What Is a Heart Transplant?
A heart transplant is an operation in which the
diseased heart in a person is replaced with a healthy heart from a deceased
donor. Ninety percent of heart transplants are performed on patients with
end-stage
heart
failure.
Heart failure is a condition in which the heart is
damaged or weakened and can’t pump enough blood to meet the body’s
needs. “End-stage” means the condition has become so severe that
all treatments, other than heart transplant, have failed.
Overview
Heart transplants are done as a life-saving measure
for end-stage heart failure when medical treatment and less drastic surgery
have failed. Because donor hearts are in short supply, patients who need a
heart transplant go through a careful selection process. They need to be sick
enough to need a new heart, yet healthy enough to receive it.
Survival rates for people receiving a heart
transplant have improved over the past 5 to 10 years—especially in the
first year after the transplant. About 88 percent of patients survive the first
year after transplant surgery, and 72 percent survive for 5 years. The 10-year
survival rate is close to 50 percent, and 16 percent of heart transplant
patients survive 20 years.
After the surgery, most heart transplant recipients
(about 90 percent) can come close to resuming their normal daily activities.
However, fewer than 40 percent return to work for many different reasons.
The Heart Transplant Process
The heart transplant process starts when doctors
refer patients with end-stage heart failure to a heart transplant center for
evaluation. Patients found to be eligible for a heart transplant are placed on
a waiting list for a donor heart.
Heart transplant surgery is done in a hospital when
a suitable donor heart is found. After the transplant, patients are started on
a lifelong health care plan involving multiple medicines and frequent medical
monitoring.
Who Needs a Heart Transplant?
Who Is Referred to a Heart Transplant Center?
Most patients referred to a heart transplant center
have end-stage
heart
failure. Of these patients, close to half have heart failure as a result of
coronary
artery disease. Others have heart failure caused by hereditary conditions,
viral infections of the heart, or damaged heart valves and muscles due to
factors such as the use of certain medicines and alcohol, and pregnancy.
Most patients considered for a heart transplant have
exhausted attempts at less invasive treatments and have been hospitalized a
number of times for heart failure.
Who Is Eligible for a Heart Transplant?
The heart transplant specialists at the heart
transplant center will determine whether a patient is eligible for a
transplant. Specialists often include a:
- Cardiologist (a doctor who specializes in
treating heart problems)
- Cardiovascular surgeon (a doctor who performs
the surgery)
- Transplant coordinator (a person who makes
arrangements for the surgery, such as transportation of the donor heart)
- Social worker
- Dietitian
- Psychiatrist
In general, patients selected for heart transplant
have severe end-stage heart failure, but are healthy enough to receive a heart
transplant. Heart failure is considered end stage when all possible
treatments—such as medicine, implanted devices, and surgery—have
failed.
Patients who have the following conditions might not
be candidates for heart transplant surgery, because the procedure is less
likely to be successful.
- Advanced age. Although there is no widely
accepted upper age limit for a heart transplant, most transplant surgery isn't
performed on patients older than 70 years.
- Poor blood circulation throughout the body,
including the brain.
- Diseases of the kidney, lungs, or liver that
can't be reversed.
- History of cancer or malignant tumors.
- Inability or unwillingness to follow lifelong
medical instructions after a transplant.
-
Pulmonary arterial hypertension (high blood pressure in the lungs) that
can't be reversed.
- Active infection throughout the body.
What To Expect Before a Heart Transplant
The Heart Transplant Waiting List
Patients who are eligible for a heart transplant are
placed on a waiting list for a donor heart. This waiting list is part of a
national allocation system for donor organs run by the
Organ Procurement and Transplantation Network (OPTN).
To make sure that organs are distributed fairly,
OPTN has policies on how donor hearts are allocated. These policies are based
on the urgency of need, the organs that are available for transplant, and the
location of the patient who is receiving the heart (the recipient). Organs are
matched for blood type and size of donor and recipient.
The Donor Heart
Guidelines on how a donor heart is selected require
that the donor meet the legal requirement for brain death and that the
appropriate consent forms are signed. Guidelines suggest that the donor be
younger than 65 years of age, have little or no history of heart disease
or trauma to the chest, and not be exposed to hepatitis or HIV. It’s also
recommended that the donor heart not be without blood circulation for more than
4 hours.
Waiting Times
Approximately 3,000 people in the United States are
on the waiting list for a heart transplant on any given day. About 2,000 donor
hearts are available each year. Wait times vary from days to several months and
will depend on a recipient’s blood type and condition.
A person may be taken off the list for some time if
he or she has a serious medical event such as a stroke, infection, or kidney
failure.
Time spent on the waiting list plays a part in who
receives a donor heart. For example, if a donor heart becomes available and
there are two recipients with equal need, the recipient who has been waiting
longer will usually get the heart.
Ongoing Medical Treatment
Patients on the waiting list for a donor heart
receive ongoing treatment for
heart
failure and other medical conditions.
Treating
arrhythmias
(irregular heartbeats), for example, is very important because they can cause
sudden
cardiac arrest in people who have heart failure. As a result, many
transplant centers will place implantable cardioverter defibrillators (ICDs) in
patients before surgery. An ICD is a small device that’s placed in the
chest or abdomen to help control life-threatening arrhythmias.
Another treatment that may be recommended to waiting
list patients is an implanted mechanical pump called a ventricular assist
device (VAD), which helps the heart pump blood.
Regular outpatient care for waiting list patients
may include frequent exercise testing, assessing the strength of the heartbeat,
and right
cardiac
catheterization (a test to measure blood pressure in the right side of the
heart).
Contact With the Transplant Center During the Wait
People on the waiting list are often kept in close
contact with the transplant center because most donor hearts must be
transplanted within 4 hours after removal from the donor.
At some heart transplant centers, recipients receive
a pager so the center can contact them at any time. They're asked to notify the
transplant center if they’re going out of town. Recipients often need to
be prepared to arrive at the hospital within 2 hours of being notified about a
donor heart. Not all patients who are called to come to the hospital will
get a heart transplant. Sometimes, at the last minute, the donor heart is found
to be unsuitable for certain patients. Other times, patients from the waiting
list are called to come in as possible substitutes in case something happens
with the selected recipient.
What To Expect During a Heart Transplant
Just before the heart transplant surgery, patients
will receive general anesthesia (that is, they’re temporarily put to
sleep).
A bypass machine is hooked up to the arteries and
veins of the heart. The machine pumps blood through the patient’s lungs
and body while the diseased heart is removed and the donor heart is sewn into
place.
Heart Transplant
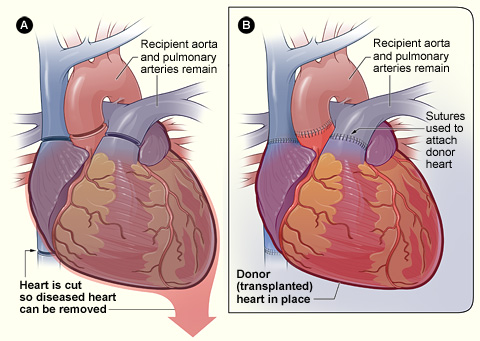
Figure A shows where the diseased
heart is cut for removal. Figure B shows where the transplanted healthy heart
is sutured (stitched) to the recipient’s arteries and veins.
Heart transplant surgery usually takes about 4
hours. Patients often spend the first days after surgery in the intensive care
unit of the hospital.
What To Expect After a Heart Transplant
In the Hospital
The amount of time a heart transplant recipient
spends in the hospital will vary with each person. It often involves 1 to 2
weeks in the hospital and 3 months of monitoring by the transplant team at the
heart transplant center. Monitoring may include frequent blood tests, pulmonary
(lung) function tests,
EKGs
(electrocardiograms),
echocardiograms,
and biopsies of the heart tissue.
A heart biopsy is a standard test used to see
whether your body is rejecting the new heart. It might be done frequently in
the weeks after a transplant. During a heart biopsy, a tiny grabbing device is
inserted into a vein of the neck or groin (upper thigh). The device is threaded
through the vein to the right atrium of the new heart to take a small tissue
sample. The tissue sample is checked for signs of rejection.
Watching for Signs of Rejection
The new heart is a “foreign body,” which
your immune system may attack if you’re not receiving enough medicine to
suppress your immune system after the surgery. Therefore, you and the
transplant team will work together to protect the new heart by watching for
signs of rejection. These signs include:
- Shortness of breath
- Fever
- Fatigue (tiredness)
- Weight gain (retaining fluid in the body)
- Reduced amounts of urine (problems in the kidneys
can cause this)
You and the team also will work together to manage
the transplant medicines and their side effects, prevent infections, and
continue treatment of ongoing medical conditions.
You may be asked to monitor your temperature, blood
pressure, and pulse when you go home.
Preventing Rejection
You will need to take medicine to suppress your
immune system so that the new heart will not be rejected. These transplant
medicines are called immunosuppressants. They’re a combination of
medicines that are tailored to your situation. Often, they include
cyclosporine, tacrolimus, MMF (mycophenolate mofetil), and steroids such as
prednisone.
Transplant medicines may need to be switched or
adjusted if they aren’t effective or have too many side effects.
Managing Transplant Medicines and Their Side
Effects
You will have to manage multiple medicines. Setting
up a routine for taking medicine at the same time each day and for refilling
prescriptions is helpful. It’s crucial to never run out of medicine. It
may help to always use the same pharmacy.
Keep a list of all medicines with you at all times
in case of an accident. When traveling, keep extra doses of medicine with you,
not packed in the luggage. Bring your medicine with you to all doctor visits.
Side effects from medicines can be serious. These
include risk of infection, diabetes, osteoporosis (thinning of the bones),
high
blood pressure, kidney disease, and cancer—especially lymphoma and
skin cancer.
Discuss any side effects of the medicines with your
transplant team, because the dose of a given medicine or the medicine
itself can be changed. Report all new medicines to your transplant coordinator.
Preventing Infection
Some transplant medicines can increase your chances
of developing infections. You may be asked to watch for signs of infection,
including fever, sore throat, cold sores, and flu-like symptoms.
Signs of possible chest or lung infections could
include shortness of breath, cough, and a change in the color of sputum (spit).
The incision must be checked for redness, swelling,
or drainage. It’s especially important to look for signs of infection,
because transplant medicines can often mask these signs.
Discuss with your doctor measures you should take to
reduce your chances of developing infections. For example, your doctor may
recommend that you avoid contact with animals or crowds of people in the first
few months after your transplant.
Regular dental care also is important. Your doctor
may prescribe you antibiotics before any dental work to prevent infections.
Pregnancy
Many successful pregnancies have occurred after
heart transplant surgeries; however, special care is important. If you’ve
had a heart transplant, talk with your doctor before planning a pregnancy.
What Are the Risks of a Heart Transplant?
Although heart transplant surgery is a life-saving
measure, it has many risks. Careful monitoring, treatment, and regular medical
care can prevent or help manage some of these risks.
Risks of heart transplant include:
- Failure of the donor heart
- Complications from medicines
- Infection
- Cancer
- Problems that arise from not following lifelong
health care plans
Failure of the Donor Heart
Over time the new heart may fail due to the same
reasons that caused the original heart to fail. Failure of the donor heart also
can occur if the body rejects the donor heart or if blood vessel disease
develops in the new heart and causes it to fail. This blood vessel disease is
called cardiac allograft vasculopathy (CAV).
Patients who receive a heart transplant that fails
can be considered for another transplant (called a retransplant).
Primary Graft Dysfunction
The most frequent cause of death in the first 30
days after transplant is when the new donor heart fails and isn't able to
function. This is called primary graft dysfunction. Factors such as shock or
trauma to the donor heart or narrowed blood vessels in the recipient's lungs
can cause primary graft dysfunction. Medicines (for example, inhaled nitric
oxide and intravenous nitrates) may be used to treat this condition.
Rejection of the Donor Heart
Rejection is one of the leading causes of death in
the first year after transplant. The recipient's immune system sees the new
heart as a "foreign body" and attempts to destroy or reject it. During the
first year, 25 percent of patients have signs of a possible rejection at least
once. Half of all possible rejections happen in the first 6 weeks after
surgery, and most happen within 6 months of surgery.
Cardiac Allograft Vasculopathy
CAV is a chronic (ongoing) disease in which the
walls of the new heart's coronary arteries become thick, hard, and lose their
elasticity. CAV can destroy the circulation of blood in the donor heart and
cause serious damage.
CAV is a leading cause of donor heart failure and
death in the years following transplant surgery. It can cause
heart attack,
heart
failure, dangerous
arrhythmias, and
sudden cardiac arrest.
Complications From Medicines
Taking daily medicines that stop the immune system
from attacking the new heart is absolutely critical, even though the medicine
combinations have serious side effects.
Cyclosporine and other medicines can cause kidney
damage. Kidney damage affects more than 25 percent of patients in the first
year after transplant. Five percent of transplant patients will develop
end-stage kidney disease in 7 years.
Infection
When the immune system—the body's defense
system—is suppressed, the patient is at increased risk for infection.
Infection is a major cause of hospital admission for heart transplant patients
and a leading cause of death in the first year after transplant.
Cancer
Suppressing the immune system leaves patients at
risk for cancers and malignancies. Malignancies are a major cause of late death
in heart transplant patients—nearly 25 percent of heart transplant deaths
3 years after transplant.
The most common malignancies are tumors of the skin
and lips (patients at highest risk are older, male, and fair-skinned) and
malignancies in the lymph system such as non-Hodgkins lymphoma.
Other Complications
High
blood pressure develops in more than 70 percent of heart transplant
patients in the first year after transplant and in nearly 95 percent of
patients in 5 years.
High levels of cholesterol and triglycerides in the
blood develop in more than
50 percent of heart transplant patients in the
first year after transplant and in
84 percent of patients in 5 years.
Osteoporosis can develop or worsen in heart
transplant patients. This is a condition in which bones gradually become
thinner and weaker.
Complications From Not Following Lifelong Health
Care Plans
Not following a lifelong treatment plan increases
the risk of all heart transplant complications. Heart transplant recipients are
asked to closely follow their doctors' instructions and monitor their own
health status throughout their lives.
Lifelong health care includes taking multiple
medicines on a strict schedule, watching for signs and symptoms of
complications, keeping all medical appointments, and stopping unhealthy
behaviors such as smoking.
Key Points
- A heart transplant is an operation in which the
diseased heart in a person is replaced with a healthy heart from a deceased
donor.
- Heart transplants are done as a life-saving
measure when medical treatment and less drastic surgery have failed. Most heart
transplants are performed on patients with end-stage
heart
failure.
- Donor hearts are in short supply, so patients who
need a heart transplant go through a careful selection process at a heart
transplant center.
- Patients who are eligible for a heart transplant
are placed on a waiting list for a donor heart. Policies on distributing donor
hearts are based on the urgency of need, the organs that are available for
transplant, and the location of the patient who is receiving the heart. Organs
are matched for blood type and size of donor and recipient.
- Waiting times for a donor heart vary from days to
several months.
- Heart transplant surgery usually takes about 4
hours. Patients might spend the first days after surgery in the intensive care
unit of the hospital.
- The amount of time a heart transplant recipient
spends in the hospital will vary with each person. It often involves 1 to 2
weeks in the hospital and 3 months of monitoring by the transplant team at the
heart transplant center.
- Once home, patients must carefully check and
manage their health status. Patients will work with the transplant team to
protect the new heart by watching for signs of rejection, managing the
transplant medicines and their side effects, preventing infections, and
continuing treatment of ongoing medical conditions.
- Risks of heart transplant include failure of the
donor heart, complications from medicines, infection, cancer, and problems that
arise from not following lifelong health care plans.
- Lifelong health care includes taking multiple
medicines on a strict schedule, watching for signs and symptoms of
complications, keeping all medical appointments, and stopping unhealthy
behaviors such as smoking.
- Survival rates for people receiving a heart
transplant have improved over the past 5–10 years—especially
in the first year after the transplant. About 88 percent of patients survive
the first year after transplant surgery.
- After the surgery, most heart transplant
recipients (about 90 percent) can come close to resuming their normal daily
activities.
Links to Other Information About Heart
Transplant
NHLBI Resources
Non-NHLBI Resources
Clinical Trials
|
