|
|
 |
 Printer-friendly
format Printer-friendly
format
 Download PDF version
Download PDF version
 Email this page
Email this page
Obesity Policy and the Law of Unintended Consequences
Fred
Kuchler
Elise Golan
Jayachandran N. Variyam
Stephen R. Crutchfield
 Americans
are increasingly overweight, with the number of obese adults and
overweight children doubling between the late 1970s and early 2000s.
Several studies of the health consequences of Americans’ weight
gain indicate that health care costs and the number of premature
deaths associated with obesity and overweight are high. A recent
(lower) estimate of the number of premature deaths published in
the Journal of the American Medical Association reveals
the uncertainty researchers face in associating weight status with
mortality. Of course, scientific uncertainty does not mute demands
for public action. Americans
are increasingly overweight, with the number of obese adults and
overweight children doubling between the late 1970s and early 2000s.
Several studies of the health consequences of Americans’ weight
gain indicate that health care costs and the number of premature
deaths associated with obesity and overweight are high. A recent
(lower) estimate of the number of premature deaths published in
the Journal of the American Medical Association reveals
the uncertainty researchers face in associating weight status with
mortality. Of course, scientific uncertainty does not mute demands
for public action.
Action to combat obesity and overweight could come in many forms
since many variables influence diet and lifestyle choices. While
economics tells us that prices and income shape choices, other factors
are important, too. Individuals choose foods based on taste, convenience,
family structure and traditions, age, health status, knowledge,
and lifestyle. Policy targeted at any of these factors could have
some success in reducing obesity and overweight. However, such success
is likely to be limited if all other factors remain unchanged. The
economic levers available to policymakers to create incentives for
individuals to alter diet and lifestyle choices affect only some
of the determinants of food choices.
The wide range of factors contributing to food choices is compounded
by the incredible variety of foods and consumption opportunities
available today—we make choices among thousands of food products,
choices about whether to eat at home or in a variety of restaurants,
and choices about lifestyles, such as diet quality and exercise.
As a result of nearly unlimited choice, public policy targeting
specific foods or lifestyle choices could have surprising unintended
consequences. ERS has examined some of the potential intended and
unintended consequences of three widely discussed obesity policies—nutrition
labels in restaurants, taxes on snack foods, and restrictions on
food advertising to children—with a focus on the likely effect
of each program on producer and consumer incentives and on health
outcomes. In every case, the unintended effects could dampen the
policy’s success in reducing overweight and obesity.
Nutrition Labeling at Restaurants
The 1994 National Labeling and Education Act (NLEA) requires manufacturers
to include a nutrition information panel on the label of almost
all packaged foods, but it does not require any similar disclosure
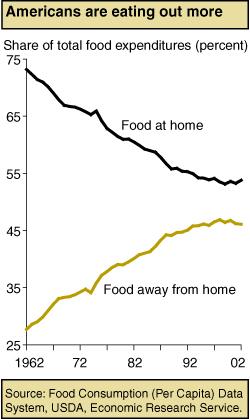
for foods purchased at restaurants—food-away-from-home (FAFH).
The lack of nutrition information for FAFH means that if consumers
misjudge the nutrient content of meals eaten out, they may inadvertently
overconsume some nutrients and underconsume others. An ERS study
showed that FAFH typically contained more of the nutrients overconsumed
(fat and saturated fat) and less of the nutrients underconsumed
(calcium, fiber, and iron) by Americans. Because FAFH commands a
large and increasing share of total food expenditures, nutrition
choices at FAFH could have a large effect on overall diet quality.
If consumers choose high-fat or high-calorie foods because they
lack FAFH nutrition information, then mandatory FAFH labeling could
potentially lead to improvements in consumers’ food choices
and health. However, lack of information may not be the reason for
poor nutritional FAFH choices, either because the industry supplies
enough information or consumers deduce the information (see “Is
There Evidence That Obesity and Overweight Are the Result of Market
Failure?”). In such cases, making standardized nutrition
labels mandatory for major sources of FAFH such as fast food and
chain restaurants will not improve public health.
 Recent
consumer choice studies suggest that the effect of nutritional information
on diet in FAFH settings may be modest. For example, a Pennsylvania
State University study of food intake among normal-weight women
found that explaining the concept of energy density (amount of calories
per gram of food) and providing nutrition information on labels
during meals in a laboratory setting had no impact on subjects’
energy intakes. A restaurant study in England found that providing
nutrition information had no effect on overall energy and fat intake
of patrons. In fact, the presence of “lower fat” information
was associated with fewer restaurant patrons’ selecting the
target dish. Another study in an Army cafeteria found no significant
difference between sales before and after nutrition labeling for
either average “healthy” (labeled, containing less than
15 grams of fat and 100 milligrams of cholesterol per serving) entrée
sales or the proportion of healthy entrée to total entrée
sales. Recent
consumer choice studies suggest that the effect of nutritional information
on diet in FAFH settings may be modest. For example, a Pennsylvania
State University study of food intake among normal-weight women
found that explaining the concept of energy density (amount of calories
per gram of food) and providing nutrition information on labels
during meals in a laboratory setting had no impact on subjects’
energy intakes. A restaurant study in England found that providing
nutrition information had no effect on overall energy and fat intake
of patrons. In fact, the presence of “lower fat” information
was associated with fewer restaurant patrons’ selecting the
target dish. Another study in an Army cafeteria found no significant
difference between sales before and after nutrition labeling for
either average “healthy” (labeled, containing less than
15 grams of fat and 100 milligrams of cholesterol per serving) entrée
sales or the proportion of healthy entrée to total entrée
sales.
Even if consumers do not immediately respond to nutrition information,
mandatory labeling could still lead to improvements in consumer
health if the FAFH industry reacted by improving the nutritional
quality of foods sold at restaurants. For example, a FAFH labeling
policy requiring disclosure of the amount of calories, fat, sodium,
and cholesterol could induce restaurants’ selling products
high in these ingredients to reformulate their product rather than
risk losing sales to restaurants’ selling nutritionally superior
products. Such reformulation could alter the entire range of market
offerings and precipitate better nutritional outcomes for all consumers.
If consumers do not like these reformulations, restaurants will
abandon them for recipes with the taste and texture that consumers
prefer.
So far, the evidence on whether the 1994 act (NLEA) induced reformulation
of foods consumed at home is mixed. One study that examined the
snack cracker market found that the average fat content and the
average share of calories from fat per serving were significantly
lower in the post-NLEA period compared with the pre-NLEA period.
However, an ERS study that analyzed the nutritional quality of five
product categories before and after NLEA found little change.
Since taste is usually linked to higher fat, salt, and sugar content,
restaurateurs are likely to resist changing their recipes or formulating
new ones unless many consumers start making different food choices.
Or, restaurateurs could choose to reformulate away from one ingredient,
like saturated fat, and compensate for flavor changes by boosting
the sugar or salt content of the food. In this case, the overall
nutritional content of a restaurant meal may not improve. Meals
that are marginally lower in one or more attributes may not be much
healthier than the originals.
Restaurants could also respond to mandatory labeling by expanding
their menu options to include healthier choices, while still selling
or even promoting their less healthy options. In this way they could
satisfy their nutritionally conscientious customers without alienating
their customers who prefer higher fat or caloric foods. This strategy
could lead to unintended outcomes for nutrition information policy.
A study by Christine Moorman of Duke University showed that following
NLEA, food suppliers expanded price promotion of nutritionally poorer
brands while promotion of nutritionally better brands did not change
significantly between the two periods.
| Is
There Evidence That Obesity and Overweight Are the Result of
Market Failure? |
Without evidence that food markets are failing
to reflect consumer and societal preferences, food policy
to curtail overweight and obesity could cause more harm than
good. Three possible market failure scenarios are drawing
the media’s and policymakers’ attention.
Scenario 1: Producers are not
responsive to consumer demand and do not supply the types
of food desired by consumers.
A business strategy that disregards consumer preferences
is unlikely to succeed for long, particularly in today’s
food industry. Processing, storage, transportation, and communication
technology have enabled food manufacturers to both gauge and
satisfy the subtlest variations in consumer preferences.
The variety of food products (40,000 in the typical supermarket
in 2000) on grocery store shelves reflects the industry’s
ability to adapt to consumer preferences—even short-lived
or faddish ones. For example, at the height of the low-fat
movement in 1996, manufacturers introduced 3,434 new “low-fat”
or “nonfat” food products. In 2003, 700 “low-carb”
or “no-carb” products hit the market and in 2004,
3,431 such products followed. Competition to attract and keep
customers extends to the fast food and restaurant industries.
Large portions and high-fat foods are one way to draw customers.
“Healthy” foods such as salads, bunless burgers,
and heart-healthy menu options are another.
Competition also extends to low-income consumers. In urban
areas, Asian, Caribbean, Indian, and South American stores
offer indigenous foods and produce for their customers, many
of whom are low-income recent immigrants. Retailers are even
courting low-income consumers with the emergence of “WIC-only”
stores, exclusive to WIC participants. All in all, there is
little evidence that the U.S. food industry is unwilling or
unable to supply the types of foods that consumers desire.
Scenario 2: Consumers do not
have enough information to make informed choices and inadvertently
demand (and consume) diets high in calories.
The sheer volume of media coverage devoted to diet and weight
makes it difficult to believe that Americans are unaware of
the relationship between a healthful diet and obesity. In
fact, results from USDA’s Diet and Health Knowledge
Survey indicate that most U.S. consumers have basic nutrition
knowledge and that they can discriminate among foods on the
basis of fat, fiber, and cholesterol. Most are aware of health
problems related to certain nutrients.
One consumer information gap may involve perceptions of
appropriate weight. ERS researchers found that 41 percent
of individuals whom health professionals would classify as
overweight, but not obese, did not perceive themselves to
be overweight. Among individuals whom professionals would
classify as obese, 13 percent said that their weight is about
right or even too low. These misperceptions about healthy
weight may lead to misinformed consumption choices.
|
But the facts admit an alternative explanation: the available
information does not allow researchers to distinguish misinformed
weight perceptions from informed disagreement with public
health weight norms.
Another information gap may exist with respect to the nutritional
quality of food sold at restaurants. For example, though savvy
consumers may be able to infer that a dessert that does not
have a “heart healthy” logo has more cholesterol
or saturated fat than one with the logo, they cannot infer
any information about sugar or calorie content. Restaurants
offer foods high in fat and calories because these foods taste
good, and they are not anxious to advertise their nutrition
information for potentially skittish customers.
Do these limitations to nutrition disclosure at restaurants
hinder the ability of consumers to make informed decisions?
On the one hand, most consumers suspect that food served at
fast food restaurants is not the healthiest. A 2003 Gallup
Poll survey found that two-thirds of consumers thought that
most food sold at fast-food restaurants was not good for them.
On the other hand, consumers may not be able to precisely
gauge the nutritional content of restaurant foods. A 1996
survey conducted by New York University and the Center for
Science in the Public Interest found that even trained dietitians
underestimated the calorie content of five restaurant meals
by an average of 37 percent and the fat content by 49 percent.
Scenario 3: Consumers make
poor diet choices because they do not bear all the health
costs of their choices.
Health insurance, both private and public, may reduce consumers’
incentives to take all cost-justified health precautions (including
choosing a healthy diet) because it reduces the medical costs
paid directly by consumers. The fact that a large part of
the health care bill from overweight and obesity is eventually
footed by taxpayers, not private insurance providers, may
further misalign social and private costs. Economists have
estimated that Medicare and Medicaid pay for at least half
of obesity-attributable medical expenses. What would otherwise
be a matter of personal choice (and responsibility) becomes
a matter of concern for all taxpayers.
Of course, Americans’ rapid weight gain may have nothing
to do with market failure. It may be a rational response to
changing technology and prices. Technological change has created
a largely sedentary workforce, so workers have to exercise
more outside of work or reduce their caloric intake to maintain
weight. In addition, frozen microwavable meals and the like
have reduced the time cost of preparing meals, encouraging
consumption. Medical technology in the treatment of obesity-related
illnesses has also improved, turning some hopeless situations
into chronic illnesses and, from the perspective of the obese,
reducing the health costs of obesity. So, if consumers willingly
trade off increased adiposity for working indoors and spending
less time in the kitchen as well as for manageable weight-related
health problems, then markets are not failing.
|
A Tax on Snack Food
Another proposal to reduce obesity in the United States is a tax
on snack foods that are high in salt, added sugar, fat, and calories.
As consumers substitute healthier foods, their weight would fall
and their health would likely improve. (Some variations of this
proposal would use revenues raised from the tax to fund expanded
nutrition education programs.)
Selective taxation of particular foods is rare for the Federal
Government. Oleomargarine was taxed from 1886 until 1950, and during
two periods in the early part of the 20th century, the Federal Government
taxed soft drinks. Thus, a Federal snack food tax would be novel
from a fiscal perspective.
For those consumers who are not overweight and enjoy snack foods,
there are only costs associated with the tax. They would either
pay the tax on their favorite snack foods or choose a less satisfying
diet. Also, excise taxes on food tend to be regressive—the
burden of the tax would likely fall disproportionately on low-income
consumers, who spend more of their income on food than do middle-
or upper-income consumers.
The health benefits of the tax depend on how big an incentive
the tax is for consumers to avoid taxed foods and make better dietary
choices. Imposing the tax may not create a strong incentive for
consumers to make changes. First, to influence consumer choices,
the tax must be passed on to retail consumers. Sometimes manufacturers
absorb the entire tax, leaving retail prices and consumers’
behavior unchanged. If snack food companies operate in competitive
markets, the tax would be passed on to consumers because the companies
are paying competitive prices for their inputs and cannot push the
tax onto suppliers. When food suppliers have some ability to set
prices, the relation between taxes and retail prices is less direct.
| Salty snack
consumption and expenditures, 1999 |
|
Snacks
|
Share of households that purchased snacks (percent)
|
Average quantity purchased by households that did purchase
(pounds)
|
Per capita quantity purchased by households that did purchase
(pounds)
|
Household expenditure by households that did purchase
(dollars)
|
|
Potato chips
|
91.3
|
9.76
|
4.18
|
26.14
|
|
All chips
|
95.5
|
16.34
|
7.00
|
41.43
|
|
Other salty snacks
|
96.8
|
16.47
|
7.92
|
37.41
|
|
All salty snacks
|
99.2
|
31.81
|
14.47
|
76.39
|
|
Source: Tabulated by ERS from ACNielsen Homescan
panel, 1999.
|
Second, the tax base—the foods that are taxed—has to
be sufficiently broad to induce better choices. The tax base has
to include nutritionally equivalent foods, however infrequently
the latter are consumed. No benefits accrue if the tax simply induces
substituting one snack food for another—pork rinds for potato
chips. Many economists have studied demands for broad classes of
foods (for example, substitution among beef, pork, chicken, and
fish). How consumers might substitute away from particular types
of highly processed food is not yet clear. Tax proponents might
hope that consumers would substitute fruit and vegetables for snack
food.
Third, consumers would have to respond to changes in retail prices.
Looking at household expenditures in relation to income reveals
that consumers are unlikely to be greatly influenced by a tax. Household
expenditures on the entire class of salty snack foods (chips, nuts,
pretzels, cheese puffs, and popcorn) are for most households about
0.1 percent of annual income. Consumers are not likely to pay much
attention to changing retail prices for small expenditures. Other
goods, like homes and cars, will command much more of their interest
in prices.
ERS research estimating household demand for snack foods confirms
that salty snack foods are not very responsive to prices. Estimated
price responsiveness was similar in magnitude to that found in other
empirical research for cigarettes and alcoholic beverages. That
is, price increases may reduce purchases, but the reduction will
be much smaller than the tax-induced price increase. A relatively
small tax on snack food, say 1 percent, would have vanishingly small
impacts on dietary choices and thus negligible impacts on weight
or health. Since calculations were made under the assumption that
the entire tax would be passed forward, the actual impacts may be
smaller still.
Higher tax rates, say 30 percent, appear to influence consumer
food choices and weight so long as the tax base is broad. But such
results are tentative since the full range of consumer substitution
possibilities is difficult to model and may not correspond to previously
observed consumption patterns.
Curtail Food Advertising, Particularly to Children
Some health researchers and health policy activists have recommended
placing restrictions on food advertising. Some have proposed eliminating
ads for candy, soft drinks, fast foods, and sugared cereal aimed
at children. Proponents argue that these restrictions will help
improve children’s health. If children were no longer exposed
to frequently repeated advertisements, other foods could compete
for their attention. The effectiveness of a policy curtailing food
advertising to children depends on the extent to which food ads
alter children’s preferences for different food groups or
simply shift them from one hamburger chain (and one toy) to another.
If advertising is effective at forming children’s food tastes
and preferences, health benefits may accrue from minimizing children’s
exposure to advertising.
The food industry spends enormous amounts on advertising; however,
it is not clear to what extent these expenditures increase overall
calorie consumption or how much consumption would drop if advertising
expenditures were curtailed. Little direct evidence links food advertising
and overall diet quality. Studies that link the demand for individual
food products and advertising are legion—many show that advertising
does increase sales, and some show that advertising is cost-effective.
Even generic advertising studies usually show demand increases in
response to such expenditures. But, because food encompasses many
products and varieties, increasing demand for one food or even a
class of foods says very little about overall diet quality.
Evidence from the cigarette industry—where advertising has
been restricted—offers some insights. Numerous studies, though
ongoing, largely conclude that aggregate cigarette advertising has
a small or negligible impact on overall cigarette smoking. Promotional
expenditures sway consumers from one cigarette brand to another,
leaving the number of smokers and the number of cigarettes smoked
unchanged. If advertising affects food consumers similarly, then
restrictions on food advertising may have a larger impact on brand
choices than on overall food groups consumed or diet quality. Food
markets, for the most part, have stable aggregate demand, and advertising
levels are strategically used to maintain market or brand share.
Additional evidence from cigarette market studies suggests, however,
that advertising effects may be different for children. Cigarette
advertising is effective in getting children’s attention,
and children’s recall of the ads is correlated with smoking
behavior or initiation. For children, cigarette advertising may
be more inducement than brand identification.
Potential benefits of restricted food advertising could be complicated
in that across-the-board restrictions could result in lower prices
and increased consumption of foods bearing the advertising restriction.
Some studies found that aggregate cigarette consumption actually
increased after the U.S. banned broadcast cigarette advertising.
Cigarette companies, no longer allowed to compete through broadcast
commercials, were forced to compete more on price, and were able
to do so from advertising savings. If restrictions on food advertisements
have similar effects on price and consumption, then Americans could
end up fatter, not fitter.
Can Policies Reduce Obesity Rates?
Weight status—underweight, healthy weight, overweight, or
obese—is, for most people, an outcome of personal choices:
what and how much to eat and whether and how much to exercise. Changes
in habits are possible—recent statistics from the Centers
for Disease Control and Prevention indicate that former smokers
now outnumber smokers. Furthermore, habits would not have to change
drastically to lead to reclassifying the weight status of most Americans.
The American Dietetic Association says that each additional 3,500
calories a person consumes results in an additional pound of body
weight. That implies that a person who gave up 100 calories (equivalent
to a piece of toast) each day for a year would end up approximately
10 pounds lighter at year’s end.
The list of policies that could potentially help Americans turn
the corner on obesity and overweight is as long as the list of factors
that influence an individual’s diet and lifestyle choices.
The list of unintended consequences stemming from obesity policy
is probably longer. Even the most apparently straightforward policy
proposal can have surprising effects: mandatory nutrition information
at fast food restaurants could lead to reformulations or price promotions
that do not necessarily contribute to healthier diets; taxes on
snack foods could lead some consumers to substitute equally unhealthy
foods for the taxed food; and restrictions on food advertising could
ultimately lead to lower prices for food subject to the restrictions.
Food policy overflows with unintended consequences. The trick is
making sure they do not overwhelm the intended ones.
|



