
|
|
Search | Index | Home | Glossary | Contact Us |
|
|
|

Please send comments to:
Perstephanie Thompson
Community Involvement Specialist
Agency for Toxic Substances and Disease Registry
1600 Clifton Road, MS E-31
Atlanta, Georgia 30333
or fax to: 404-498-0079
| This study and final report were supported in whole by funds from the Comprehensive Environmental Response, Compensation, and Liability Act (CERCLA) trust fund through the Agency for Toxic Substances and Disease Registry, U.S. Department of Health and Human Services. |
Community OutreachRESULTS
Study Population and Site Selection
Informed Consent
Privacy
Specimen Collection
Blood Sample Analyses
Children with Blood Lead Levels Above 10 micrograms per deciliter
Data Management and Tabulation
Program ParticipantsDISCUSSION
Blood Lead Levels
Dissemination of Information
Appendix A--Informed Consent
Appendix B--Specimen Collection Procedures
In response to community concerns of possible elevations in blood lead levels among the children of Anniston, Alabama, ATSDR facilitated a lead screening program during spring 2001. The screening program focused on children less than six years of age living in select areas of Anniston. Through the school system and community centers, ATSDR screened 410 children. A capillary blood sample was taken from each child using the finger stick method.Four children had blood lead levels greater than 10.0 micrograms per deciliter Their results, in micrograms per deciliter, were: 16.0, 13.7, 12.4, and 10.4. At the time the screening was conducted, these children were six, five, five, and three years of age, respectively. Three of these children were retested (through venipuncture) and two were confirmed elevated.
Results of this project do not provide a complete picture of blood lead levels in Anniston. Less than 1% of the children screened by ATSDR had a blood lead level higher than the CDC guidelines of 10.0 micrograms per deciliter However, approximately 25% of the children had a blood lead level 5.0 micrograms per deciliter These findings provide evidence that children are being exposed to lead. Although risks at these low levels are unclear, this evidence points to the need for continued screening and education for exposure prevention. ATSDR will continue to work with state and federal agencies, as well as the community, to implement recommendations for increased screening and awareness in Anniston.
Anniston, Alabama
The Agency for Toxic Substances and Disease Registry (ATSDR) is working with the Environmental Protection Agency (EPA) Region IV, the Alabama Department of Public Health (ADPH), and the Alabama Department of Environmental Management (ADEM) to characterize the environmental conditions in select areas of Anniston. Previous and ongoing investigations have determined that polychlorinated biphenyls (PCBs) are present in the soil at numerous residential properties. During some of the more recent investigations, elevated soil lead concentrations were also detected in residential properties.
During spring 2000, a screening investigation detected lead at levels exceeding 400 parts per million (ppm) in 36 residential properties in Anniston. Of these properties, the soil screening tests showed that 14 of the properties had soil lead levels in a range of 1000 to 3080 PPM In addition, soil at commercial properties contained elevated levels of lead. ATSDR reviewed the available data and determined that the soil in numerous residential properties presented a public health hazard. However, data were insufficient to determine the extent and source of the contamination (ATSDR 2001).
Lead Poisoning
Nationwide, lead-based paint in homes remains the major source of exposure among children. Many homes built before 1978 contain lead-based paint; after 1978 lead-based paint was banned from use on the interior and exterior of to 1990 Census data, 5,300 (31.3%) housing units in Anniston were built before 1950. Other sources or risk factors for lead exposure include industrial sources, parental occupations, and hobbies. Most commonly, children are exposed through ingestion of lead-contaminated dust (CDC 1997a). Most lead-contaminated dust is believed to come from lead-based paint (as a result of deterioration), but can also be a result of contaminated soil. Industrial processes (i.e., lead mining and smelter operations, battery recycling facilities, and foundries) are also potential sources of soil contamination.
Blood lead levels (BLLs) as low as 10 micrograms per deciliter (micrograms per deciliter) have been associated with long-term adverse effects on cognitive development, growth, and behavior among children under five years of age (NRC 1993). The Centers for Disease Control and Prevention (CDC) has established a BLL of 10 micrograms per deciliter as the level at which adverse health effects have been demonstrated (CDC 1991). States which receive federal funding for lead screening follow these CDC guidelines. However, evidence exists for subtle effects at even lower blood lead levels (Schwartz 1994, Campagna 2000, Lanphear 2001, Rothenber 2000).
The past decades of research on the health effects of lead have guided public health responses aimed at reducing lead poisoning. Because early evidence indicated that children are particularly sensitive to the effects of lead, much of the research, awareness, and prevention efforts have been focused on children. The effects of collective public health efforts are clearly shown in the dramatic reductions in childhood BLL over the past 20 years. Based on data collected from 1976 to 1980, children one to five years of age had an average BLL of 15 micrograms per deciliter By 1991 to 1994, the BLL of similarly aged children had decreased to 2.7 micrograms per deciliter,with 4.4% of children having a BLL of 10 micrograms per deciliter or higher (CDC 1997b). More recent data indicate a continuing decline in children's blood lead levels. The national average BLL in 1999 was 2 micrograms per deciliter, however, many areas with high prevalence of elevated levels persist (CDC 2000).
The likelihood of lead poisoning increases among children with multiple risk factors. The primary risk factors for lead poisoning include: low income, non-Hispanic black race, and living in older housing (Pirkle 1998). Based on data gathered in 1991 to 1994, 16.4 % of low-income children living in older housing had elevated BLLs, versus 0.9 % of high income children living in older housing. The data collected also suggest that children between one to two years of age have slightly higher BLLs than children three to five years old (CDC 1997b, Walter 1980).
Lead screening identifies children who need environmental or medical intervention because the majority of children with elevated BLLs do not develop clinical symptoms (CDC 1997b). There are two methods commonly for obtaining blood for lead screening. The first method requires a sample of blood obtained by venipuncture (blood is drawn from the vein). While results of this method are reliable and such a test is required to define a child requiring intervention, successful venipuncture in young children can be difficult and time-consuming. A second method uses blood obtained by finger stick and collected into a capillary tube. This method is easier and suitable for sampling larger groups of children. However, when blood is obtained in through finger stick, the possibility of contamination exists. When rigorous cleaning and a strict collection protocol are followed, finger stick results are more reliable (Schnlenker 1994, Parsons 1997, and Schonfeld 1994).
In response to community concerns, the purpose of this program was to supplement the existing lead screening program by the Calhoun County Health Department (CCHD), funded by CDC, through ADPH. ATSDR did not intend to perform universal screening in the Anniston community. Limited resources were set aside to conduct this activity. Based on an estimated 100 children per day, the program was equipped to screen 600 children.
The following were specific objectives of the screening program:
The success of this program was dependent upon participation, which relied heavily on community outreach. Outreach activities focused on educating Anniston residents about the dangers of lead poisoning and the benefits of childhood screening. In November and December 2000, ATSDR held two planning sessions with leaders of existing community groups in Anniston (Community Against Pollution, SweetValley/Cobbtown Environmental Justice Task Force, and Citizens for Environmental Justice), along with representation from the school system and Concern for Children, a local organization. ATSDR also held conversations with the Citizens Lead Education and Poisoning Prevention group in Birmingham, Alabama. The information gathered over a six-month period was used to design this blood lead screening program.
ATSDR partnered with Community Against Pollution (CAP). Through collaborative efforts, a logo was developed for this project, "Say Yes to the Lead Test," and flyers and posters were created to encourage participation. CAP representatives provided leadership on outreach strategies and distributed this information throughout the area. The educational materials included information about the effects of lead poisoning, the importance of screening, and special precautions for pregnant women exposed to lead.
ATSDR also issued a
press release at the start of the program and the screening events were
announced in the Anniston Star (local newspaper)to increase participation.
During the first week, the program received considerable publicity from local
media outlets.
Study Population and Site
Selection
The screening program focused on children under six years of age attending selected schools in Anniston. The program was designed to collect data from approximately 100 children per day, for six days, during a four-week period. The following locations were chosen by the community: Evelyn D. Hall Head Start, Wellborn Elementary School, Constantine Head Start, Cobb Elementary School, Carver Community Center, and Norwood Boys & Girls Club. Kindergarten and pre-K were the focus of these screening events. Head Start programs enroll children aged three to five years, so all students were invited to participate. CAP invited children to participate at the Norwood Boys & Girls Club and the Carver Community Center prior to the events.
Informed consent was obtained from all participants. An informed consent (Appendix A) described the purpose of the activity and collected basic demographic information. Parents (or guardians) were made aware that the program was voluntary, and a child or parent/guardian could stop participation at any time. Parents were also given an opportunity to have ATSDR send a copy of their child's results to their pediatrician.
As a federal public health agency, ATSDR is bound by federal law regarding the protection of the confidentiality of study participants. Under the Privacy Act of 1974 (5 U.S.C. Section 552a(e)), employees of federal agencies are responsible for protecting data collected on identifiable persons or organizations where the supplier of the information has not given the Agency consent to make that data public. Every precaution was taken to keep the information confidential to the extent permitted by law.

The Northeast Alabama Regional Medical Center (RMC) serves the Anniston community. Through ATSDR's contract mechanism, RMC Wellness Connection Bus was acquired to collect samples. The Bus is a clean and safe environment, suitable for the collection of samples. The Bus operated for up to 6-hours per day and was staffed with four to five experienced lab technicians at all times.
Prior to the screening event, the CDC National Center for Environmental Health (NCEH), Division of Laboratory Sciences, trained the Wellness staff for proper collection procedures, storage, and shipment. The NCEH laboratory provided lead-free materials for specimen collection, storage, and shipment. A capillary blood sample was taken from each child using the finger stick method. A description of this process is attached (Appendix B).
Each child was given a unique identifying number at the time the sample was taken. The same number was also placed on the child's consent form. All samples were shipped directly to the NCEH Laboratory at the end of each day. The Laboratory followed their standard procedure for analyzing blood lead levels (Appendix C includes a complete description of this process). The lead content was analyzed by using a Perkin Elmer Model 5100 atomic absorption spectrophoto-meter with Zeeman effect background correction. The lower limit of this instrument is 0.6 micrograms per deciliter After specimen analysis, individual laboratory data was sent electronically to ATSDR.
Children with Blood Lead Levels Above 10 micrograms per deciliter
The parents of children with a BLL greater than or equal to 10 micrograms per deciliter were notified by mail and telephone. According to CDC guidelines, children with BLLs 10-19 micrograms per deciliter must provide blood to confirm the elevation within 3 months of the finger stick (CDC 1997a). A representative from the ADPH lead program contacted each family to schedule a venous blood draw at the county health department. ADPH was responsible for all follow-up activities related to affected individuals, and those activities were directed by the guidelines established by CDC.
For follow up of children with confirmed elevated levels (greater than or equal to 10 micrograms per deciliter), CDC has recommended specific interventions to reduce the BLLs. The CDC recommended follow-up for children 10.0-19.0 micrograms per deciliter includes: providing families with lead education, offering follow-up testing, and referral for social services, if necessary (CDC 1997a). The CDC distributes this information to state and local health departments nationwide.
Data Management and Tabulation
Information collected on the informed consent was entered into a database by CDC staff. ATSDR conducted quality assurance/quality control (QA/QC) procedures to verify the accuracy of the data. The individual blood lead level (BLL) data were linked with the individual's demographic information (collected on the informed consent) by personal identifying numbers.
Descriptive analyses of population demographics were performed. Summary statistics were also tabulated for the BLL data. Because blood lead data are not normally distributed (some values are very large in magnitude compared to others), the geometric mean was computed. The lower limit of the laboratory instrument used to analyze the samples was 0.6 micrograms per deciliter, so samples less than 0.6 micrograms per deciliter were assigned as 0.3 (one-half the detection limit) for statistical analyses.
The program participants were self-selected and may not be representative of the general population. For this reason, results apply to those who participated and information gathered can not be generalized. Comparisons to summary statistics, such as national and state rates, and should not be made. The descriptive information collected through this program should inform and help direct public health practitioners and state and federal environmental agencies in making decisions about follow-up activities in Anniston.
Of the approximately 600 children invited to participate, 410 were screened. Table 1 describes the demographic characteristics of these children. Demographic information was not provided for all participants. Over 75 percent of the children screened were African American/Black. Roughly half of the children were male and half were female. Although the intent was to screen children under the age of 72 months, children over the age of six years were present at the two community-based screening locations and were included in the analyses. Overall, the children ranged in age from one month to 11 years; the majority were four through five years of age.
Table 1. Demographic characteristics of the program participants.
| Variable | Level | Frequency* | Percentage(%) |
|---|---|---|---|
| Sex | Male | 192 | 49.3 |
| Female | 198 | 50.7 | |
| Race | Black/African American | 307 | 75.6 |
| White | 80 | 19.7 | |
| Other | 19 | 4.7 | |
| Age (months) | <12 | 23 | 5.7 |
| 12-23 | 15 | 3.7 | |
| 24-35 | 18 | 4.5 | |
| 36-47 | 54 | 13.4 | |
| 48-59 | 103 | 25.6 | |
| 60-71 | 113 | 28.0 | |
| 72-83 | 72 | 17.9 | |
| 84+ | 5 | 1.2 |
*Not all participants reported demographic information .
Over 350 of the children screened currently reside in the city of Anniston. The remaining children live in communities surrounding Anniston. Fifty-eight households had more than one child screened, including 11 sets of twins and one set of triplets.
On average, about 70 children were screened each day. Figure 1 describes the
percentage of screenings conducted at each location. Approximately 40% of the
children were screened at Hall Head Start. On May 1st, a number of
community children, not enrolled in the school, were screened on the property of
Constantine Head Start.
Of the 404 samples analyzed, the geometric mean blood lead level was 2.9 micrograms per deciliter
The lowest detectable level was 0.6 micrograms per deciliter and the highest value was 16.0 micrograms per deciliter
Half of the results were 3.0 micrograms per deciliter or higher (the median). Figure 2 below
provides a summary of the blood lead levels. Over 75% of the children screened
were under 5.0 micrograms per deciliter
Four samples were greater than or equal to 10 micrograms per deciliter;
specifically 16.0, 13.7, 12.4, and 10.4. At the time the screening was
conducted, these children were 6, 5, 5, and 3 years of age, respectively. These
children were screened at Cobb Elementary School, Constantine Head Start, and
Hall Head Start and all live within the city limits of Anniston. By telephone,
mail, and in-person visits, ADPH and CCHD contacted the parent or guardian of
all four children with BLLs greater than or equal to 10.0 micrograms per deciliter
At the time this report was written, ADPH and CCHD were able to re-test three of
these children.
The child with a BLL of 16 micrograms per deciliter was confirmed at 13 micrograms per deciliter A home evaluation was
conducted by ADPH and results are expected in October 2001. The child with a BLL
of 13.7 micrograms per deciliter was confirmed at 3micrograms per deciliter and the child with a BLL of 12.4 micrograms per deciliter was
confirmed at 11.0 micrograms per deciliter
Figure 3 below provides information about blood lead levels by age. Within
each age group, most children had blood lead levels <5.0 g/d. However, of
children who were one year of age at the time of the screening, close to 50%
were 5.0-9.9 micrograms per deciliterApproximately 40% of children two to three years of age had
blood lead levels that ranged from 5.0 to 9.9 micrograms per deciliter. Children at these ages may
be more likely to be involved with hand-to-mouth activities that can increase
their opportunity for exposure (Walter 1980).
Figure 1.--Map of Screening Locations
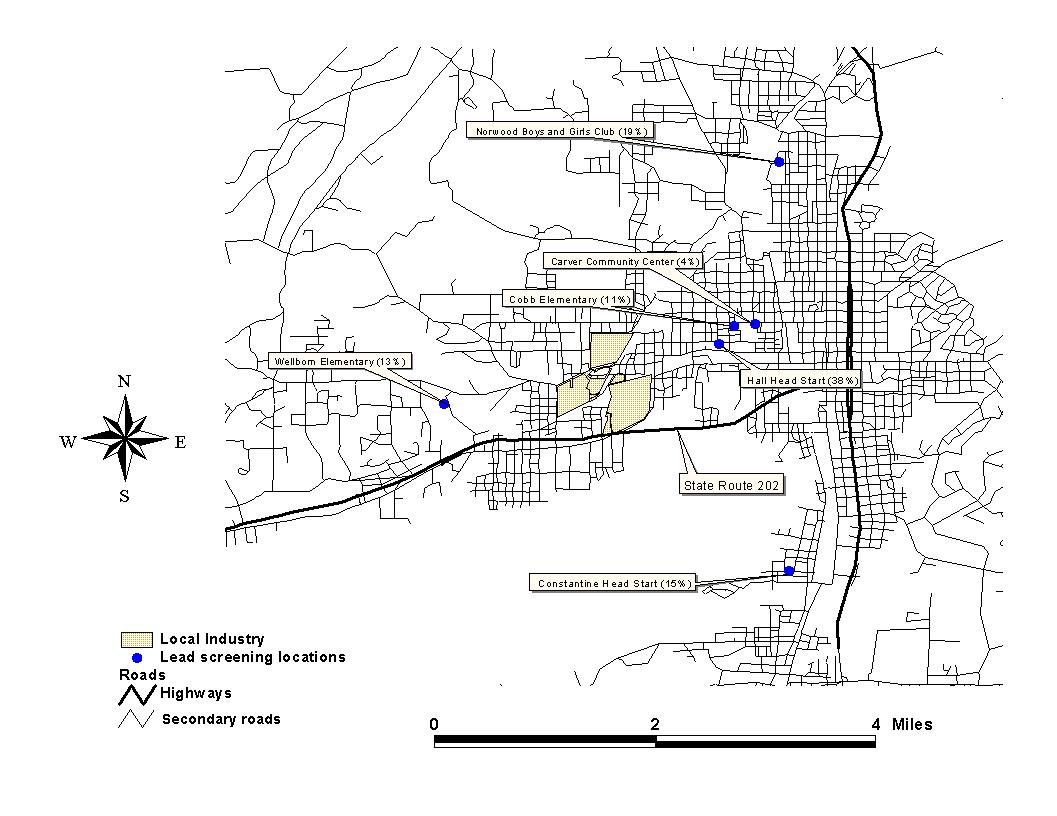
Figure 2.--The Distribution of Blood Lead Level (micrograms per deciliter ) Data
Figure 3.--Blood Lead Levels (micrograms per decilite) By Age
Individual results were mailed to each household during the week of June 11th. Three separate letters were created to convey the correct information to the parent or guardian: children greater than or equal to 10.0 micrograms per deciliter, children below 10.0 micrograms per deciliter, and children with insufficient amounts of blood to analyze the sample (Appendix D). During the week of June 18th, letters were sent to the children's pediatricians
Prior to its release, this draft report was sent to three external peer reviewers for an objective review. These reviewers are physicians and scientists who work at three different universities. They have expertise in lead exposure and/or pediatric medicine. A summary of the reviewers' comments and ATSDR's responses are attached (Appendix E). This report was released to the public in September comment. The report was mailed to the following repositories in Anniston, Alabama: the Anniston Public Library, Carver Library, the Environmental Protection Agency Community Relations Office, and Community Against Pollution.
A fact sheet was developed to address frequently asked questions regarding this activity. This will be mailed to the parents of all participants. After the report is released for comment, ATSDR will hold an availability session for parents to speak directly with ATSDR staff (scheduled for October 29, 2001).
The purpose of this program was to supplement the existing lead screening program. ATSDR did not intend to perform universal screening in the Anniston community. This program was not designed to evaluate risk factors for lead poisoning nor was it designed to determine the source of lead found in the blood samples. Blood lead levels were assessed at one point in time; this is a snapshot of the experience of this population, and does not provide information about potential risk factors, nor does it provide information about trends over time.
From the design stage to implementation, members of the community contributed to this project. Without the support from CAP, which was clearly conveyed to the Anniston residents throughout the process, community participation might not have been as high. CAP spoke to hundreds of parents and distributed a large amount of materials to educate residents about the effects of lead poisoning. The partnerships built during this project demonstrated the collaborative efforts and utilized the unique capabilities of local community groups, RMC staff, administrators and principals from county, city and Head Start school systems, the ADPH, CCHD, CDC, and ATSDR.
Of the 404 samples that were analyzed by the laboratory, four were greater than or equal to 10.0 micrograms per deciliter Because levels may be higher when the finger stick method is used, a venous sample was taken to confirm the result. Three of the children were re-tested and venous results confirmed two with BLLs 10.0 micrograms per deciliter The parent of the fourth child did not agree to have their child re-tested, but ADPH and CCHD will continue to work with this parent. Approximately one quarter of the children screened had a BLL greater than or equal to 5.0 micrograms per deciliter Although exposure effects to lower lead levels are unknown, these results emphasize the need to encourage parents and pediatricians to screen children at risk.
In the process of conducting this program, ATSDR collected information about the current lead screening practices in Anniston, Alabama. At no cost to the parent, the CCHD offers blood lead screening to children under 6 years of age. Parents can contact the health department at (256) 236-3274. However, if children are enrolled in Medicaid, the parent should contact their pediatrician to schedule a screening. According to the Advisory Committee on Childhood Lead Poisoning Prevention, children enrolled in Medicaid are legally entitled to screening at ages 12 and 24 months or at ages 36-72 months if they have not previously been screened. (CDC 2000). Community members may also contact the Anniston Quality Health Care Center at (256) 236-0221 for information about blood lead screening for children.
To date, EPA has sampled over 600 household yards in the Anniston area for lead. The addresses of the four children with blood lead levels greater than or equal to 10.0 micrograms per deciliter were checked with EPA's database to determine what sampling has been conducted at these homes. That search showed that no sampling has been conducted at the four properties in question. However, EPA is in the process of making arrangements to conduct sampling at all four locations.
Based on the finger stick method, four children had BLLs greater than or equal to 10.0 micrograms per deciliter Three of these children were retested and two of them were confirmed as "elevated." Results of this project do not provide a complete picture of blood lead levels in Anniston. However, this program identified a number of children with blood lead levels greater than or equal to 5.0 micrograms per deciliter These findings provide evidence that children are being exposed to lead. Although risk associated with these low levels is unclear, these results point to the need for continued screening and education for exposure prevention.
Based on the information collected during this program, the following activities are planned:
Authors
Sherri Berger-Frank, ATSDR/Division of Health Studies (DHS)/Health Investigations Branch (HIB)
Lakeisha Sykes, ATSDR/DHS/HIB
Clement Welsh, ATSDR/Division of Health Assessment and Consultation (DHAC)/Exposure Investigations and Consultation Branch (EICB)
Acknowledgments
These activities were possible with permission and assistance provided by Superintendent Stephen Nowlin and Ms. Theletha Williams (Anniston City Schools), Superintendent Jacky Sparks and Ms. Lesa Cotton (Calhoun County Schools), Principal Nancy Grogan (Wellborn Elementary), Principal Sharron Thomas (Cobb Elementary), and Ms. Dora Jones, Ms. Mary McCain, and Ms. Veronica Carter (Head Start Programs).
Thanks are also due to the community members who assisted with outreach activities and educating the residents of Anniston about the importance of blood lead screening. A well deserved thank you is extended to Ms. Shirley Williams, Community Against Pollution, who took the lead and went out into the community, week after week, to increase participation and awareness among the residents of Anniston.
This project would not have been successful without assistance from a number of staff in other ATSDR Divisions and Offices. PerStephanie Thompson (DHAC) served as a liaison between ATSDR staff and the community. In conjunction with the community, she coordinated the outreach activities and developed materials for distribution. Susan Moore, John Abraham (DHAC), and Mary White (DHS) played a significant role in the design and implementation of these activities. Carl Blair (Office of Regional Operations) served as the liaison between ATSDR and other state and local agencies. Both Mike Groutt and John Florence (Office of Policy and External Affairs) served as media liaisons, and Peter McCumiskey (Office of the Assistant Administrator) and Mike Youson (Office of Program Operations and Management) assisted with securing funds to support this program.
Ms. Noreen Pettit of the RMC Wellness Foundation did an outstanding job of coordinating the collection activities and keeping the children entertained throughout the process. Ms. Pettit and her hardworking staff brought a smile to the children's faces.
Our gratitude is also extended to Drs. Robert Jones and Kathleen Caldwell
(National Center for Environmental Health) for providing advice to ATSDR staff,
training to the RMC staff, delivering the necessary supplies, and analyzing the
samples. And, to Judy Waters of the Alabama Department of Public Health (ADPH)
and Donald Bain of the Calhoun County Health Department (CCHD) for providing
valuable input into the design and conduct of these activities.
Finally, special appreciation is extended to the parents and children of west Anniston who participated in this program.
Agency for Toxic Substances and Disease Registry. Health Consultation: evaluation of lead in residential surface soil from Anniston, Alabama. Atlanta: US Department of Health and Human Services, 2001.
Campagna D et al. 2000. Negative relationship between erythrocyte Ca-pump activity and lead levels in mothers and newborns. Life Sci. 68:203-15.
CDC. Preventing lead poisoning in young children. Atlanta, Georgia: US Department of Health and Human Services, CDC, 1991.
Centers for Disease Control and Prevention. Screening young children for lead poising: guidance for state and local public health officials. Atlanta: US Department of Health and Human Services, 1997a.
Centers for Disease Control and Prevention. Update: blood lead levels--United States, 1991-1994. MMWR 1997b; 46:141-6.
Centers for Disease Control and Prevention. Recommendations for blood lead screening of young children enrolled in Medicaid: targeting a group at high risk. MMWR 2000; 49:1-5.
Lanphear, B.P., K . Deitrich, P. Auinger, and C. Cox. 2000. Cognitive deficits associated with blood lead concentrations <10 micrograms per deciliter in US children and adolescents. Public Health Rep. 115(6):521-9.
National Research Council. Measuring lead exposure in infants, children, and other sensitive populations. Washington, DC: National Academy Press, 1993.
Pirkle JL, Kaufmann RB, Brody DJ, Hickman T, Gunter EW, Paschal DC. Exposure of the US population to lead, 1991-1994. Environ Health Perspect. 1998 Nov;106(11):745-50.
Parsons PJ, Reilly AA, Esernio-Jenssen D. Screening children exposed to lead:
an assessment of the capillary blood lead fingerstick test. Clinical
Chemistry 1997; 43(2):302-____
Rothenberg S, Poblano A, Schaans L. 2000. Brainstem auditory evoked response
at five years and prenatal and postnatal blood lead. Nerotoxicolo
Teratol 22:503-10.
Schlenker et al. Screening for pediatric lead poisoning: comparability of
simultaneously drawn capillary and venous blood samples. JAMA 1994;
271(17):1346-1348.
Schonfeld DJ et al. Screening for lead poisoning in an urban pediatric clinic
using samples obtained by fingerstick. Pediatrics 1994;
94(2):174-179.
Schwartz J. Low-level lead exposure and children's IQ: a meta-analysis and
search for a threshold. Environ 1994;65:42--55.
Walter SD, Yankel AJ, von Lindern IH. Age-specific risk factors for lead absorption in children. Arch Environ Health 1980;35(1):53-8.
Participant Consent for Blood Lead Level Screening Program
for Children
The Agency for Toxic Substances and Disease Registry (ATSDR), of
the US Public Health Service, US Department of Health and Human Services, is
screening children for their blood lead level. The authority for collecting
the information in this survey is the Comprehensive Environmental Response,
Compensation, and Liability Act of 1980 (CERCLA or Superfund). The purpose of
this program is to provide a public health service to the community.
Lead Poisoning
Behavior, learning,
and sleep problems may be caused by high levels of lead. You may not notice any
signs of lead poisoning. Children under 6 years of age are at greatest
risk.
Participation
Participation involves pricking your child's finger to get a sample of
blood to test for the presence of lead. There will be no physical examination
of the body. Should your child's results be high, you will
be contacted by an employee of the Alabama Department of Public Health to have
your child tested again to confirm the results.
There is little risk to your child. Benefits of the study
include: (1) individual results of your child's blood lead level mailed to
your home within 4 months, (2) individual results mailed to your child's pediatrician, if requested,
and (3) educational materials for you to share with your child about the risk
of lead poisoning.
Participation in this program is
voluntary. You may choose to stop at any time. If you choose not to participate,
or to stop at any time, there will be no penalty.
Privacy
Under the Information Federal Privacy Act of 1974
as amended, information obtained will be confidential. Reports written about
this program will give only group information and will not identify individuals.
APPENDIX B--SPECIMEN COLLECTION PROCEDURES
Caution: Treat all human blood as if it could transmit infectious diseases, e.g. Hepatitis, HIV etc. (wear fresh "powder-free" gloves for each patient)




Description of Analyses and QA/QC Procedures from the National Center for Environmental Health
The CDC lead analysis laboratory has met all CLIA '88 requirements, successfully participating in proficiency testing procedures for blood lead analysis.
Lead is measured in blood by atomic absorption spectrometry. Quantification is based on the measurement of light absorbed at 283.3 nm by ground state atoms of lead from either an electrodeless discharge lamp (EDL) or from a hollow cathode lamp (HCL) source. Blood samples, human and bovine blood quality control pools, and aqueous standards are diluted with a matrix modifier (nitric acid, Triton X-100, and ammonium phosphate). The lead content is determined by using a Perkin Elmer Model 5100 atomic absorption spectrophotometer with Zeeman effect background correction. Lead contamination must be carefully avoided throughout all procedures. All materials used for collecting and processing specimens are screened for possible lead contamination. All processing work is performed under clean conditions, including laminar flow hoods.
Two types of quality control systems are used in this analytical method. These two systems are: (1) "bench" quality control specimens that are inserted by the analyst two times in each analytical run ( a set of consecutive assays performed without interruption) so that judgments may be made on the day of analysis and (2) "blind" quality control samples that are placed in vials, labeled, and processed so that they are indistinguishable from the subject samples. The results of the blind specimens are decoded and reviewed by the supervisor. With both systems, all levels of lead concentration are assessed by taking these samples through the complete analytical process. The data from these materials are then used in estimating methodological imprecision and in assessing the magnitude of any time associated trends. Two levels of blind quality control pools are used. The levels chosen are in the "low-normal" (approximately 5 micrograms per deciliter) and "high normal" (approximately 20 micrograms per deciliter) range so as not to be obvious to the analyst. The pools are prepared in the same way as the bench pools and stored at -20C. At least one blind sample is randomly incorporated with every analytical run and analyzed according to the method protocol. The bench quality control pools comprise three levels of concentration spanning the "low normal", "normal", and high ranges for lead. Reference materials (blood products with certified values assigned by independent reference methods) are used periodically as a check of accuracy. NIST SRM 955 or 955b (levels A, B, C, and D) should be analyzed once every six months for this purpose. If the stock of these materials becomes low, another should be ordered in time to analyze it concurrently with the quality control materials currently in use so that a bridge may be formed between the materials. If the material ordered from NIST is from the same lot, a full characterization is not necessary. However, there should be some overlap between the old and new stocks. In addition, participation in external proficiency test serves to test accuracy. Quality control limits are established for each pool. An analysis of variance (ANOVA) is performed for each pool after twenty characterization runs have been performed in which previously characterized NIST SRM and bench quality control pools are used for evaluation. In addition to providing quality control limits, the characterization runs also serve to establish homogeneity of the pools. Once the homogeneity of the bench and blind materials has been established, it is useful to have them analyzed by another independent reference method, e.g. Isotope Dilution Mass Spectrometry.
Precision and Accuracy: After the standards and bench quality control materials are analyzed (at the beginning of an analytical run), the long-term quality control charts for each control material are consulted to determine if the system is "in control". Two types of charts are used. The first chart plots the means of the duplicate determinations and compares them to the 95% and 99% confidence limits as well as to the centerline (the overall mean of the characterization runs). The system is out of control if any of the following events occur for any one of the quality control materials:
The second type of quality control chart plots the range of the duplicate determinations and compares them to the 95% and 99% limits as well as to the center line. The system is out of control if any of the following events occur for any one of the quality control materials:
If the run is declared "out of control," the system (instrument, calibration standards, etc.) is investigated to determine the root of the problem before any analysis of specimens occurs.
ATSDR Home |
Search |
Index |
Glossary |
Contact Us
About ATSDR |
News Archive |
ToxFAQs |
Public Health Assessments
Privacy Policy |
External Links Disclaimer |
Accessibility
U.S. Department of Health and Human Services