To a Friend
|
Email this Page To a Friend |
|
U.S. Food and
Drug Administration
FDA Consumer magazine
September-October 2001
Table
of Contents
by Michelle Meadows
It was supposed to be a short course of treatment with tranquilizers after the death of her infant son 15 years ago. But Lynn Ray, 46, of Germantown, Md., says her abuse of the anti-anxiety drug Xanax and other prescription drugs led to a long struggle with addiction that nearly ruined her life.
Tranquilizers, which slow down the central nervous system and cause drowsiness, numbed Ray's agony, helped her sleep, and untied the relentless knot in her stomach. Soon, even if her doctor had prescribed one pill in an eight-hour period, she took two or three in an attempt to intensify the calming effect of the drug.
When the doctor stopped writing prescriptions for her and encouraged grief counseling, Ray began doctor-shopping--going from doctor to doctor, fabricating panic attacks, backaches, migraines, and other ailments that would get her multiple prescriptions for tranquilizers and pain killers. "I became a very good actress," Ray says. "I thought I needed these drugs no matter what, even if I had to bamboozle the doctors to get them."
Most patients take medicine responsibly, but approximately 9 million Americans used prescription drugs for non-medical purposes in 1999, according to the National Institute on Drug Abuse (NIDA). Non-medical purposes include misusing prescription drugs for recreation and for psychic effects--to get high, to have fun, to get a lift, or to calm down.
Experts stress that prescription drug abuse isn't about bad drugs or even bad people. It involves a complex web of factors, including the power of addiction, misperceptions about drug abuse, and the difficulty both patients and doctors have discussing the topic.
There is also the delicate balance of curbing criminal activity related to drug abuse while making sure that people with legitimate health needs can still access care, says Alan I. Leshner, Ph.D., director of NIDA. "We recognize the very real issue that millions of lives are improved because of prescription drugs--the same drugs that are sometimes abused," he says.
Ray had convinced herself that abusing prescription drugs was safer than abusing heroin, marijuana, and other "street drugs." "I would never do those," she says. "I figured I had a prescription for what I was doing, which made it OK."
Scott Walker, program director for substance abuse at the Mountain Comprehensive Care Center in Prestonsburg, Ky., says he hears that rationalization over and over. "Some people tell themselves they aren't using something old Joe cooked up in a garage somewhere," Walker says. They may figure a legitimate manufacturer made this, "so what could be the harm?"
As Ray's life unraveled, she found out the harm can be great, whether you're using heroin or sleeping pills. She lost her job as a computer programmer after repeatedly showing up late for work and falling asleep at her desk. Her son, a preteen at the time, couldn't understand her erratic behavior and didn't want anything to do with her.
Then in 1995, she crashed her car three times in one month while under the influence of tranquilizers and painkillers, seriously injuring others each time. Her driver's license was revoked, and she served a one-year jail sentence in 1998. "I will always know in my heart that I could have killed those people," she says. "It doesn't matter that I didn't kill them; it matters that I could have."
Walker says that roughly half of the people undergoing substance abuse treatment at Mountain Comprehensive Care Center come after realizing that they found themselves in a hole too deep to get out of on their own. The other half, like Ray, come because of some criminal charge related to drug possession or drug use.
OxyContin (oxycodone), a controlled drug approved in 1995 to treat chronic, moderate-to-severe pain, has received considerable attention because of deaths and crimes associated with its abuse. (For more on the classes--or schedule--of drugs, see "Controlled Substances".) OxyContin is a morphine-like narcotic that contains a high dose of oxycodone. Manufactured by Purdue Pharma, Stamford, Conn., the drug was originally believed to pose a lower risk for abuse because it is a controlled-release drug designed to be taken orally and swallowed whole, says Deborah Leiderman, M.D., director of the Food and Drug Administration's controlled substance staff. The drug's active ingredient, oxycodone, is slowly released over a 12-hour period. "But the safety of the drug is based on taking the drug exactly as intended," she says.
Abusers sometimes disrupt the time-release formula of the drug to speed up absorption, often chewing the tablets, crushing them and snorting the powder, or dissolving them in water and injecting the drug to get a fast high. Abusers have also used OxyContin with other painkillers, alcohol, and marijuana. Several deaths have resulted, mostly in rural areas of the Eastern United States, especially in Virginia and West Virginia.
Other products containing oxycodone such as Percodan and Percocet have also been abused over the years. Abuse of opiates is not new; what's new is the recent surge in local epidemics of opiate abuse (see "Most Commonly Abused").
The most highly abused stimulants are illicit drugs, including cocaine and methamphetamines. There also have been recent reports of Ritalin (methylphenidate) abuse among middle and high school students. The drug, which produces effects more potent than caffeine and less potent than amphetamine, is prescribed to treat attention-deficit/hyperactivity disorder and other conditions. But some have used it to suppress their appetite or to stay awake while studying. The DEA lists Ritalin as a "drug of concern" and reports that some abusers have dissolved the tablets in water and injected the mixture, which can block small blood vessels and damage the lungs and retina of the eye.
It's not that potentially addictive medications shouldn't be used, says Richard Brown, M.D., M.P.H., associate professor of family medicine at the University of Wisconsin Medical School. "They have an important place in the treatment of debilitating conditions." According to NIDA, drug addiction--characterized by drug craving that is out of control--is actually uncommon among people who use drugs as prescribed.
NIDA, along with several health organizations, has launched a national initiative to educate the public about the dangers of the non-medical use of prescription drugs, and the potential for abuse and addiction. With psychological addiction, there is a preoccupation with obtaining and using drugs that persists despite the consequences. Psychological addiction is distinct from physical dependence and tolerance, but the presence of these problems can complicate the treatment of addiction, says Alice Young, Ph.D., a professor in the department of psychology at Wayne State University in Detroit. "It is true that both psychological addiction and physical dependence can happen together," she says, "but they are not the same."
Young says that physical dependence, which is sometimes unavoidable, develops
when an individual is exposed to a drug at a high enough dose for long enough
that the body adapts and develops a tolerance for the drug. This means that
higher doses are needed to achieve a drug's original effects. "If the patient
stops taking the drug, then withdrawal will occur," Young says.
But the development of physical dependence doesn't necessarily lead to addiction
in all cases, she explains. "It means that the individual can't just stop
taking the drug; the dose has to be tapered," a method to gradually decrease
a drug's amount over time to prevent withdrawal reactions.
In addition to promoting public education, NIDA's initiative will foster new research on why certain people become addicted, says Leshner. "Some choose prescription drugs as the drug of choice, and others become addicted inadvertently," he says. "We want to learn more about what makes some people more likely to stray from the prescribed plan than others." NIDA also will support research into the mechanisms by which certain substances produce addiction.
Physician supervision and appropriate use is critical for all prescription drugs. Doctors consider a patient's diagnosis and whether non-addictive treatments should be considered first.
"Very strong opiate drugs play a critical role in pain management," FDA's Leiderman says. "But they aren't appropriate for all pain. Treatment needs to be tailored depending on a patient's specific condition."
Brown says doctors must also consider the patient's medical history and whether an individual has had addictive disorders in the past. But a history of substance abuse doesn't necessarily rule out using potentially addictive medications. "Patients should be honest about their substance abuse history because then it tells me to watch them even more closely," Brown says.
 A
good rapport between a patient and
doctor can make it easier to discuss
problems that come up, and health-care
professionals should carefully monitor
patients who take potentially addictive
medication. For some, that might
require a periodic urine drug screen,
Brown says. "This is not an
issue of distrust or intrusiveness,"
he says. "I explain to patients
that it's a way to help protect them,
especially because people who are
addicted may not recognize it. Addiction
can make people do things they wouldn't
normally do."
A
good rapport between a patient and
doctor can make it easier to discuss
problems that come up, and health-care
professionals should carefully monitor
patients who take potentially addictive
medication. For some, that might
require a periodic urine drug screen,
Brown says. "This is not an
issue of distrust or intrusiveness,"
he says. "I explain to patients
that it's a way to help protect them,
especially because people who are
addicted may not recognize it. Addiction
can make people do things they wouldn't
normally do."
A couple of Brown's patients experienced trouble with opioids and impulsivity--symptoms that led them to take more medicine than prescribed instead of waiting for the initial medicine to work. Brown picked up on the problems because both patients requested early refills. He switched them to non-drug treatments, such as physical therapy and relaxation techniques, until they could more successfully take prescription drugs.
Complicating matters is the fact that physicians are vastly undertrained in
identifying drug abuse. "The average physician gets little training in
drug abuse, mainly because drug abuse has only been recently recognized as a
health problem," Leshner says.
Brown says that some doctors are so concerned about penalties for overprescribing
potentially addictive medications that they don't treat patients appropriately.
"Other physicians mean well and prescribe the drugs, but don't know the
warning signs of abuse," he says. "Then there are those who just can't
say 'No' to patients who violate the prescribed plan."
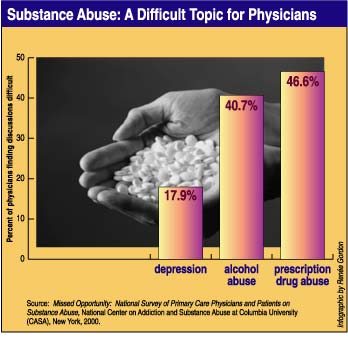
One recent survey from the National Center on Addiction and Substance Abuse
at Columbia University in New York City indicated that nearly half of primary
care physicians report having difficulty talking about substance abuse with
patients.
H. Westley Clark, M.D., J.D., director of the Center for Substance Abuse Treatment
at the Substance Abuse and Mental Health Services Administration (SAMHSA), says
his agency began a training program last year to help address this major problem.
The joint project with the Health Resources and Services Administration will train faculty members in the health professions. "It's not only for doctors," Clark says. "Other health professionals, including nurses and pharmacists, should also learn about recognizing the signs of substance abuse, talking about it, and knowing when patients should be referred for treatment."
For Ray, jail was the turning point. "There's something about those metal bars slamming shut behind you that makes it all very real," she says. A drug program in prison helped her beat addiction and taught her to cope with the triggers or life stressors that pushed her down the path to drug abuse.
"If you find yourself not following your doctor's orders, buying drugs off the street, or doctor-shopping, know that there is effective treatment and you can get help," Clark says. "If there is a treatment center within 100 miles of you, we can help you find it." (See "Treatment Centers".) Addiction is a brain disease typically treated with behavioral intervention, drug treatment, or often a combination.
Some treatments need to alleviate both withdrawal symptoms and the psychological addiction to drugs. Detoxification, the process by which the body recovers from tolerance and dependence, is considered a first stage in the sense that it purges drugs from the body. "It doesn't constitute a treatment," Young says. "Treatment has to address stopping future use."
Methadone, a synthetic opioid, has been used for more than 30 years to treat some opioid addictions. Levo-alpha-acety/methadol (LAAM) is another opioid treatment.
With methadone treatment, the patient receives both behavioral intervention and an oral, daily dose that maintains the physical dependence. When people abuse drugs, they commonly use fast routes of administration such as injection or inhalation, which basically slam the drugs into the brain. Methadone treatment delivers the narcotic orally so that it is slowly released in the body. The intent is to lessen the chance that the patient will use illegal opioids, Young explains. Among the goals is to decrease cravings for the "rush" created when opioids are taken by fast routes, and to prevent the occurrence of withdrawal signs by maintaining a steady level of opiate in the body. "It's a maintenance therapy over a long period of time, just like maintenance for diabetes, asthma, or any other chronic problem."
Prescription drugs commonly are diverted through fraudulent prescriptions, doctor-shopping, over-prescribing, and pharmacy theft. Clark says that dealing with diversion requires the involvement of patients, physicians, and pharmacists, and that there are many variables linking these three groups.
"Sometimes it's a matter of patients and physicians without adequate information about drug abuse," Clark says. "Sometimes overworked pharmacies don't notice when a patient is doubling up on a medication."
But as pharmacists look out for false or altered prescription forms and doctors look out for suspicious complaints, patients with legitimate medical problems still need fair treatment, Clark says. "We don't want to wind up punishing people in need."
Ellen Stovall, president of the National Coalition of Cancer Survivorship, says some cancer patients have been frustrated with the lack of appreciation for assessment of their own pain. The last thing patients need is a setback to pain management, Stovall says. "We have all the important laws around the abuse of narcotics, but we need legislation and support to protect people who are experiencing real, honest suffering."
Because of continuing reports of abuse, the FDA has strengthened the warnings and precautions sections in the labeling of OxyContin controlled-release tablets, a narcotic drug approved for the treatment of moderate to severe pain. Some of these reported cases have been associated with serious consequences, including death.
OxyContin contains oxycodone HCl, an opioid agonist with addiction potential similar to that of morphine. Opioid agonists act by attaching to specific proteins called opioid receptors, which are found in the brain, spinal cord, and gastrointestinal tract. When these drugs attach to certain opioid receptors in the brain and spinal cord, they can effectively block the transmission of pain messages to the brain.
OxyContin is a controlled substance in Schedule II of the Controlled Substances Act (CSA), which is administered by the Drug Enforcement Administration (DEA). Schedule II provides the maximum amount of control possible under the CSA for approved drug products. (For more on the classes--or schedule--of drugs, see "Controlled Substances".)
To educate health-care providers about the risks of OxyContin, Purdue Pharma of Stamford, Conn., manufacturer of the product, has issued a warning in the form of a "Dear Health Care Professional" letter, which will be distributed to physicians, pharmacists, and other health-care professionals. The letter highlights the problems associated with OxyContin abuse and explains the changes to the labeling, including proper prescribing information.
OxyContin, like morphine, has a high potential for abuse. It is supplied in a controlled-release dosage form and is intended to provide up to 12 hours of relief from moderate to severe pain. The tablet must be taken whole and only by mouth. When the tablet is crushed and its contents are injected intravenously or snorted into the nostrils, the controlled release mechanism is defeated and a potentially lethal dose of oxycodone is released immediately.
The FDA has worked with Purdue to make specific changes to the OxyContin labeling. The new labeling is intended to change prescription practices, as well as increase the physicians' focus on the potential for abuse and misuse. Changes include a "black box warning," the strongest type of warning for an FDA-approved drug. The new warnings are intended to lessen the chance that OxyContin will be prescribed inappropriately for pain of lesser severity than the approved use or for other disorders or conditions inappropriate for a Schedule II narcotic.
The FDA-approved use for OxyContin is for the treatment of patients with moderate to severe pain who are expected to need continuous opioids for an extended time. An important factor that must be considered in prescribing OxyContin is the severity of pain that is being treated, not simply the disease causing the painful symptoms.
The FDA continues to recommend that appropriate pain control be provided to patients who are living with severe pain. Although abuse and misuse are potential problems for all opioids, including OxyContin, opioids are very important treatment options for pain management when used appropriately under the careful supervision of a physician.
Because of the ongoing problem of OxyContin abuse and diversion, the FDA has met with the DEA, the Substance Abuse and Mental Health Services Administration, the National Institute on Drug Abuse, Purdue Pharma, and others. The FDA will continue to monitor reports of abuse and misuse of OxyContin and other opioids, and will work with other federal agencies and drug manufacturers to help ensure that these important drugs remain available to appropriate patients.
Because opioids are subject to abuse, the FDA is encouraging all manufacturers of opioids sold in the United States to review voluntarily, and revise as necessary, their products' labeling to provide adequate warnings and precautions regarding these risks and to promote responsible prescribing practices.
For more information, patients and health-care providers can call Purdue Pharma at 1-800-745-7445, or go to the FDA's Web site at www.fda.gov/cder/drug/infopage/oxycontin/.
--M.M.
The Controlled Substances Act categorizes drugs and substances into one of five schedules based on their medical use, abuse and addiction potential, and harmfulness. Schedule I drugs have the highest abuse potential. Heroin falls into the Schedule I category, drugs that have no accepted medical use in the United States. Schedule II drugs include OxyContin, morphine, and Ritalin. Schedule III drugs include anabolic steroids and Tylenol (acetaminophen) with codeine.
Legitimate handlers of controlled substances, such as hospitals and pharmacies, have to register with the Drug Enforcement Administration and use their registration numbers to purchase drugs. They must maintain complete and accurate records of all quantities manufactured, purchased, and sold. Drugs with higher abuse potential are subject to more restrictions than other drugs. For example, registered handlers must use a special order form to obtain Schedule II drugs. And orders for these drugs must be written and signed by practitioners and not phoned into the pharmacy except in an emergency. Prescriptions for Schedule II drugs also may not be refilled; patients have to go back to the doctor first. Those convicted of unlawful manufacturing, distributing, and dispensing of controlled substances face fines, prison sentences, or both.
--M.M.
The Substance Abuse Treatment Facility Locator covers more than 12,000 treatment
centers. To find a treatment center in your state, visit http://findtreatment.samhsa.gov/facilitylocatordoc.htm.
Or call the locator's toll-free numbers: 1-800-662-HELP (1-800-662-4357), 1-800-662-9832
(Spanish), and 1-800-228-0427 (TDD line for those who are hearing impaired).
--M.M.
National Institute on Drug Abuse
6001 Executive Blvd., Rm. 5213
Bethesda, MD 20892
301-443-1124
www.nida.nih.gov or www.drugabuse.gov
Substance Abuse and Mental Health Services Administration
Center for Substance Abuse Treatment
5600 Fishers Lane, Suite 618
Rockwall II
Rockville, MD 20857
301-443-5052
For publications, contact SAMHSA's National Clearinghouse for Alcohol and Drug
Information
1-800-729-6686
www.health.org
White House Office on National Drug Control Policy
Drug Policy Information Clearinghouse
P.O. Box 6000
Rockville, MD 20849
1-800-666-3332
www.whitehousedrugpolicy.gov/about/clearingh.html
--M.M.
(Graphic by Renée Gordon)
Table
of Contents | How
to Subscribe |
Back Issues | Editorial
Questions
FDA/Office of Public Affairs
Web page created by tg
2001-AUG-24.