Identifying Individuals at High Risk of Melanoma:
A Practical Predictor of Absolute Risk
Thomas R. Fears1, DuPont Guerry IV2, Ruth M. Pfeiffer1, Richard W. Sagebiel3, David E. Elder2, Allan Halpern4, Elizabeth A. Holly3, Patricia Hartge1, and Margaret A. Tucker1
J Clin Oncol 24: Online May 25, 2006
From the 1Division of Cancer Epidemiology
and Genetics, National Cancer Institute,
National Institutes of Health,
Bethesda, MD;
2Melanoma Program,
Abramson Cancer Center, University of
Pennsylvania School of Medicine, Philadelphia,
PA;
3Melanoma Clinic and
Department of Epidemiology and
Biostatistics, University of California
San Francisco, San Francisco, CA; and
4Dermatology Service, Memorial Sloan-
Kettering Cancer Center, New York, NY.
ABSTRACT
Purpose
We developed a model to estimate the 5-year absolute risk of melanoma to efficiently identify individuals at increased risk of melanoma for potential interventions.
Patients and Methods
We used data from a case-control study with 718 non-Hispanic white patients with invasive cutaneous melanoma from melanoma clinics in Philadelphia, PA and San Francisco, CA; matched controls were 945 patients from outpatient clinics with similar catchment areas. All participants underwent extensive interviews and skin examinations. We selected easily obtained clinical characteristics and responses to simple questions for study in order to develop sex-specific relative risk models. These models were combined with incidence and mortality rates by United States geographic areas to develop estimates of the absolute risk of developing melanoma within 5 years.
Results
Relative risk models yielded an attributable risk of 86% for men and 89% for women, using at most seven variables. Attributable risks did not vary by age, ultraviolet B flux or hours outdoors. The absolute individual risks varied widely, depending on age, other host characteristics, and geographic area. Individual absolute risk can be estimated using a program available online.
Conclusion
Our procedures allow for estimating the absolute risk of developing melanoma to assist in the identification of patients at high risk. Such high-risk individuals could undergo interventions including a complete skin examination, counseling to avoid sun exposures, regular self and professional surveillance, or participation in prevention trials. It is important to emphasize that these projections are not intended to identify current melanoma cases.
Among the white population, cutaneous melanoma is a problem of increasing clinical and public health importance. An estimated 62,190 new cases of cutaneous melanoma were diagnosed in the United States in 2006.[1] The age-adjusted incidence rate of cutaneous melanoma for 1997 to 2001 was 21.4 per 100,000 person-years[2] and has been rising rapidly for many years. Estimated 10-year survival rates for patients without evident metastases range from 88% for those patients with tumors <= 1.0 mm without ulceration to 32% for those patients with tumors larger than 4.0mm with ulceration.[3] Initially, melanomas evolve slowly and in a step-wise fashion. Patients whose primary lesions are detected and treated early have an excellent outcome: their 10-year metastasis-free survival rate is 91.8% to 99.5%.[4, 5]
In very high-risk individuals, screening and interventions have resulted in earlier-stage diagnoses.[6, 7] However, routine screening for melanoma is currently controversial.[8] Some groups, such as individuals with a strong family history[9] or previous melanoma,[2] have been appropriately targeted. Other high-risk individuals could be identified for either screening or interventions, including chemoprevention trials.[10] Prevention trials would require a large number of individuals; simple identification of potential participants would be very useful. There is broad agreement that primary care providers should play an important role in reducing mortality by identifying those patients at high risk for melanoma[7, 11, 12] and by developing and implementing effective prevention and early-detection tactics for them. Thus, primary care providers could use a pre-diction model to identify individuals who are at high absolute risk.
To identify patients at high risk, we developed a model to estimate the chance of developing a first primary melanoma over the next 5 years for a white man or woman with a given age between 20 and 70 years with specified risk factors. The risk factors for this model can be ascertained easily during a routine physical exam by a health care provider. They are based on at most two questions and an examination of only the skin of the back. We present a specific example, but a program to calculate estimated absolute risk for any combination of risk factors is available online (http://dceg.cancer.gov/melanomarisktool_prvw).
Study Subjects
In a case-control study,[13, 14] patients ages 20 to 79 years with histologically confirmed invasive cutaneous melanoma were those newly diagnosed from 1991 to 1992 at the University of Pennsylvania's Pigmented Lesion Clinic (Philadelphia, PA) and the University of California San Francisco's Melanoma Clinic (San Francisco, CA). Controls were from outpatient clinics with similar catchment areas and were frequency matched to case subjects by sex, age group, and study site. Those with initial dermatologic or psychiatric problems were excluded. The analysis was restricted to non-Hispanic white subjects because melanoma is rare in other ethnic groups. Of the 738 case subjects and 1,030 controls, 718 case subjects and 945 controls with a median age of 49 years were used in the relative-risk modeling.
As described previously,[13] trained interviewers administered a detailed questionnaire in person to each participant. Data included sunburn and suntan responses along with medical, occupation, residence, and outdoor exposure case histories. Each participant also had a complete skin examination during which participants' freckling pattern, skin color, solar damage, and mole and dysplastic nevi counts (small moles, >= 2 mm and < 5 mm; large moles, >= 5 mm) were recorded. Examiners (physicians and nurses) were uniformly trained and were retrained every 6 months by the same instructor.
Statistical Methods
Estimates of 5-year melanoma absolute risk were developed using the methods of Gail et al[15] to combine relative risk models based on data from the case-control study[13, 14] with US rates for melanoma incidence and mortality from other causes for the years 1992 to 2001 derived from the Surveillance, Epidemiology, and End Results Program (SEER).[2] Our projections were not intended for those participants with a prior melanoma or nonmelanoma skin cancer or for those with a first-degree relative with melanoma, as such individuals are recognized as being high risk[2, 7, 9] and standard care would include surveillance. For details of the statistical methods, see Appendix.
The components of the final absolute risk model are presented with an illustrative example. The final model is a combination of the relative risk associated with individual phenotype and risk factors as estimated from the case-control study, the population risk as measured by SEER, and the competing hazard of mortality from other causes.
Relative Risk Models
The factors considered for inclusion in the models were required to be quickly, easily, and accurately identified during routine healthcare evaluations. Factors requiring the provider to have specialized diagnostic skills, ask detailed questions, or carry out more extensive patient examinations were specifically not considered. Factors considered for inclusion in the model from the questionnaire included selfreported eye color, hair color, complexion, sunburn type, tan type, blistering sunburn as a child, blistering sunburn ever, and family history of melanoma. Factors considered from the physical examination included skin phenotype, eye, and hair color. Moles, freckling, and solar damage were evaluated for the back only. This is because the back and shoulders are commonly and readily examined at an office visit, the evaluation of moles, freckling, or solar damage on the back is easier than examination of chronically exposed areas such as the face, and the numbers of nevi on the back are highly correlated with nevi in the total body count.
Moles, freckling, and solar damage were evaluated for the back as follows: small nevi and those >=5mm in diameter were counted; the degree of freckling on the back and solar damage on the shoulders were ascertained with reference to standard photographs (see Fig 1 or online at (http://dceg.cancer.gov/melanomarisktool_prvw). Many important available factors from the questionnaire were not considered because of the relative complexity of obtaining the information in the primary care setting.
The variables were evaluated using stepwise logistic regression, conditional on the age and location matching in the case-control study. Estimated relative risk and confidence intervals for the final relative risk models are summarized in Table 1. These are the components that alter the individual's risk from the baseline population risk of a person of the same age, sex, and geographic area. For all risk factors, the estimated relative risks from age groups 20 to 49 years and >=50 years were consistent with the CIs obtained using the full data. Relative risks for a combination of risk factors can be obtained by multiplying the component relative risks.
Example: Determination of Risk Factors by the Primary Care Provider
Assessment of risk factors requires asking two questions, depending on the patient's sex, and an examination of only the back. Table 2 lists the specific questions to be asked and the phenotypes to record. As noted, the extent of freckling and of solar damage are graded by comparison with standard images (Fig 1).
The estimated relative risk can be calculated for an individual with a specified profile of risk characteristics. For example, consider a 40-year-old man with three large nevi and eight smaller nevi on the back and severe solar damage on his shoulders. This individual's relative risk is obtained from Table 1 as the product of the relative risks for the individual risk factors, r = 2.412 * 1.935 * 2.803 = 13.08. The specific values used to compute this example are boldfaced in Tables 1 and 3.
Incidence and Mortality Rates
Age-specific melanoma incidence rates were available for the 10 continental SEER locations for the years 1992 to 2001. Generally available SEER incidence rates are averages of different geographic regions. Because melanoma incidence rates are higher for areas of high ultraviolet B radiation (UVB) flux, the SEER locations were categorized into three regions: south (Atlanta, GA; Los Angeles, CA; New Mexico), central (San Francisco-Oakland, CA; San Jose-Monterey, CA; Utah) and north (Seattle, WA; Connecticut; Detroit, MI; Iowa).
To obtain estimates of melanoma incidence rates by region, the logarithmically transformed 5-year age-specific rates for men and women ages 20 to 74 years were regressed on age, the logarithm of age, and the logarithm of estimated UVB intensity (Fig 2 and Table 3). Five-year age-specific mortality rates for all causes except melanoma were also available for the years 1992 to 2001, for all continental states (Table 3).[2]
These estimates are necessary for adjusting for the age, likelihood of dying of other causes, and geographic area of the person at risk.
Predicting Absolute Risk of Melanoma
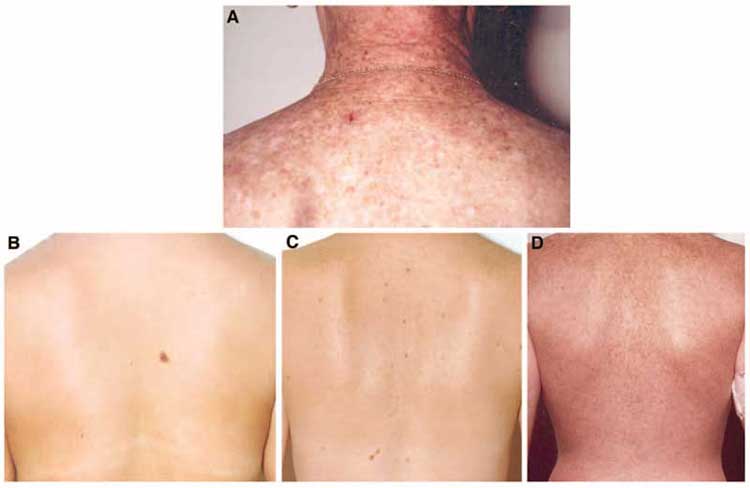
Fig 1. (A) Standard photograph for grading severe solar damage on the shoulders. Standard photographs for grading freckling of the back: (B) mild freckling of the upper back,
one large nevus, four small nevi; (C) moderate freckling of the upper back, four large nevi, 12 small nevi; (D) extensive freckling of the upper and lower back, no nevi.
Example: Estimation of the Baseline Melanoma Incidence for Those Without Risk Factors
The baseline melanoma incidence rates are the rates for those individuals without any risk factors. The current residence can be associated with a geographic region to determine the appropriate incidence rates and the baseline hazard for melanoma. Specifically, the baseline melanoma rates were estimated using melanoma incidence rates for the population multiplied by one minus the attributable risk that was in turn derived from the relative risk model. The attributable risks changed little with age, residence, or outdoor exposure, so the overall estimates were used.
In the case described in Example: Determination of Risk Factors by the Primary Care Provider, suppose that the 40-yearold man lived in the central region of the United States. According to Table 3, the melanoma incidence rate for men 40 to 44 years old is 23.50/100,000, and according to Table 1, the attributable risk for men is 0.856, so that the baseline hazard for men 40 to 44 years old is obtained as h1 =0.0002350(1 - 0.856) =.00003384. Again, the specific values used to compute this example are boldfaced in Tables 1 and 3.
Example: Estimation of the Individual 5-Year Absolute Risk for Melanoma
We have shown that for an individual with a specified profile of risk characteristics, the estimated relative risk can be calculated, and the current residence associated with a geographic region can be used to determine the appropriate baseline incidence rates. Using equation A1 in the Appendix, these estimates together with mortality rates can be combined to provide an estimate of the individual's absolute risk for melanoma during the next 5 years. These estimates can be used to show that although melanoma risks vary greatly by age and region, other individual risk factors play an important role in determining the projected 5-year risk for melanoma (see Appendix).
Consider again the 40-year-old man in the example. The man's estimated relative risk using Table 1 was r = 13.08. Using the melanoma incidence rate for men 40 to 44 years old from Table 3 and the attributable risk for men, the baseline hazard obtained was h1 =0.00003384. Also from Table 3, mortality rate for men 40 to 44 years old from causes other than melanoma is h2 =283.55/100,000. The estimating equation reduces to
P(a,r) ={h1 r/(h1r + h2)}[1 - exp{- 5(h1r + h2)}](1)
with a =  = 40 and + 1 = 45. Substituting for r, h1i, and h2i in equation 1 gives P(40, 13.08) =0.00220 or 0.22%.
= 40 and + 1 = 45. Substituting for r, h1i, and h2i in equation 1 gives P(40, 13.08) =0.00220 or 0.22%.
| Table 1. Summary of Final Relative Risk Model for Melanoma Among Men
and Women Without a Previous Skin Cancer or First-Degree Family Member With Melanoma |
| | Estimate of Relative Risk |
95% Cl |
| Men |
| Any blistering burn* |
1.437 |
1.023 to 2.019 |
| Light complexion* |
1.767 |
1.295 to 2.411 |
| >=2 large moles† |
2.412 |
1.704 to 3.415 |
| 7-16 small moles† |
1.935 |
1.337 to 2.799 |
| >=17 small moles† |
4.630 |
3.061 to 7.002 |
| >mild freckling† | 1.830 | 1.332 to 2.514 |
| Very severe solar damage‡ | 2.803 | 1.359 to 5.782 |
| Attributable risk | 0.856 | 0.797 to 0.915 |
| Women |
| Light complexion* | 1.802 |
1.238 to 2.625 |
| Light or no tan* | 1.926 |
1.325 to 2.801 |
| 5-11 small moles† |
2.512 |
1.667 to 3.788 |
| >=12 small moles† | 5.154 |
3.316 to 8.012 |
| Mild freckling† | 2.174 |
1.231 to 3.840 |
| More extensive freckling† | 3.856 |
2.124 to 7.000 |
| Attributable risk | 0.894 |
0.843 to 0.945 |
NOTE. Boldfaced values are used in text example.
*Factors were ascertained by self-report.
†Factors were ascertained by examination of the back.
‡Factors were ascertained by examination of the shoulders. |
The provider enters the patient's age, sex, and data regarding response to sun exposure, phenotype, and geographic area into the program (available online at (http://dceg.cancer.gov/melanomarisktool_prvw), which incorporates average annual UVB flux for the continental states.[16]
Estimated Performance of the Predictor
We compared the performance of two approaches to indentify high-risk individuals. The first approach was suggested by studies showing that melanoma detection efforts may be more cost-effective when focused on the population that is older than 50 years.[12, 17] The approach, then, is based simply on age: all participants aged 50 years or older are identified as high risk. The second approach is based somewhat arbitrarily on the individual 5-year absolute risk estimates for melanoma from our models: all men and women with P(a,r) of at least 0.15% are identified as high risk.
| Table 2. Determination of Risk Factors Required to Estimate the Probability
of Developing Melanoma Over the Next 5 Years |
| General examination |
|
For all patients
"Do you have a light, medium, or dark complexion?"
For men only
"Did you ever get a blistering sunburn?"
For women only
"After repeated and prolonged exposure to sunlight, at the age you are now, would your skin become very brown and deeply tanned, moderately tanned, lightly tanned, or not tan at all?" |
| Examination of the back and shoulders |
|
For all patients
Count the number of small moles on the back (up to 12 for women
and up to 17 for men) and
Determine the extent of freckling on the upper and lower back by
comparison with standard photographs
For men only
"Determine whether there are >= 2 large moles on the back and
Determine whether there is severe solar damage on the shoulders by
comparison with standard photographs |
| NOTE. All patients were administered a full skin examination including an
examination of the back and shoulders. |
For a computational comparison of the two approaches, we regarded the average population of the 10 continental SEER locations, using the individuals aged 20 to 69 years as a cohort (14,244,767 individuals). We assumed that after 5 years everyone in the cohort would have had a physical exam and been evaluated for risk of melanoma.
Weighting the case-control data by age and sex using SEER populations, we estimated that compared with identification based on age, the approach based on P(a,r) would identify 22% fewer men and 18% fewer women in the general population as being high risk. If the healthcare provider must work with each high-risk individual to develop effective prevention and early detection tactics, this difference suggests that identification of high risk based on P(a,r) would require less total time and therefore reduced total cost.
The number of melanoma cases in this hypothetical cohort diagnosed in the sixth year was taken to be the SEER average, 3,496 men and women. During the 5 years before diagnosis, all of these individuals would have received a physical exam and been evaluated for risk of melanoma. Those individuals identified as at high risk for melanoma would have received assistance in developing effective prevention and early-detection tactics before the sixth year and their diagnosis. Again, using the SEER populations for weighting, we estimated that 32% more men and 31% more women would have been identified as high risk during the 5 years before their diagnosis of melanoma, if the identification approach based on P(a,r) were used. These calculations therefore suggest that the identification of high-risk individuals based on P(a,r) will be the more effective approach to provide assistance in melanoma prevention and detection.
Melanoma has many features that make it a good target for early detection. It is increasingly common, has biologically early visually distinctive lesions that require noninvasive inspection for provisional identification, and is definitively diagnosed and cured in its early stages with simple nonmorbid inexpensive surgery. Routine screening of the general population for melanoma using complete skin exams is theoretically possible, but would be very costly because of the large number of examinations required and would be inefficient because of the many negative examinations. Targeting high-risk individuals would improve efficiencies and help select the appropriate people for interventions. These interventions could include complete skin examination, counseling and education to avoid sun exposure, regular self-examination, and professional surveillance. Interventions in high-risk individuals may lead to the detection of early-stage curable disease or to a decrease in patients' risk of developing melanoma.[10, 18, 19]
| Table 3. Estimated Rates per 100,000 Person-Years for Incidence of Invasive Melanoma and Mortality Without Melanoma for the Years 1992-2001 by Age Group and Region Based on Continental SEER Locations |
| | Men | Women |
| | Melanoma Incidence | Mortality Without Melanoma | Melanoma Incidence | Mortality Without Melanoma |
| Age Group (years) | South | Central | North | Continental | South | Central | North | Continental |
| 20-24 |
4.49 |
4.12 |
3.6 |
122.86 |
9.35 |
8.84 |
8.12 |
43.13 |
| 25-29 |
7.85 |
7.19 |
6.3 |
127.25 |
13.18 |
12.47 |
11.45 |
49.40 |
| 30-34 |
12.42 |
11.38 |
9.96 |
161.32 |
17.16 |
16.23 |
14.91 |
66.13 |
| 35-39 |
18.32 |
16.79 |
14.7 |
209.35 |
21.12 |
19.98 |
18.35 |
96.86 |
| 40-44 |
25.64 |
23.50 |
20.57 |
283.55 |
24.93 |
23.58 |
21.66 |
142.86 |
| 45-49 |
34.46 |
31.58 |
27.65 |
404.72 |
28.48 |
26.94 |
24.75 |
221.75 |
| 50-54 |
44.84 |
41.10 |
35.97 |
608.14 |
31.71 |
30.00 |
27.55 |
359.32 |
| 55-59 |
56.82 |
52.08 |
45.59 |
979.82 |
34.57 |
32.70 |
30.04 |
588.77 |
| 60-64 |
70.43 |
64.55 |
56.51 |
1,600.96 |
37.03 |
35.02 |
32.17 |
955.41 |
| 65-69 |
85.70 |
78.55 |
68.76 |
2,490.23 |
39.08 |
36.96 |
33.95 |
1,478.73 |
| 70-74 |
102.64 |
94.07 |
82.35 |
3,824.02 |
40.72 |
38.51 |
35.38 |
2,316.32 |
|
NOTE. Boldfaced values are used in text example.
Abbreviation: SEER, Surveillance, Epidemiology, and End Results program. |
|
We have developed a model to project individual 5-year absolute risks of developing melanoma in the presence of competing risks that has the potential to identify high-risk individuals by focusing on information that a healthcare provider can readily obtain during a routine office visit or comparable encounter. To foster generalizability and portability of the proposed model, we emphasized the use of risk factors that take a minimum of time to obtain and do not require the patient to completely disrobe. Developing different models for men and women increased the predictive ability as it allowed for the inclusion of different predictors and the different impact of predictive variables that may have different distributions among the sexes.
Overall, when compared with the identification of high risk using age only, the approach based on estimated absolute risk would identify fewer individuals in the general population, yet identify more individuals among the melanoma cases in the follow-up year. If the former is regarded as a measure of "cost" and the latter as a measure of "effectiveness," then using estimated absolute risk is projected to cost less and be more effective. The referral values for estimated absolute risk were arbitrary. Increasing the referral values will reduce the cost but will also reduce the effectiveness. Decreasing the referral values will increase the effectiveness but will also increase the cost.
Although the absence of several known melanoma risk factors may be seen as a potential limitation of our model, this is likely of little impact, as many of the excluded factors are highly correlated with those included in the model. Pregnancy provided important improvement in the model for women but was omitted since its role as a risk factor is not yet clear.[20] Pregnancy may be correlated with other risk factors that were not considered, such as hormones or behavior. Nevertheless, the phenotypic factors in the model (eg, freckling and nevi) are powerful summations of both host susceptibility and total life sun/UV exposure. The stable high attributable risks demonstrate that these factors capture much of melanoma risk. Risk factors for melanoma not explicitly included in the models, such as presence and number of dysplastic nevi,[13] may be accounted for in part by large nevi.
A limitation of the model is that it was based on data from one case-control study, though it was a large one with bicoastal representation. Validation of the relative risk in other case-control data sets is difficult because clinical skin exams with variables similar to those in our models have not been part of any other large melanoma case control study. We believe that the potential utility of the model will encourage its testing by other investigators in other populations. We note a recently published report based on a cohort of employees in the healthcare professions.[21] Although the study is not population based and did not include a professional skin exam, it is reassuring that risk factors identified were comparable to those determined here (age, sex, sunburn history, and nevus number, together with hair color).
We have estimated the area under the receiver operating characteristics (ROC) curve for the model. Using the population sizes of the continental SEER locations along with risk estimates from our case control data, the false-positive and true-positive rates were estimated for different possible cut points. The estimated area under the ROC curves ranged from 0.70 for women aged >= 50 years to 0.80 for men aged 20 to 49 years. This compares favorably with other risk models with which we are familiar, such as the Gail model for breast cancer risk.
Fig 2.Estimated melanoma incidence rates by 5-year intervals of age and by region of the United States.
The model has a number of strengths. As a predictive model with potential utility in general practice, it uses readily obtainable variables. It is flexible and can easily be extended to predict over longer time intervals, or provide lifetime risk estimates. The model is probably widely generalizable. It is important that the relative risk and associated attributable risk estimates were found to be very stable over a wide range of UVB intensity levels and outdoor exposure rates. This indicates that these or related models can be used with appropriate incidence and mortality rates to develop absolute risk estimates, not just for the United States, but for other regions of the world with comparable UVB intensity levels and similar melanoma risk factors.
References
- Jemal A, Siegal R, Ward E, et al: Cancer Statistics, 2006. CA Cancer J Clin 56:106-130, 2006
- Ries LAG, Eisner MP, Kosary CL, et al (eds): SEER Cancer Statistics Review, 1975-2001. Bethesda, MD, National Cancer Institute, 2004 http://seer.cancer.gov/csr/1975_2001/
- Balch CM, Buzaid AC, Soong SJ, et al: Final version of the American Joint Committee on Cancer Staging System for Cutaneous Melanoma. J Clin Oncol 19:3635-3648, 2001
- Gimotty PA, Guerry D, Ming ME, et al: Thin primary cutaneous melanoma: A prognostic tree for 10-year metastasis is more accurate than American Joint Committee on Cancer Staging. J Clin Oncol 22:3668-3676, 2004
- Leiter U, Buettner PG, Eigentler TK, et al: Prognostic factors of thin cutaneous melanoma: An analysis of the central malignant registry of the German Dermatological Society. J Clin Oncol 22: 3660-3667, 2004
- Masri GD, Clark WH, Guerry D, et al: Screening and surveillance of patients at high risk for malignant melanoma result in detection of earlier disease. J Am Acad Dermatol 22:1042-1048, 1990
- MacKie RM, McHenry P, Hole D: Accelerated detection with prospective surveillance for cutaneous malignant in high-risk groups. Lancet 341:1618-1620, 1993
- Geller AC: Screening for melanoma. Dermatol Clin 20:629-640, 2002
- Kefford RF, Newton Bishop JA, Bergman W, et al: Counseling and DNA testing for individuals perceived to be genetically
predisposed to melanoma: A consensus statement of the Melanoma Genetics Consortium. J Clin Oncol 17:3245-3251,1999
- Demierre M-F, Sondak VK: Cutaneous melanoma: Pathogenesis and rationale for chemoprevention. Crit Rev Oncol Hematol 53:225-239, 2005
- Edman RL, Klaus SN: Is routine screening for melanoma a benign practice? JAMA 284:883-885, 2000
- Weinstock MA: Early detection of melanoma. JAMA 284:886-889, 2000
- Tucker MA, Halpern A, Holly EA, et al: Clinically recognized dysplastic nevi, a central risk factor for cutaneous melanoma. JAMA 277:1439-1444, 1997
- Fears TR, Bird CC, Gail MH, et al: Average UVB intensity and time outdoors predict melanoma risk. Cancer Res 62:3992-3996, 2002
- Gail MH, Brinton LA, Byar DP, et al: Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J Natl Cancer Inst 81:1879-1886, 1989
- Scotto J, Fears TR, Fraumeni JF Jr: Solar radiation, in Shottenfeld D, Fraumeni JF Jr (eds): Cancer Epidemiology and Prevention, Second Edition. New York, NY, Oxford University Press, 1996, pp 355-372
- Girgis A, Clarke P, Burton RC, et al: Screening for melanoma by primary health care physicians: A cost -effectiveness analysis. J Med Screen 3:47-53, 1996
- Tucker MA, Fraser MC, Goldstein AM, et al: Risk of melanoma and other cancers in melanomaprone families. J Invest Dermatol 100:350S-355S, 1993
- Kang S, Barnhill RL, Mihm MC, et al: Melanoma risk in individuals with clinically atypical nevi. Arch Dermatol 130:999-1001, 1994
- Wiggins CL, Berwick M, Bishop JA: Malignant melanoma in pregnancy. Obstet Gynecol Clin North Am 32:559-568, 2005
- Cho E, Rosner BA, Feskanich D, et al: Risk factors and individual probabilities of melanoma for whites. J Clin Oncol 23:2669-2675, 2005
- Bruzzi P, Green SB, Byar DP, et al: Estimating the population attributable risk for multiple risk factors using case-control data. Am J Epidemiol 122:904-914, 1985
- Graubard BA, Fears TR: A simple method for obtaining standard errors and confidence intervals for attributable risk from simple random samples and complex samples. Biometrics 61:847-855, 2005
- SAS Institute Inc: SAS Technical Report P-217 SAS/STAT Software: The PHREG Procedure. Cary, NC: SAS Institute Inc, 1991
Acknowledgment
We wish to acknowledge Susan Devesa, PhD, for assistance in developing data for the analysis and Barry Graubard, PhD, for valuable discussions and important suggestions.
Methods to develop risk projections. For an individual of age
awith
<=
a <

for some

= 20,25,30,... and relative risk
r, the estimated probability that the individual will develop melanoma by age
a+5 is
where the h1i are baseline hazard rates for melanoma and the h2i are mortality rates from causes other than melanoma.
The baseline hazard rate is the hazard rate for those individuals without any of the risk factors. The age-specific baseline hazard rates can be estimated by multiplying the age-specific incidence rate by one minus the estimate of the appropriate attributable risk (AR) derived from the full relative risk model. Specifically, the relative risk models were used to estimate the attributable risks,
where m is the number of cases, the summation is over the case data, and rj is the estimated relative risk for the jth case.[22] If h1i*are the
age-specific rates for melanoma incidence, then the baseline hazard for melanoma is hli = h1i*(1 - AR) when AR varies little with age.
Computations indicated that the estimates of incidence and mortality rates were very stable; thus for CI calculations we developed robust
estimates of the variability of the 5-year risk projections based only on the sampling variability in the case-control data.[23]
The Relative Risk Estimates
We developed separate relative risk models for males and females from the case-control study[13, 14] using conditional logistic regression to estimate odds ratios for melanoma.[24] All models included terms for previous skin cancer or first-degree family history of melanoma, so that the baseline hazard referred to those without previous skin cancer or a family history of melanoma.
Attributable Risk Assumption
The baseline hazard rate was estimated using melanoma incidence rates and one minus the attributable risk that was in turn derived from the relative risk model. As the ARs for our models are near one, it is particularly important that the ARs are stable since a small change in AR has a large impact on the baseline hazard rate.
The incidence for melanoma increases with age so it was necessary to ensure that attributable risk does not vary with age. The study cases were used to estimate the attributable risk by tertile of age based on the model. The attributable risks varied only slightly, from 0.85 to 0.87 for men and from 0.85 to 0.92 for women, within the 95% CIs for attributable risk in Table 2.
Incidence rates also vary with a location’s UVBflux and the hours spent outdoors by its population. To make predictions for locations other than those in the case-control study, we investigated whether attributable risks also varied with exposure variables. In the questionnaire, we collected information on all places where study participants lived for more than 6 months. Based on ground level UVB measurements, each residence location was assigned an estimate of the total UVB flux at the location. For each individual, dividing the total lifetime UVB flux by age provided an estimate of the mean annual exposure intensity.[14] The respondents were grouped by tertile of average annual exposure intensity and attributable risk was found to vary little with exposure intensity (men, 0.84 to 0.87; women, 0.88 to 0.91). Adult hours outdoors were also calculated and the respondents were grouped by tertile of average hours outdoors per day as an adult. Attributable risk varied little with outdoor exposure rates (men, 0.83 to 0.87; women, 0.88 to 0.90).
Thus, the attributable risk factor changed little with age, UVB intensity of residence locations, or outdoor exposure rates. The same attributable risks are likely to apply for all the SEER regions as long as the prevalence of risk factors does not vary. The overall estimates of attributable risk were therefore used to estimate the baseline hazard rates for each of the three SEER regions.
Estimation of Individual 5-Year Absolute Risk of Melanoma
Appendix Tables A1, A2, andA3contain examples of the estimates for the probability (%) of developing melanoma within 5 years for individuals with different sets of risk factors. Among the men, patient 1 has a self-reported light complexion, no burns, and no moles or freckling on his back; patient 2 has medium complexion, no burns, and has seven small nevi and very extensive back freckling; and patient 3 has dark complexion, had a blistering burn, and has three large nevi and nine small nevi on his back. Among the women, patient 4 has light complexion, can develop a moderate tan, and has mild freckling on her back; patient 5 has light complexion, does not tan, has eight small nevi, and no freckling on her back; and patient 6 has light complexion, does not tan,
has five small nevi, and mild freckling on her back.
Assuming that the individuals live in the central region of the United States, risk estimates for five initial ages (30, 40, 50, 60, and 70 years) are given in Appendix Table A1. Probability estimates increase with initial age for each individual, just as the incidence rates increase with age. It is evident that risk factors for melanoma other than age play an important role in determining estimated risk, for example, among the women, patient 6 is more likely to develop melanoma at age 40 than patient 4 or patient 5 at any age. Assuming that the individuals are 60 years old, Appendix Table A2 provides the estimates of the risk for developing melanoma within 5 years by region. Probability estimates are lower for the more northern latitudes. Additional risk factors again play a significant role in determining estimated risk, eg, among the men the estimated risk for patient 3 in the north region of the United States is greater than that of patient 2
in the southern region. Melanoma incidence rates vary greatly by age and region, but other individual risk factors play an important role in determining the projected 5-year risk for melanoma.
Appendix Table A3 gives results for the six individuals at age 60 years who live in the central region of the United States. Confidence intervals are nearly symmetric for these probability estimates and half the interval width is less than 50% of the risk projection.
| Table A1.Projected Probability (%) of Developing Malignant Melanoma Within 5 Years for Six Patients Residing in the Central Region of the United States, by Five
Initial Ages |
| | Projected Probability (%) by Initial Age |
| Patient No. | Estimated Relative Risk | 30 Years | 40 Years | 50 Years | 60 Years | 70 Years |
Men |
| 1* |
1.8 |
0.01 |
0.03 |
0.05 |
0.08 |
0.11 |
| 2† |
3.5 |
0.03 |
0.06 |
0.10 |
0.16 |
0.22 |
| 3‡ |
6.7 |
0.05 |
0.11 |
0.20 |
0.30 |
0.41 |
Women |
| 4§ |
4 |
0.03 |
0.05 |
0.06 |
0.07 |
0.08 |
| 5|| |
8.8 |
0.07 |
0.11 |
0.14 |
0.16 |
0.17 |
| 6# |
19.2 |
0.16 |
0.24 |
0.30 |
0.34 |
0.36 |
|
|
*Patient 1: light complexion, no burns, no moles, and no freckling.
†Patient 2: medium complexion, no burns, seven small moles on his back, and very extensive back freckling.
‡Patient 3: dark complexion, a blistering burn at age 22 years, and has three large moles and nine small moles on his back.
§Patient 4: light complexion, can develop a moderate tan, and mild freckling on her back.
||Patient 5: light complexion, does not tan, has eight small moles on her back, and no freckling on her back.
#Patient 6: light complexion, does not tan, has five small moles on her back, and mild freckling on her back.
|
|
| Table A2.Projected Probability (%) of Developing Malignant Melanoma
Within 5 Years for Six Patients Who Are 60 Years Old, by Three US Regions |
| |
Projected Probability (%) by Region of Residence |
| Patient No. | Estimated Relative Risk |
North |
Centeral |
South |
Men |
| 1 |
1.8 |
0.07 |
0.08 |
0.09 |
| 2 |
3.5 |
0.14 |
0.16 |
0.17 |
| 3 |
6.7 |
0.26 |
0.30 |
0.33 |
Women |
| 4 |
4.0 |
0.07 |
0.07 |
0.08 |
| 5 |
8.8 |
0.15 |
0.16 |
0.17 |
| 6 |
19.2 |
0.32 |
0.34 |
0.36 |
|
|
| Table A3.Projected Probability (%) and 95% CI of Developing Malignant
Melanoma for Six Patients Who Are 60 Years Old and Live in the Central Region of the US |
| Patient No. |
Estimated Relative Risk |
Estimated
Absolute Risk (%) |
95% CI |
Men |
| 1 |
1.8 |
0.08 |
0.05 to 0.11 |
| 2 |
3.5 |
0.16 |
0.09 to 0.22 |
| 3 |
6.7 |
0.30 |
0.17 to 0.43 |
Women |
| 4 |
4.0 |
0.07 |
0.04 to 0.10 |
| 5 |
8.8 |
0.16 |
0.08 to 0.23 |
| 6 |
19.2 |
0 .34 |
0.18 to 0.51 |
|
|
Authors' Disclosures of Potential Conflicts of Interest
The authors indicated no potential conflicts of interest.
Author Contributions
Conception and design: Thomas R. Fears, DuPont Guerry IV, Ruth M. Pfeiffer, Richard W. Sagebiel, David E. Elder, Allan C. Halpern, Elizabeth A. Holly,
Patricia Hartge, Margaret A. Tucker
Administrative support: Allan C. Halpern, Elizabeth A. Holly, Margaret A. Tucker
Provision of study materials or patients: DuPont Gerry IV, Richard W. Sagebiel, David E. Elder, Allan C. Halpern, Elizabeth A. Holly
Collection and assembly of data: Thomas R. Fears, DuPont Guerry IV, Ruth M. Pfeiffer, Richard W. Sagebiel, David E. Elder, Allan C. Halpern, Elizabeth
A. Holly, Patricia Hartge, Margaret A. Tucker
Data analysis and interpretation: Thomas R. Fears, DuPont Guerry IV, Ruth M. Pfeiffer, Margaret A. Tucker
Manuscript writing: Thomas R. Fears, DuPont Guerry IV, Ruth M. Pfeiffer, Elizabeth A. Holly, Patricia Hartge, Margaret A. Tucker
Supported by the Intramural Research
Program of the National Institutes of
Health and the National Cancer Institute.
Address reprint requests to Thomas R.
Fears, PhD, National Cancer Institute;
Executive Plaza S, Room 8040,
Bethesda, MD 20892; e-mail: fearst@
epndce.nci.nih.gov.