|
|
|
Physical Activity Protects against
the Health Risks of Obesity
Introduction
Considerable attention has been placed
on the increasing prevalence of obesity in our society.
One population-based study (Mokdad et al., 1999) indicated
that the prevalence increased from 12 to 18.9% from
1991 to 1998. Another study (Troiano & Flegal, 1998),
using a different set of national data, indicated that
the prevalence of obesity increased from 14.5% to 22.5%
over the past 2 decades. The trends are similar for
men and women and are consistent across different ages
and socioeconomic classes. While all of these data are
cross-sectional, the magnitude and repeatability of
the changes suggest that these trends reflect real changes
in the population prevalence of obesity.
There are major public health consequences
associated with these trends. Obesity has been linked
to a variety of serious diseases and metabolic disorders
including Type II diabetes, hypertension, dyslipidemia,
coronary heart disease, gall bladder disease, respiratory
diseases, various cancers and osteoarthritis (Pi-Sunyer,
1999). The direct economic costs of treating obesity
in the United States are estimated at over 70 billion
dollars (Colditz, 1999). The fact that obesity increases
with age combined with the rapidly expanding elderly
population suggests that the problems are likely to
even get worse in the near future. These trends are
troubling and have caused obesity to be recognized as
one of the leading public health problems facing our
society. The World Health Association released
a report on preventing and managing the global epidemic
of obesity (World Health Association, 1998). At the
same time, the National Institutes of Health released
a report on the identification, evaluation and treatment
of overweight and obesity (National Institutes of Health,
1998). In 1999, the American College of Sports Medicine
convened a meeting to describe the role of physical
activity in the prevention and treatment of obesity
and its co-morbidities. These recent developments reveal
the current emphasis being placed on addressing the
obesity epidemic.
Because there is little reason
to suspect changes in genetics over this short time frame,
the most common explanation for the recent trends in obesity
is that a variety of environmental and behavioral influences
have combined to make it harder for individuals to maintain
weight balance. Hill & Melanson (1999) recently
presented a conceptual model describing some of these
influences. The model suggests that the availability of
high fat, energy dense foods, coupled with large portion
sizes and low costs of fast foods have combined to drive
up energy intake. Conversely, declines in work related
physical activity, reduced activity of daily living and
increases in sedentary behavior tend to drive down daily
energy expenditure values. While some of these changes
may be subtle, they appear to be exerting large influences
on the population.
Obesity is clearly a multifactorial
problem but there is some evidence that physical inactivity
may play a more pivotal role in the overall process.
An ecological review of secular trends (Jebb & Moore,
1999) recently suggested that the prevalence of obesity
is more strongly related to decreases in energy expenditure
than to increases in energy intake. DiPietro (1999)
reached a similar conclusion in a review of studies
on the prevention of weight gain. She indicated that
habitual physical activity plays a critical role in
attenuating the age-related weight gain that is commonplace
in our society. She further suggested that an increasing
amount of activity might be needed to maintain a constant
body weight with age.
While physical inactivity appears
to be a strong contributing factor to the etiology of
obesity, studies on the effectiveness of physical activity
in promoting weight loss have been less than encouraging.
Because physical activity increases energy expenditure,
it is reasonable to assume that the combination of diet
plus exercise would be more effective than dieting alone
for weight loss. A recent review of 13 controlled studies
found that this is rarely the case (Wing, 1999). Only
two of the 13 studies reported statistically significant
differences in weight loss from the diet plus exercise
regimen compared to diet alone. The conclusion from
this review was that "…exercise does not significantly
increase initial weight loss over and above that obtained
with diet only." When the effect of exercise on
weight loss was studied without corresponding dietary
modifications, exercise was found to promote weight
loss in only one of five randomized controlled trials
(Ross & Janssen, 1999).
These results present a confusing
picture. Physical activity is clearly viewed as being
essential to the prevention of weight gain but fairly
ineffective (at least in clinical trials) at promoting
weight loss. On an individual level, the failure of
exercise to contribute to weight loss in a predictable
manner could be a major deterrent to continued involvement
in an exercise program. Overweight individuals who begin
an exercise program would likely remain motivated only
if they see some changes in body composition resulting
from their efforts.
On the positive side, recent evidence
suggests that physical activity confers health benefits
that are largely or entirely independent of changes
in body composition. These findings suggest that overweight
and obese individuals can obtain the same benefits of
physical activity as lean individuals. While the overall
health benefits of physical activity have become well
accepted, the general assumption (even among many within
the scientific community) has been that the benefits
are contingent or dependent on corresponding changes
in body composition. While physical activity can lead
to changes in body composition, the amount of change
depends on an individual's genetics, individual variability
in metabolism and possibly other lifestyle behaviors.
The cellular and metabolic adaptations occurring as
a result of physical activity appear to be independent
of these changes. Therefore, an overweight or obese
person can have good cardiovascular health as long as
he/she remains active and possesses a reasonable level
of fitness. This is clearly an important message that
should be conveyed to individuals who have struggled
with weight control all their lives.
The purpose of this article is to
review the relationships between physical fitness and
body composition and their combined effect on health2.
First we will review the epidemiological evidence for
a protective effect of physical fitness on the health
risks associated with obesity. Probable mechanisms for
this protective effect will then be described. A summary
of these observations will focus on the implications
of these findings for the treatment and prevention of
obesity.
Epidemiological Evidence for the
Protective Effect of Physical Activity
The science of epidemiology is predicated
on identifying and explaining causes of diseases in
the population. The general approach is to compare
the prevalence or rates of diseases in populations exposed
to certain potential risk factors against populations
not exposed to these risk factors. This is typically
evaluated with a statistic known as a relative risk
ratio (death rate in those exposed to a risk factor/death
rate in those not exposed to that factor). Different
exposure variables are studied to identify the factors
that increase risks for specific diseases or outcomes.
In these studies, it is important to discount other
competing explanations through progressive advances
in design and more complex analyses. Examples from the
Aerobics Center Longitudinal Study will be used to describe
the progression of epidemiological research used to
examine the protective effects of physical activity/physical
fitness on the health risks associated with obesity.
The Aerobics Center Longitudinal
Study
The Aerobics Center Longitudinal Study
(ACLS) is an on- going observational study of individuals
who have come to the Cooper Clinic in Dallas, Texas
for preventive medical examinations. A major strength
of the database is that objective measures of cardiorespiratory
fitness from maximal exercise treadmill tests are included
in the comprehensive medical exam. This has allowed
the relationships between physical fitness and a variety
of health outcomes to be examined in a large cohort
over an extended period of time.
Preliminary evidence for a protective
effect of fitness came from a study focused primarily
on the benefits of cardiorespiratory fitness for reducing
risks of all cause mortality (Blair et al., 1989). As
a way to document the persistence of these effects,
comparisons were made for individuals in three different
categories of body mass index - BMI (< 20, 20-25
and > 25). In these analyses, individuals in
the bottom 20% of the age and sex group distribution
for treadmill time were classified as unfit and those
in the top 40% were classified as high fit. The results
suggested that fit individuals with higher BMI values
had lower mortality rates than unfit individuals with
low BMI's. Because this study only examined moderate
levels of overweight (BMI > 25), additional confirmation
was required to test the strength of the findings.
A subsequent study (Barlow, Kohl,
Gibbons, & Blair, 1995) was conducted to examine
similar relationships among a larger sample (nearly
26,000) of men across three higher BMI ranges (<
27, 27-30 and > 30). In all three BMI categories,
moderately fit individuals and highly fit individuals
were found to have lower relative risk for all-cause
mortality than individuals in the unfit category. A
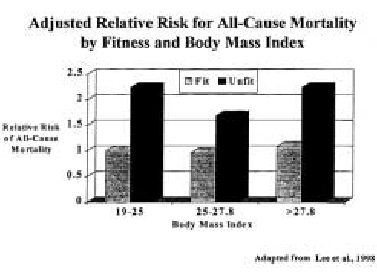
follow-up study (Lee, Jackson, & Blair, 1998) repeated
the analyses after excluding men with previous myocardial
infarction, stroke or cancer at baseline and adjusting
for exam year, smoking habit and alcohol intake. The
definition of unfit participants was the same as in
previous studies but in this study, all individuals
above the 20th percentile were classified as "fit".
Comparisons also were made using the fit and lean individuals
(< 25 BMI) as the reference group rather than making
comparisons separately for each BMI category. Unfit
individuals in each BMI category had greater risk of
dying as compared with the fit and lean group (relative
risks ranged from 1.68 to 2.24). An interesting observation
from this study was that there were no differences in
relative risk for fit individuals in the three different
BMI categories. Fit overweight men had no greater risk
than fit lean men (See Figure 1).
Figure 1.
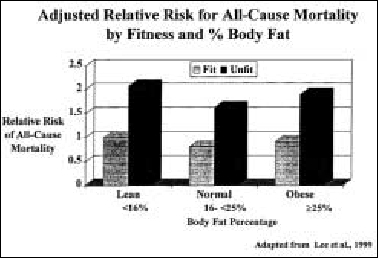
A limitation of the previous
studies was a reliance on BMI as the indicator of body
composition. To address this issue, another study (Lee,
Blair, & Jackson, 1999) examined the relationship
of cardiorespiratory fitness to mortality with more
specific measures of body composition. The study evaluated
the risks for all-cause mortality among men who had
received a body composition assessment (either sum of
7 skinfolds or underwater weighing) and a cardiorespiratory
fitness assessment. Individuals were classified as lean
if they had body fat levels less than 16.7%, normal
if they had body fat levels from 16.7 - 25% and obese
if they had body fat levels greater than 25%. Relative
risks for unfit individuals ranged from 1.62 to 2.07
compared with lean and fit men (See Figure 2). The investigators
also examined the relationships on a subsample of participants
who also had waist circumference measurements. These
participants were divided into 3 waist girth strata
(< 87 cm, 87 to 99 and > 99). The relative risks
for these comparisons were even higher – ranging from
2.05 to 4.88. The greatest risk was found for the lean
unfit group but this may have been due to the smaller
sample from this particular category. The main
message from the study was that risks are higher for
unfit men at all three waist circumference categories.
Figure 2.
The most comprehensive analysis on
the topic compared the relative importance of various
cardiovascular risk factors on cardiovascular disease
and all-cause mortality across different body composition
categories (Wei et al., 1999). In this study, the investigators
categorized men from the ACLS database into three different
BMI levels (< 25, 25-29.9 and > 30) and then sub-classified
by the presence or absence of six different mortality
predictors (cardiovascular disease, type II diabetes,
cholesterol, hypertension, current smoking status, and
low fitness). Low fitness was found to be an independent
predictor of mortality in all body mass index groups
even after adjusting for all of the other mortality
predictors. This suggests that being unfit is a risk
that adds to the risks already associated with other
risk factors. The magnitude of the relative risks for
low fitness in this study was as high or higher than
those for the other established co- morbidities.
Summary of Epidemiological Evidence
The studies reviewed above demonstrate
a strong protective effect for physical activity and
physical fitness on the health risks associated with
obesity. Consistent differences in health risks were
evident between fit and unfit individuals among all
body composition categories. Persistence in the proposed
protective effect is also evident in the fact that the
results have been found to be similar for a number of
different indicators of body composition, including
BMI, body fatness, fat free mass and waist circumference.
These effects were also found to be independent of potential
confounding variables as well as the presence of other
risk factors. While the relationships reviewed here
were demonstrated with fitness as an outcome, similar
relationships have been reported in studies using physical
activity as the primary exposure variable (Paffenbarger
& Hyde, 1984). Additional work is needed but the
current findings provide compelling evidence to support
the view that the health risks of obesity can be largely
managed through physical activity.
The reason this evidence has been
relatively slow to surface is that few epidemiological
studies have examined physical activity and body composition
as related, but independent, exposures. With respect
to health, studies linking physical activity and fitness
with health typically control for some aspect of body
composition. In contrast, studies linking body composition
with health have rarely considered the moderating influence
of physical activity and fitness. The erroneous assumption
has been that overweight or obese individuals would,
by default, be unfit. In a comprehensive review of the
current literature on this topic, Blair and Brodney
(1999) identified 24 articles that evaluated health
outcomes across levels of both physical activity/fitness
and some indicator of body composition. Sufficient data
were available to summarize outcomes of all-cause mortality,
coronary heart disease, hypertension, type 2 diabetes
mellitus and cancer. The studies consistently showed
that active or fit men and women were protected against
the health risks of overweight or obesity. The authors
concluded that "…active obese individuals actually
have lower morbidity and mortality than normal weight
individuals who are sedentary." (p. S646).
Probable Mechanisms for a Protective
Effect
Physical activity provides protection
against the health risks of obesity primarily by reducing
and/or reversing the development of a progressive disease
process known as insulin-resistance syndrome or Syndrome
X. This syndrome is closely associated with obesity
and is characterized by the clustering of insulin resistance
and hyperinsulinemia, dyslipidemia, essential hypertension,
glucose intolerance, and an increased risk of non-insulin
dependent diabetes mellitus and cardiovascular disease
(Landsberg, 1996; Opara & Levine, 1997; Timar, Sestier,
& Levy, 2000). Before describing the moderating
influence of physical activity, the general mechanisms
underlying insulin resistance syndrome will first be
described.
While research is still accumulating
on the specific mechanisms, the general disease process
is related to the presence of abdominal body fat - particularly
visceral fat (Despres, 1993; Chisholm, Campbell, &
Kraegen, 1997). Abdominal body fat is characterized
by an increased responsiveness to lipoprotein lipase.
Because of its high lipolytic activity, abdominal adipocytes
readily release free fatty acids (FFA) into the circulation.
These FFA are carried directly to the liver through
the portal circulation where they are converted into
very-low density lipoproteins (VLDL) and ultimately
LDL cholesterol. The high levels of FFA may also lead
to enhanced lipid oxidation and reduced glucose oxidation.
These changes can result in high levels of blood glucose
and lead to a reduced sensitivity to insulin.
The increased levels of FFA in the portal circulation
also act directly to inhibit insulin clearance by the
liver resulting in hyperinsulinemia. High levels of
insulin in the presence of elevated glucose tend to
promote reductions in insulin sensitivity and hasten
the development of non-insulin dependent diabetes mellitus.
The increased insulin levels also are associated with
increases in blood pressure as insulin is thought to
increase sodium retention in the kidney. Thus, high
levels of abdominal obesity are directly related to
dyslipidemia (elevated levels of LDL and triglycerides),
hypertension, hyperinsulinemia, reduced glucose sensitivity
and ultimately non-insulin dependent diabetes mellitus.
Physical activity induces beneficial
metabolic changes that limit the progression of this
underlying disease process. A major benefit of physical
activity is that it leads to specific reductions in
levels of abdominal obesity (Ross & Janssen, 1999).
The enhanced lipolytic activity of these fat cells allows
fatty acids to be released and metabolized more readily
than other fat depots. While overall weight loss from
exercise is limited, studies have indicated that changes
in abdominal body fat levels can occur without corresponding
weight loss or total fat loss. Studies have also demonstrated
that physical activity has a direct effect on improving
overall metabolic profiles (e.g. normalization of insulin
levels and improved glucose homeostasis). In a review
of these studies (Kelley & Goodpaster, 1999), the
improvements in insulin action were found to occur without
concomitant changes in weight and/or body composition.
While there appears to be some chronic adaptations that
occur as a result of regular exercise performed over
a period of time, there are also observations that indicate
that some benefits are related to the acute effects
following individual bouts of activity. The fact that
physical activity exerts some of its positive influence
independent of changes in body composition is consistent
with the findings from the epidemiological studies reviewed
earlier.
Summary and Conclusions
The general assumption in our society
is that overweight or obese individuals are probably
physically inactive and unfit. Conversely, most people
would assume that a thin individual is probably physically
active, physically fit and healthy. These characterizations
are gross oversimplifications and don't take into account
the complex metabolic relationships that influence body
composition, fitness and health. It is clearly possible
for overweight individuals to maintain high levels of
fitness. Through participation in regular physical activity,
it is also possible for overweight individuals to have
good health and low risks for chronic disease.
While the public health concerns about
the increasing prevalence of obesity are well founded,
they may be misplaced. The epidemiological studies reviewed
here suggest that the health risks of obesity are largely
controlled if a person is physically active and physically
fit. The protection appears to come, at least in part,
from positive metabolic changes that occur as a result
of regular participation in physical activity. Because
most of these changes have been found to occur independent
of changes in body composition it may prove more successful
to promote physical activity for its own sake - without
emphasizing or expecting corresponding changes in body
composition. If a larger percentage of the population
became physically active, the public health burden associated
with obesity would be greatly reduced. This conclusion
should not be interpreted to dismiss the health risks
associated with obesity, but rather to emphasize the
moderating influence of physical activity and physical
fitness on these risks. The implications of this distinction
for the clinical treatment of obesity and for health
promotion in general are described below.
Implications for Treatment
With regard to treatment, physicians
routinely counsel patients about the health risks of
obesity and typically prescribe various weight loss
treatments to address the issue. Guidelines published
by the National Institutes of Health (1998) recommend
that physicians test for the presence of other coexisting
diseases (co-morbidities) such as diabetes and hypertension
since the presence of additional risk factors has been
shown to compound overall health risks. The results
reviewed here suggest that low fitness (and/or lack
of physical activity) should be considered as equally
important when evaluating health status of overweight
or obese individuals. As previously stated by Wei et
al., (1999), it is as important for a clinician to assess
an obese patient's fitness status as it is to measure
fasting plasma glucose an cholesterol, evaluate blood
pressure and inquire about smoking habits.
Implications for Health Promotion
Weight loss is frequently cited as
one of the most common reasons for beginning an exercise
program. In light of the negative results from studies
on physical activity and weight loss, continued efforts
in this direction may be counterproductive. Many obese
individuals have become frustrated with exercise since
their efforts often do not lead to corresponding changes
in weight or body composition. Rather than encouraging
these individuals to lose weight it is more appropriate
and probably more effective to encourage them to just
become physically active. If regular physical activity
is performed, physical fitness will improve to the extent
possible and lead to positive metabolic outcomes. These
changes will provide significant benefits for health
regardless of any changes in body weight. The focus
on behavior rather than an outcome (e.g. weight loss)
also offers motivational advantages for obese individuals
since it increases the likelihood that they can be successful
and feel positive about their efforts. Specific guidelines
and strategies for using physical activity in this way
have previously been published (Leermakers, Dunn, &
Blair, 2000).
It is important to point out that
only modest amounts of physical activity are needed
to attain some protection against the health effects
of obesity. The cutpoints used to define the high risk
(low fitness) category in the ACLS is the lowest 20%
of the age-specific fitness distributions for both men
and women. When expressed in absolute levels of fitness,
the cutpoints for young adults (20-39 years) are approximately
8.1 and 10.5 METS (or a VO2 max of 28 – 35 ml/kg/min),
for women and men, respectively. Similar cutpoints for
middle aged adults (40-59 years) are approximately 7
and 9.5 METS (or a VO2 max of 25 – 33 ml/kg/min) . These
fitness levels can be achieved with modest amounts of
physical activity. A recent study examining activity
levels of ACLS participants (Stofan, DiPietro, Davis,
Kohl, & Blair, 1998) indicated that an average leisure
time energy expenditure of 525 to 1650 kcal per week
for males and 420 to 1260 kcal/week for females were
associated with moderate to high levels of fitness.
These levels of activity can easily be attained by following
the current public health guidelines for physical activity,
which recommend 30 minutes of moderate activity on most
days of the week (Pate et al., 1995).
The President's
Council on
Physical Fitness and Sports Research Digest
is now available on-line at http://www.indiana.edu/~preschal
Please note that the appropriate
language for the citation of this resource is:
The President's
Council on Physical Fitness and Sports Research Digest.
The President's Council on Physical
Fitness and Sports
The President's Council on Physical Fitness and Sports
(PCPFS) was established in 1956 through an Executive
Order by President Dwight D. Eisenhower as part
of a national campaign to help shape up America's younger
generation. Today, the PCPFS serves as an advisory council
to the President and Secretary of the
Department of Health & Human Services on matters
involving physical activity, fitness and sports to enhance
and improve the health of Americans of all ages.
The PCPFS enlists the active support and assistance
of individual citizens, civic groups, private enterprise,
and voluntary organizations to promote and improve the
physical activity and fitness of all Americans and to
inform the public of the important link which exists
between regular activity and good health.
Twenty (20) individuals from the sports, fitness and
health fields are appointed by the President to serve
as members of the Council. They are:
- Lee Haney, Chairman
- Elizabeth Arendt, M.D., St. Paul, MN
- Billy Blanks, Sherman Oaks, CA
- Jeff Blatnick, Halfmoon, NY
- Ralph Boston, Knoxville, TN
- Don Casey, East Rutherford, NJ
- Timothy Finchem, Ponte Vedra Beach, FL
- Rockne Freitas, Ed.D., Honolulu, HI
- Zina Garrison, Houston, TX
- Lauren Gregg, Charlottesville, VA
- Jimmie Heuga, Avon, CO
|
- Jim Kelly, Buffalo, NY
- Judith Pinero Kieffer, Los Angeles, CA
- Deborah Slaner Larkin, Pelham, NY
- Nikki McCray, Washington, D.C.
- Albert Mead III, Atlanta, GA
- Jack Mills, Columbia, SC
- Ellen Hart Peña, Denver, CO
- Ken Preminger, Atherton, CA
- Amber Travsky, Laramie, WY
- Executive Director—Sandra Perlmutter
|
200 Independence Avenue, S.W., Washington,
DC 20201 • (202) 690-9000 • FAX (202) 690-5211
Physical Activity and Fitness Quote
"If a larger percentage of
population became physically active, the public health
burden associated with obesity would be greatly reduced.
This conclusion should not be interpreted to dismiss
the health risks associated with obesity, but rather
to emphasize the moderating influence of physical activity
and physical fitness on these risks."
Gregeory J. Welk
Iowa State University, Ames, IA 50011
Steven N. Blair
The Coopert Institute, Dallas, TX 75230
1The concepts behind this
originated while Dr. Welk was the Director of the Childhood
and Adolescent Health Division, Cooper Institute.
2Much of the content for
the present article was based on the recent ACSM Roundtable
meeting and the subsequent publication of various review
articles (Blair & Bouchard, 1999).
Published quarterly by the President´s
Council on Physical Fitness and Sports, Washington,
D.C.
Guest Authors:
Gregory J.Welk
Iowa State University, Ames, IA
Steven N. Blair
The Cooper Institute, Dallas, TX
Co-Edited By:
Drs. Chuck Corbin and Bob Pangrazi Arizona State University
Reference List
Barlow, C. E., Kohl, H. W. I.,
Gibbons, L. W., & Blair, S. N. (1995). Physical
fitness, mortality and obesity. International Journal
of Obesity and Related Metabolic Disorders, 19,
S44.
Blair, S. N. & Bouchard,
C. (1999). Physical activity and obesity: American College
of Sports Medicine consensus conference. Medicine
and Science in Sports and Exercise, 31, S497-S497.
Blair, S. N. & Brodney, S.
(1999). Effects of physical inactivity and obesity on
morbidity and mortality: Current evidence and research
issues. Medicine and Science in Sports and Exercise,
31, S646-S662.
Blair, S. N., Kohl, H. W. I.,
Paffenbarger, R. S., Clark, D. G., Cooper, K. H., &
Gibbons, L. W. (1989). Physical fitness and all- cause
mortality: A prospective study of healthy men and women.
Journal of The American Medical Association,
262, 2395-2437.
Chisholm, D. J., Campbell, L.
V., & Kraegen, E. W. (1997). Pathogenesis of the
insulin resistance syndrome (syndrome X). Clinics
in Experimental and Pharmacological Physiology,
24, 782-784.
Colditz, G. A. (1999). Economic
costs of obesity and inactivity. Medicine and Science
in Sports and Exercise, 31, S663- S667.
Despres, J. P. (1993). Abdominal
obesity as important components of insulin-resistance
syndrome. Nutrition, 9, 452-459.
DiPietro, L. (1999). Physical
activity in the prevention of obesity: Current evidence
and research issues. Medicine and Science in Sports
and Exercise, 31, S542-S546.
Hill J.O. & Melanson, E.
L. (1999). Overview of the determinants of overweight
and obesity: current evidence and research issues. Medicine
and Science in Sports and Exercise, 31, S515-S521.
Jebb, S. A. & Moore, M. S.
(1999). Contribution of a sedentary lifestyle and inactivity
to the etiology of overweight and obesity: Current evidence
and research issues. Medicine and Science in Sports
and Exercise, 31, S534-S541.
Kelley, D. E. & Goodpaster,
B. H. (1999). Effects of physical activity on insulin
action and glucose tolerance in obesity. Medicine
and Science in Sports and Exercise, 31, S619-S624.
Landsberg, L. (1996). Obesity
and the insulin resistance syndrome. Hypertension
Research, 1, S51-S55.
Lee, C. D., Blair, S. N., &
Jackson, A. S. (1999). Cardiorespiratory fitness, body
composition, and all-cause and cardiovascular disease
mortality in men. American Journal of Clinical Nutrition,
69, 373-380.
Lee, C. D., Jackson, A. S., &
Blair, S. N. (1998). US weight guidelines: Is it also
important to consider cardiorespiratory fitness. International
Journal of Obesity, 22, S1-S7.
Leermakers, E. A., Dunn, A. L.,
& Blair, S. N. (2000). Exercise management of obesity.
Medical Clinics of North America, 84, 419-439.
Mokdad, A. H., Serdula, M. K.,
Dietz, W. H., Bowman, B. A., Marks, J. S., & Koplan,
J. P. (1999). The spread of the obesity epidemic in
the United States, 1991-1998. Journal of The American
Medical Association, 282, 1519-1522.
National Institutes of Health
(1998). Clinical Guidelines on the Identification,
Evaluation, and Treatment of Overweight and Obesity
in Adults: The Evidence Report. Rockville, MD: National
Institutes of Health, National Heart Lung and Blood
Institute.
Opara, J. U. & Levine, J.
H. (1997). The deadly quartet - The insulin resistance
syndrome. Southern Medical Journal, 90, 1162-1168.
Paffenbarger, R. S. & Hyde,
R. T. (1984). Exercise in the prevention of coronary
heart disease. Preventive Medicine, 13, 3- 22.
Pate, R. R., Pratt, M., Blair,
S. N., Haskell, W. L., Macera, C. A., Bouchard, C.,
Buchner, D., Ettinger, W., Heath, G. W., King, A. C.,
Kriska, A. L. A. M. B. H., Morris, J. P. R. S., Patrick,
K., Pollock, M. L., Rippe, J. M., Sallis, J., &
Wilmore, J. H. (1995). Physical activity and public
health: A recommendation from the Centers for Disease
Control and Prevention and the American College of Sports
Medicine. Journal of The American Medical Association,
273, 402- 407.
Pi-Sunyer, F. X. (1999). Comorbidities
of overweight and obesity: current evidence and research
issues. Medicine and Science in Sports and Exercise,
31, S602-S608.
Ross, R. & Janssen, I. (1999).
Is abdominal fat preferentially reduced in response
to exercise-induced weight loss? Medicine and Science
in Sports and Exercise, 31, S568-S572.
Stofan, J. R., DiPietro, L.,
Davis, D., Kohl, H. W., & Blair, S. N. (1998). Physical
activity patterns associated with cardiorespiratory
fitness and reduced mortality: The aerobics center longitudinal
study. American Journal of Public Health, 88,
1807-1813.
Timar, O., Sestier, F., &
Levy, E. (2000). Metabolic syndrome X: A review. Canadian
Journal of Cardiology, 16, 779-789.
Troiano, R. P. & Flegal,
K. M. (1998). Overweight children and adolescents:
Description, epidemiology, and demographics. Pediatrics,
101, 497-504.
Wei, M., Kampert, J. B., Barlow,
C. E., Nichaman, M. Z., Gibbons, L. W., Paffenbarger,
R. S., Jr., & Blair, S. N. (1999). Relationship
between low cardiorespiratory fitness and mortality
in normal-weight, overweight, and obese men. Journal
of The American Medical Association, 282, 1547-1553.
Wing R.R. (1999). Physical activity
in the treatment of the adulthood overweight and obesity:
Current evidence and research issues. Medicine and
Science in Sports and Exercise, 31, S547-S552.
World Health Association (1998).
Obesity: Preventing and Managing the Global Epidemic
Geneva, Switzerland: World Health Organization.
Indiana University
PRESIDENT'S CHALLENGE
Poplar's Research Center
400 East 7th Street
Bloomington, IN 47405 41-454-02
Back
to top
|