPV infection who do not smoke.
-
Using birth control pills for a long time: Using birth control pills for a long
time (5 or more years) may increase the risk of cervical cancer among women
with HPV infection.
-
Having many children: Studies suggest that giving birth to many children may
increase the risk of cervical cancer among women with HPV infection.
Diethylstilbestrol
(DES) may increase the risk of a rare form of cervical
cancer and certain other cancers of the reproductive system in daughters
exposed to this drug before birth. DES was given to some pregnant women in the
United States between about 1940 and 1971. (It is no longer given to pregnant
women.)
Women who think they may be at risk for cancer of the cervix should discuss
this concern with their doctor. They may want to ask about a schedule for
checkups. For more information about risk factors, see the NCI booklet
Understanding Cervical Changes 5.
Screening
Screening to check for cervical changes before there are symptoms is very
important. Screening can help the doctor find abnormal cells before cancer
develops. Finding and treating abnormal cells can prevent most cervical cancer.
Also, screening can help find cancer early, when treatment is more likely to be
effective.
For the past several decades, the number of women diagnosed each year with
cervical cancer has been falling. Doctors believe this is mainly because of the
success of screening.
Doctors recommend that women help reduce their risk of cervical cancer by
having regular Pap tests. A Pap test (sometimes called Pap smear or cervical
smear) is a simple test used to look at cervical cells. For most women, the
test is not painful. A Pap test is done in a doctor's office or clinic during a
pelvic exam. The doctor or nurse
scrapes a sample of cells from the cervix, and then smears the cells on a glass
slide. In a new type of Pap test (liquid-based
Pap test), the cells are rinsed into a small
container of liquid. A special machine puts the cells onto slides. For both
types of Pap test, a lab checks the cells on the slides under a microscope for
abnormalities.
Pap tests can find cervical cancer or abnormal cells that can lead to cervical
cancer. Doctors generally recommend that:
-
Women should begin having Pap tests 3 years after they begin having sexual
intercourse, or when they reach age 21 (whichever comes first).
-
Most women should have a Pap test at least once every 3 years.
-
Women aged 65 to 70 who have had at least three normal Pap tests and no
abnormal Pap tests in the past 10 years may decide, after speaking with their
doctor, to stop cervical cancer screening.
-
Women who have had a
hysterectomy (surgery)
to remove the uterus and cervix, also called a
total hysterectomy, do not need to
have cervical cancer screening. However, if the surgery was treatment for
precancerous cells or cancer, the woman should continue with screening.
Women should talk with their doctor about when they should begin having Pap
tests, how often to have them, and when they can stop having them. This is
especially important for women at higher-than-average risk of cervical cancer.
Some activities can hide abnormal cells and affect Pap test results. Doctors
suggest the following tips:
-
Do not
douche for 48 hours before the
test.
-
Do not have sexual intercourse for 48 hours before the test.
-
Do not use vaginal medicines (except as directed by a doctor) or birth control
foams, creams, or jellies for 48 hours before the test.
Doctors also suggest that a woman schedule her Pap test for a time that is 10
to 20 days after the first day of her menstrual period.
Most often, abnormal cells found by a Pap test are not cancerous. However, some
abnormal conditions may become cancer over time:
-
LSIL (low-grade
squamous intraepithelial lesion):
LSILs are mild cell changes on the surface of the cervix. Such changes often
are caused by HPV infections. LSILs are common, especially in young women.
LSILs are not cancer. Even without treatment, most LSILs stay the same or go
away. However, some turn into high-grade lesions, which may lead to cancer.
-
HSIL (high-grade squamous
intraepithelial lesion): HSILs are not cancer, but without treatment they may
lead to cancer. The precancerous cells are only on the surface of the cervix.
They look very different from normal cells.
The NCI booklet Understanding
Cervical Changes 5 has more information about abnormal Pap test results.
You also may want to read the brochure Having a Pelvic Exam and Pap Test
and the NCI fact sheet "The Pap Test: Questions and Answers." 6
You may want to ask the doctor the following questions about screening:
- How soon after the test will I learn the results?
- Do you recommend that I get tested for HPV?
- How much do the tests cost? Will my health insurance help pay for screening tests?
|
Symptoms
Precancerous changes and early cancers of the cervix generally do not cause pain or other symptoms. It is important not to wait to feel pain before seeing a doctor.
When the disease gets worse, women may notice one or more of these symptoms:
- Abnormal vaginal bleeding
- Bleeding that occurs between regular menstrual periods
- Bleeding after sexual intercourse, douching, or a pelvic exam
- Menstrual periods that last longer and are heavier than before
- Bleeding after
menopause
- Increased vaginal discharge
- Pelvic pain
- Pain during sexual intercourse
Infections or other health problems may also cause these symptoms. Only a doctor can tell for sure. A woman with any of these symptoms should tell her doctor so that problems can be diagnosed and treated as early as possible.
Diagnosis
If a woman has a symptom or Pap test results that suggest precancerous cells or
cancer of the cervix, her doctor will suggest other procedures to make a
diagnosis.
These may include:
-
Colposcopy: The doctor uses a
colposcope
to look at the cervix. The colposcope
combines a bright light with a magnifying lens to make tissue easier to see. It
is not inserted into the vagina. A colposcopy is usually done in the doctor's
office or clinic.
-
Biopsy
: The doctor removes tissue to look for precancerous cells or cancer
cells. Most women have their biopsy in the doctor's office with
local anesthesia. A
pathologist
checks the tissue with a microscope.
-
Punch biopsy: The doctor uses a sharp, hollow device to pinch off small samples
of cervical tissue.
-
LEEP: The doctor uses an electric wire loop to slice off a thin, round piece of
tissue.
-
Endocervical curettage: The doctor uses a
curette
(a small, spoon-shaped
instrument) to scrape a small sample of tissue from the cervical canal. Some
doctors may use a thin, soft brush instead of a curette.
-
Conization: The doctor removes a cone-shaped sample of tissue. A conization, or
cone biopsy, lets the pathologist see if abnormal cells are in the tissue
beneath the surface of the cervix. The doctor may do this test in the hospital
under
general anesthesia. Conization also may be used to remove a precancerous
area.
Removing tissue from the cervix may cause some bleeding or other discharge. The
area usually heals quickly. Women may also feel some pain similar to menstrual
cramps. Medicine can relieve this discomfort.
For more information about tests, cell changes, and treatment for these
changes, you may want to read
Understanding Cervical Changes 5.
You may want to ask the doctor these questions before having a procedure:
- Which test(s) do you recommend?
- How will the test be done?
- Will I have to go to the hospital?
- How long will it take? Will I be awake? Will it hurt?
- Are there any risks? What are the chances of infection or bleeding after the procedure?
- Can the test affect my ability to get pregnant and have children?
- How soon will I know the results? Who will explain them to me?
- If I do have cancer, who will talk to me about the next steps? When?
|
Staging
If the biopsy shows that you have cancer, your doctor will do a thorough pelvic
exam and may remove additional tissue to learn the extent
(stage) of your
disease. The stage tells whether the tumor has invaded nearby tissues, whether
the cancer has spread and, if so, to what parts of the body.
These are the stages of cervical cancer:
-
Stage 0: The cancer is found only in the top layer of cells in the tissue that
lines the cervix. Stage 0 is also called
carcinoma in situ.
-
Stage I: The cancer has invaded the cervix beneath the top layer of cells. It
is found only in the cervix.
-
Stage II: The cancer extends beyond the cervix into nearby tissues. It extends
to the upper part of the vagina. The cancer does not invade the lower third of
the vagina or the
pelvic wall
(the lining of the part of the body between the
hips).
-
Stage III: The cancer extends to the lower part of the vagina. It also may have
spread to the pelvic wall and nearby
lymph nodes.
-
Stage IV: The cancer has spread to the
bladder,
rectum,
or other parts of the
body.
-
Recurrent cancer: The cancer was treated, but has returned after a period of
time during which it could not be detected. The cancer may show up again in the
cervix or in other parts of the body.
To learn the extent of disease and suggest a course of treatment, the doctor
may order some of the following tests:
-
Chest
x-rays: X-rays often can show whether cancer has spread to the lungs.
-
CT scan: An x-ray machine linked to a computer takes a series of detailed
pictures of your organs. You may receive
contrast material
by
injection
in your
arm or hand, by mouth, or by
enema. (Some people are allergic to contrast
materials that contain iodine. Tell your doctor or nurse if you have
allergies.) The contrast material makes abnormal areas easier to see. A tumor
in the liver, lungs, or elsewhere in the body can show up on the CT scan.
-
MRI: A powerful magnet linked to a computer is used to make detailed pictures
of your pelvis and abdomen. The doctor can view these pictures on a monitor and
can print them on film. An MRI can show whether cancer has spread. Sometimes
contrast material makes abnormal areas show up more clearly on the picture.
-
Ultrasound:
An ultrasound device is held against the abdomen or inserted into
the vagina. The device sends out sound waves that people cannot hear. The waves
bounce off the cervix and nearby tissues, and a computer uses the echoes to
create a picture. Tumors may produce echoes that are different from the echoes
made by healthy tissues. The picture can show whether cancer has spread.
 |
Treatment
Many women with cervical cancer want to take an active part in making decisions
about their medical care. It is natural to want to learn all you can about your
disease and your treatment choices. However, shock and stress after the
diagnosis can make it hard to think of everything you want to ask the doctor.
It often helps to make a list of questions before an appointment.
To help remember what the doctor says, you may take notes or ask whether you
may use a tape recorder. You may also want to have a family member or friend
with you when you talk to the doctor - to take part in the discussion, to take
notes, or just to listen.
You do not need to ask all your questions at once. You will have other chances
to ask your doctor to explain things that are not clear and to ask for more
information.
Your doctor may refer you to a specialist, or you may ask for a referral.
Gynecologists,
gynecologic oncologists,
medical oncologists, and
radiation oncologists
are specialists who treat cervical cancer.
Before starting treatment, you might want a second opinion about the diagnosis
and treatment plan. Many insurance companies cover a second opinion if you or
your doctor requests it. It may take some time and effort to gather medical
records and arrange to see another doctor. Usually it is not a problem to take
several weeks to get a second opinion. In most cases, the delay in starting
treatment will not make treatment less effective. To make sure, you should
discuss this delay with your doctor. Some women with cervical cancer need
treatment right away.
There are a number of ways to find a doctor for a second opinion:
-
Your doctor may refer you to one or more specialists. At cancer centers,
several specialists often work together as a team.
-
NCI's Cancer Information Service, at 1-800-4-CANCER, can tell you about nearby
treatment centers. Information Specialists also can provide online assistance
through
LiveHelp 1 at http://www.cancer.gov.
-
A local or state medical society, a nearby hospital, or a medical school can
usually provide the names of specialists in your area.
-
The American Board of Medical Specialties (ABMS) has a list of doctors who have
had training and passed exams in their specialty. You can find this list in the
Official ABMS Directory of Board Certified Medical Specialists. This Directory
is in most public libraries. Or you can look up doctors at
http://www.abms.org 7. (Click on "Who's Certified.")
-
The NCI provides a helpful fact sheet called "How To Find a Doctor or Treatment
Facility If You Have Cancer." 8
The choice of treatment depends mainly on the size of the tumor and whether the
cancer has spread. If a woman is of childbearing age, the treatment choice may
also depend on whether she wants to become pregnant someday.
Your doctor can describe your treatment choices and the expected results of
each. You and your doctor can work together to develop a treatment plan that
meets your medical needs and personal values.
You may want to ask the doctor these questions before treatment begins:
- What is the stage of my disease? Has the cancer spread? If so, where?
- What are my treatment choices? Which do you recommend for me? Will I have more than one kind of treatment?
- What are the expected benefits of each kind of treatment?
- What are the risks and possible
side effects
of each treatment? What can we do to control my side effects?
- How will treatment affect my normal activities?
- What can I do to take care of myself during treatment?
- How long will treatment last?
- Will I have to stay in the hospital?
- What is the treatment likely to cost? Does my insurance cover this treatment?
- How often should I have checkups?
- Would a
clinical trial
(research study) be appropriate for me?
|
Women with cervical cancer may be treated with surgery,
radiation therapy,
chemotherapy,
radiation therapy and chemotherapy, or a combination of all three
methods.
At any stage of disease, women with cervical cancer may have treatment to
control pain and other symptoms, to relieve the side effects of therapy, and to
ease emotional and practical problems. This kind of treatment is called
supportive care,
symptom management,
or
palliative care.
Information about such
treatment is available on NCI's Web site at http://www.cancer.gov/cancertopics/coping
and from NCI's Cancer Information Service at 1-800-4-CANCER.
You may want to talk to your doctor about taking part in a clinical trial, a
research study of new treatment methods. The section on
"The Promise of Cancer Research" 9 has more information about clinical trials.
Surgery treats the cancer in the cervix and the area close to the tumor.
Most women with early cervical cancer have surgery to remove the cervix and
uterus (total hysterectomy). However, for very early (Stage 0) cervical cancer,
a hysterectomy may not be needed. Other ways to remove the cancerous tissue
include
conization,
cryosurgery,
laser surgery,
or
LEEP.
Some women need a
radical hysterectomy. A radical hysterectomy is surgery to
remove the uterus, cervix, and part of the vagina.
With either total or radical hysterectomy, the
surgeon
may remove both
fallopian tubes
and
ovaries. (This procedure is a
salpingo-oophorectomy.)
The surgeon may also remove the lymph nodes near the tumor to see if they
contain cancer. If cancer cells have reached the lymph nodes, it means the
disease may have spread to other parts of the body.
You may want to ask the doctor these questions about surgery:
- What kind of operation will I have? Will my ovaries be removed?
- Do I need to have lymph nodes removed? Will other tissues be removed? Why?
- How will I feel after the operation?
- If I have pain, how will it be controlled?
- How long will I have to stay in the hospital?
- Will I have any lasting side effects? If I don't have a hysterectomy, will I be able to get pregnant and have children? Is there increased risk of miscarriage?
- When will I be able to resume normal activities?
- How will the surgery affect my sex life?
|
Radiation therapy (also called radiotherapy) uses high-energy rays to kill
cancer cells. It affects cells only in the treated area.
Women have radiation therapy alone, with chemotherapy, or with chemotherapy and
surgery. The doctor may suggest radiation therapy instead of surgery for the
small number of women who cannot have surgery for medical reasons. Most women
with cancer that extends beyond the cervix have radiation therapy and
chemotherapy. For cancer that has spread to distant organs, radiation therapy
alone may be used.
Doctors use two types of radiation therapy to treat cervical cancer. Some women
receive both types:
-
External radiation:
The radiation comes from a large machine outside the body.
The woman usually has treatment as an outpatient in a hospital or clinic. She
receives external radiation 5 days a week for several weeks.
-
Internal radiation
(intracavitary radiation): Thin tubes (also called implants)
containing a
radioactive
substance are left in the vagina for a few hours or up
to 3 days. The woman may stay in the hospital during that time. To protect
others from the radiation, the woman may not be able to have visitors or may
have visitors for only a short period of time while the tubes are in place.
Once the tubes are removed, no radioactivity is left in her body. Internal
radiation may be repeated two or more times over several weeks.
You may want to ask the doctor these questions before having radiation therapy:
- What is the goal of this treatment?
- How will the radiation be given?
- Will I need to stay in the hospital? If so, for how long?
- When will the treatments begin? When will they end?
- How will I feel during therapy? Are there side effects?
- How will we know if the radiation therapy is working?
- Will I be able to continue my normal activities during treatment?
- How will radiation therapy affect my sex life?
- Will I be able to get pregnant and have children after my treatment is over?
|
Chemotherapy uses anticancer drugs to kill cancer cells. It is called
systemic therapy
because the drugs enter the bloodstream and can affect cells all over
the body. For treatment of cervical cancer, chemotherapy is generally combined
with radiation therapy. For cancer that has spread to distant organs,
chemotherapy alone may be used.
Anticancer drugs for cervical cancer are usually given through a vein. Women
usually receive treatment in an outpatient part of the hospital, at the
doctor's office, or at home. Rarely, a woman needs to stay in the hospital
during treatment.
You may want to ask the doctor these questions before having chemotherapy:
- Why do I need this treatment?
- Which drug or drugs will I have?
- How do the drugs work?
- What are the expected benefits of the treatment?
- What are the risks and possible side effects of treatment? What can we do about them?
- When will treatment start? When will it end?
- How will treatment affect my normal activities?
|
Side Effects of Treatment
Because cancer treatment often damages healthy cells and tissues, unwanted side
effects are common. Side effects depend mainly on the type and extent of the
treatment. Side effects may not be the same for each woman, and they may change
from one treatment session to the next. Before treatment starts, your health
care team will explain possible side effects and suggest ways to help you
manage them.
The NCI provides helpful booklets about cancer treatments and coping with side
effects. These include
Radiation Therapy and You 10,
Chemotherapy and You 11, and
Eating Hints for Cancer Patients 12.
It takes time to heal after surgery, and the recovery time is different for
each woman. You may be uncomfortable for the first few days. However, medicine
can usually control the pain. Before surgery, you should discuss the plan for
pain relief with your doctor or nurse. After surgery, your doctor can adjust
the plan if you need more pain relief.
If you have surgery to remove a small tumor on the surface of the cervix, you
may have cramping or other pain, bleeding, or a watery discharge.
If you have a hysterectomy, the length of the hospital stay may vary from
several days to a week. It is common to feel tired or weak for a while. You may
have problems with nausea and vomiting, and you may have bladder and bowel
problems. The doctor may restrict your diet to liquids at first, with a gradual
return to solid food. Most women return to their normal activities within 4 to
8 weeks after surgery.
After a hysterectomy, women no longer have menstrual periods. They cannot
become pregnant.
When the ovaries are removed, menopause occurs at once. Hot flashes and other
symptoms of menopause caused by surgery may be more severe than those caused by
natural menopause. You may wish to discuss this with your doctor before
surgery. Some drugs have been shown to help with these symptoms, and they may
be more effective if started before surgery.
After surgery, some women may be concerned about sexual intimacy. Many women
find that it helps to share these concerns with their partner. A couple may
want to ask a counselor to help them express their concerns.
Side effects depend mainly on the dose of radiation and the part of your body
that is treated. Radiation to the abdomen and pelvis may cause nausea,
vomiting, diarrhea, or urinary problems. You may lose hair in your genital
area. Also, your skin in the treated area may become red, dry, and tender.
You may have dryness, itching, or burning in your vagina. The radiation may
also make your vagina narrower. The doctor or nurse may suggest ways to relieve
discomfort. There also are ways to expand the vagina, which will help make
follow-up exams easier. Your doctor may advise you not to have intercourse
during treatment. But most women can resume sexual activity within a few weeks
after treatment ends.
You are likely to become very tired during radiation therapy, especially in the
later weeks of treatment. Resting is important, but doctors usually advise
patients to try to stay as active as they can.
Although the side effects of radiation therapy can be distressing, your doctor
can usually find ways to relieve them.
The side effects of chemotherapy depend mainly on the specific drugs and the
dose. The drugs affect cancer cells and other cells that divide rapidly:
-
Blood cells: These cells fight infection, help your blood to clot, and carry
oxygen to all parts of the body. When drugs affect your blood cells, you are
more likely to get infections, bruise or bleed easily, and feel very weak and
tired.
-
Cells in hair roots: Chemotherapy can cause you to lose your hair. The hair
will grow back, but it may be somewhat different in color and texture.
-
Cells that line the
digestive tract: Chemotherapy can cause a poor appetite,
nausea and vomiting, diarrhea, or mouth and lip sores.
The drugs used for cervical cancer also may cause skin rash, hearing problems,
loss of balance, joint pain, or swollen legs and feet.
Your doctor can suggest ways to control many of these side effects.
Complementary and Alternative Medicine
Some people with cancer use
complementary and alternative medicine
(CAM) to ease stress or to reduce side effects and symptoms:
- An approach is generally called complementary medicine when it is used along with standard treatment.
- An approach is called alternative medicine when it is used instead of standard treatment.
Acupuncture,
massage therapy, herbal products, vitamins or special diets, visualization, meditation, and spiritual healing are types of CAM. Many people say that such approaches help them feel better.
However, some types of CAM, including certain vitamins, may interfere with standard treatment. Combining CAM with standard treatment may even be harmful. Before trying any type of CAM, you should discuss its possible benefits and harmful effects with your doctor.
Some types of CAM are expensive. Health insurance may not cover the cost.
The NCI offers a fact sheet called
"Complementary and Alternative Medicine in Cancer Treatment: Questions and Answers." 13
Nutrition
It is important to eat well during cancer treatment. Eating well means getting
enough calories to maintain a good weight and enough protein to keep up your
strength. Good nutrition often helps people with cancer feel better and have
more energy.
But eating well can be difficult. You may not feel like eating if you are
uncomfortable or tired. Also, the side effects of treatment (such as poor
appetite, nausea, vomiting, or mouth sores) can be a problem. Some people find
that foods do not taste as good during cancer therapy.
The doctor, a
dietitian,
or another health care provider can suggest ways to
maintain a healthy diet. The NCI booklet
Eating Hints for Cancer Patients 12 has
many useful ideas and recipes.
Follow-up Care
Follow-up care after treatment for cervical cancer is important. Even when the
cancer seems to have been completely removed or destroyed, the disease
sometimes returns because undetected cancer cells remained somewhere in the
body after treatment. Your doctor will monitor your recovery and check for
recurrence
of the cancer. Checkups help ensure that any changes in your health
are noted and treated as needed. Checkups may include a physical exam as well
as Pap tests and chest x-rays. Between scheduled visits, you should contact the
doctor right away if you have any health problems.
To help answer questions about follow-up care and other concerns, NCI has a
booklet for people who have completed their treatment.
Facing Forward Series:
Life After Cancer Treatment 14 provides tips for making the best use of medical
visits. It describes how to talk with the doctor about creating a plan of
action for your recovery and future health.
Sources of Support
Living with a serious disease such as cervical cancer is not easy. You may
worry about caring for your family, keeping your job, or continuing daily
activities. Concerns about treatments and managing side effects, hospital
stays, and medical bills are also common. Doctors, nurses, and other members of
the health care team can answer questions about treatment, working, or other
activities. Meeting with a social worker, counselor, or member of the clergy
can be helpful if you want to talk about your feelings or concerns. Often, a
social worker can suggest resources for financial aid, transportation, home
care, or emotional support.
Support groups also can help. In these groups, patients or their family members
meet with other patients or their families to share what they have learned
about coping with the disease and the effects of treatment. Groups may offer
support in person, over the telephone, or on the Internet. You may want to talk
with a member of your health care team about finding a support group.
Cancer Information Specialists at 1-800-4-CANCER and at
LiveHelp 1 (http://www.cancer.gov) can help you
locate programs, services, and publications. Also, you may want to see the NCI
fact sheets called "Cancer Support Groups: Questions and Answers" 15 and
"National Organizations That Offer Services to People With Cancer and Their Families." 16
The Promise of Cancer Research
Doctors all over the country are conducting many types of clinical trials
(research studies in which people volunteer to take part). They are studying
new ways to treat cervical cancer. Some are also studying therapies that may
improve the
quality of life
for women during or after cancer treatment.
Clinical trials are designed to answer important questions and to find out
whether new approaches are safe and effective. Research already has led to many
advances, and researchers continue to search for more effective methods for
dealing with cancer.
Researchers are testing new approaches to treatment, including anticancer drugs
and drug combinations. They also are studying different methods, doses, and
schedules of radiation therapy. Some trials are combining chemotherapy,
surgery, and radiation therapy. Other trials are researching
biological therapy.
Researchers also are studying surgery to remove
sentinel lymph nodes.
A
sentinel lymph node is the first lymph node to which the cancer is likely to
spread. Today, surgeons often have to remove many lymph nodes and check each of
them for cancer. But if the research shows that it is possible to identify the
sentinel lymph node (the lymph node most likely to have cancer), doctors may be
able to avoid more surgery to remove other lymph nodes.
People who join clinical trials may be among the first to benefit if a new
approach is effective. And even if participants do not benefit directly, they
still make an important contribution to medicine by helping doctors learn more
about the disease and how to control it. Although clinical trials may pose some
risks, researchers do all they can to protect their patients.
If you are interested in being part of a clinical trial, talk with your doctor.
You may want to read the NCI booklet Taking Part in Cancer Treatment Research Studies 17. It explains how clinical trials are carried out and explains their possible benefits and risks.
NCI's Web site includes a section on clinical trials at http://www.cancer.gov/clinicaltrials.
It has general information about clinical trials as well as detailed
information about specific ongoing studies of cervical cancer. Information
Specialists at 1-800-4-CANCER or at
LiveHelp 1 at http://www.cancer.gov can answer
questions and provide information about clinical trials.
National Cancer Institute Information Resources
You may want more information for yourself, your family, and your doctor. The
following National Cancer Institute (NCI) services are available to help you.
Cancer Information Service (CIS)
The CIS provides accurate, up-to-date information on cancer to patients and
their families, health professionals, and the general public. Information
Specialists translate the latest scientific information into understandable
language and respond in English, Spanish, or on TTY equipment. Calls to the CIS
are free.
Telephone: 1-800-4-CANCER (1-800-422-6237)
TTY: 1-800-332-8615
The NCI's Web site (http://www.cancer.gov) provides information from numerous
NCI sources. It offers current information on cancer prevention, screening,
diagnosis, treatment, genetics, supportive care, and ongoing clinical trials.
It has information about NCI's research programs and funding opportunities,
cancer statistics, and the Institute itself. Information Specialists provide
live, online assistance through LiveHelp 1.
National Cancer Institute Publications
National Cancer Institute (NCI) publications can be ordered by writing to the
address below: Publications Ordering Service
National Cancer Institute
Suite 3035
6116 Executive Boulevard, MSC 8322
Bethesda, MD 20892-8322
Many NCI publications can be viewed, downloaded, and ordered from
http://www.cancer.gov/publications on the Internet. In addition, people in the
United States and its territories may order these and other NCI publications by
calling the Cancer Information Service at 1-800-4-CANCER.
|
|
