 |
National Vaccine Program Office
Immunization Registries
Welcome Center | What's New | Publications | Contact Us
|
||||||||
National Vaccine Program Office Immunization Registries Welcome Center | What's New | Publications | Contact Us |
||||||||
|
|
Progress ReportApproved by NVAC: January 2002 Executive summary: Since approval of the report "Development of Community- and State-Based Immunization Registries" by the National Vaccine Advisory Committee (NVAC) in January, 1999, important progress has been made toward all four primary objectives identified in the report. In the area of privacy, confidentiality, and security, a document outlining minimum specifications has been approved and distributed. Important support for registries has been manifested by numerous professional organizations and agreement has been reached on key technical standards. Provider recruitment is proceeding, but not as rapidly as desired. Financial sustainability has not been achieved. Support continues through Federal Section 317 Immunization Grant funds and the prospect exists for support through Medicaid. Additional Federal support through the operational funds of the Vaccines For Children would provide a critical and stable base of financing. In addition to VFC support, a 5-year $60 million/year grant program would help support further development and initial implementation of registries. Finally, concerted efforts should be directed to getting financial support for immunization registries from the private sector (health plans/insurers). Introduction: On July 23, 1997, President Bill Clinton said: "I'm directing Secretary Shalala to start working with the states on an integrated immunization registry system....we have to do it and do it right." In response to this mandate, the National Vaccine Advisory Committee (NVAC) led an Initiative on Immunization Registries with support from the National Vaccine Program Office (NVPO) and the National Immunization Program (NIP) of the Centers for Disease Control and Prevention (CDC). Following a series of public meetings and focus groups, NVAC approved the report "Development of Community- and State-Based Immunization Registries" on January 12, 1999. The report identified four objectives and recommendations and action steps for each. Immunization registries are "confidential, computerized information systems that contain information about immunizations and children." The goal is to "establish a nationwide network of community/state population-based registries that are capable of sharing information while maintaining privacy and confidentiality." The purpose of this report is to highlight progress toward achieving that goal in the past 20 months, describe major remaining issues, and make recommendations for future action. The progress report is organized according to the four primary objectives identified by NVAC and the action steps NVAC recommended. Three recent actions transcend these specific objectives. The first is the release of the Healthy People 2010 objectives in January 2000. Objective 14-26 is to "increase the proportion of children [<6 years of age] who participate in fully operational population-based immunization registries" to 95% by 2010. The second is the convening of two highly successful conferences on immunization registries co-sponsored by CDC, All Kids Count (AKC), and host state health departments. More than 360 persons attended the 1999 conference in St. Paul MN and almost 400 attended the 2000 conference in Newport RI. CDC has committed to support annual registry conferences in the future. The third major action was the release, in June 2000, of the Institute of Medicine (IOM) report "Calling the Shots: Immunization Finance Policy and Practices." The report characterized the immunization program as a "national treasure that is too often taken for granted." It also described the importance of reminder/recall, assessment, etc., as major components of successful immunization programs. These functions are all facilitated by use of immunization registries. The IOM committee stated that "Once fully operational, registries may allow communities to target their outreach and other interventions more successfully, as well as achieve significant savings in other surveillance programsY.immunization registries offer one of the most useful instruments for assessing the population-specific effectiveness of health and medical care programs. Specific objectives
Action steps:
Progress: In February 2000, NVAC approved a document outlining minimum specifications for privacy, confidentiality, and security. This document, an update of a chapter approved by NVAC in 1997, addresses confidentiality policies, user agreements, parent notification, parental consent, use of immunization data, access to and disclosure of registry information, liability penalties for unauthorized disclosures, data retention and disposal, and security of data. The chapter was developed under the leadership of CDC in close consultation with privacy experts and is consistent with HIPAA legislation and proposed regulations. It has been widely disseminated and is available on the NIP/CDC registry web site. CDC has made strong recommendations to its project sites to develop written policies and procedures consistent with these minimum specifications. Information is currently incomplete as to the degree of compliance, but no reports have been submitted to CDC or DHHS describing instances in which confidentiality has been breached. Major remaining issues: Interstate exchange of information while assuring appropriate protection of confidentiality within individual states has not yet been achieved. A pilot project is under development between the states of Washington and Oregon to test this exchange. In addition, a Memorandum of Understanding on data exchange between North Carolina and Tennessee is now being extended to other states through the Southern Governors Association. Recommendations:
Action steps:
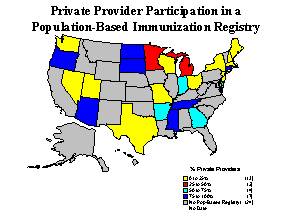
Progress: Many organizations have passed resolutions or made statements endorsing immunization registries, including the American Academy of Pediatrics, American Association of Health Plans, American Medical Association, American Osteopathic Association, American Public Health Association, American School Health Association, Association of State and Territorial Health Officials, Informed Parents Against Vaccine Associated Paralytic Polio, National Association of County and City Health Officials, National Association of Pediatric Nurse Associates and Practitioners, National Association of School Nurses, National Medical Association, National School Boards Association, and the U.S. Secretary of Education. Educational materials have been developed at national, state, and local levels for parents and providers. A toolkit to help registry coordinators work with private providers has been developed by a workgroup led by AKC and will shortly be distributed to CDC immunization projects and other registries. Intensive efforts to recruit private providers are underway at the local level but progress is not as rapid as desired. Providing information back to providers and focusing on simplicity are important tools in recruitment. Efforts are underway at national and state levels to establish methods that can consistently and accurately "de-duplicate" records, increase the timeliness and ease of reporting data, and provide a standard "language" so state and local registries can exchange information. CDC is establishing a system of "sentinel" or model registries. Several state and local registries have systems that meet nearly all of the 13 functional standards considered essential for registry operations and are able to capture almost all the data on children <6 years of age in their catchment areas. These registries will be asked to provide quarterly updates of vaccine coverage levels for their populations and may be asked to examine specific questions on vaccine use or uptake. Successful demonstrations of the practical uses of registry data and the timeliness of their assessments will be important demonstrations of their need and value. An important action to help create demand by parents and providers has been an increased emphasis on data quality to ensure that information from disparate sources is consolidated into a single complete record of each child's immunizations. The CDC June 2000 National Registry Report indicates that registries are under development or in operation in all states of the country as well as the District of Columbia and Puerto Rico. 47 jurisdictions reported information on current functionality of population-based immunization registries. These included 27 states, DC, PR, and 18 city or regional registries. In these areas, 40.7% of children 0-6 years of age are currently enrolled in registries (Figure 1). In the same areas, 58.6% of public providers and 19.6% of private providers are participating in registries (Figure 2). With respect to integration, 76.6% of registries report they are sharing information with vital statistics systems, 70.2% with Community/Migrant Health Centers, 53.1% with public clinic billing systems, 53.1% with hospitals, 46.8% with WIC, 46.8% with private clinic billing systems, 40.4% with managed care organizations, 38.3% with Medicaid Management Information Systems, 34.0% with schools, and 31.9% with Indian Health Service facilities. A major effort is currently underway in New York City to link the Citywide Immunization Registry with the lead poisoning program information system. CDC, the Health Resources and Services Administration (HRSA), and All Kids Count are working on integration of other systems including newborn metabolic and hearing screening. Major remaining issues: Continued recruitment of providers and parents. Recommendations:
Action steps:
Progress: A major step forward was realized with the development of implementation guidelines for exchanging immunization information using Health Level 7 (HL7) protocols. These guidelines were developed through leadership from CDC working in collaboration with six registries, Kaiser Permanente, Indian Health Service, and AKC. Adherence to these guidelines will enable ready exchange of information in a standard format between registries. Even before the 1999 NVAC report was issued, CDC had established a mechanism for acquiring immunization registry software using Section 317 Direct Assistance immunization funding. Contracts were awarded to four vendors of commercially available Immunization Information Systems Software whose core systems meet the minimum functional requirements established by CDC. This approach makes it easy for grantees to obtain software meeting (and exceeding) minimum specifications. CDC has modified the grant guidance for the 317 Immunization Grant Program to require that applicants include objectives and action steps for each of the 13 functional standards for registries. The Advisory Committee on Immunization Practices (ACIP) has endorsed precise definitions as to what constitutes an acceptable minimum/maximum age and interval for administering a particular vaccine. CDC used these definitions to develop algorithms for their use. This will free registry developers from having to develop their own algorithms and make it easier for registries to agree on what constitutes adequate immunization. By assuring consistent definitions of adequate immunization (e.g., defining adequate measles immunization as a dose administered not more than 7 days before the first birthday), the algorithms will prevent unnecessary revaccinations. A Technical Working Group (TWG) has been formed with representatives from informatics and standards-making organizations, health care software vendors, field registry managers, managed care organizations, state/local health departments, and staffed by CDC. The TWG has reviewed and endorsed the 13 Immunization Registry Functional Standards developed by CDC that are being used as criteria for evaluating registries. Discussion continues on what evaluation tools should be used, and what approach should be taken to certification. As recommended by NVAC, a Committee on Immunization Registry Standards and Electronic Transactions (CIRSET) has been formed and receives staff support from CDC. It includes immunization registry developers who are actively developing data exchange capability with other registries and providers and who have agreed to follow the HL7 implementation guide. CIRSET intends to establish common implementation policies and provide technical assistance to other developers. In addition, CIRSET intends to approach vendors about building the HL7 specification into their information systems. To assist with CIRSET's efforts, CDC is developing a public domain HL7 parser for intended distribution to registry developers in 2002. The Vaccine Identification Standardization Initiative (VISI) is working to develop standardized unique identifiers for each vaccine manufacturer, formulation, and lot. This information will be bar-coded and make it much easier to enter specific vaccine information into registries. CDC carries out an annual survey of immunization registries to monitor the extent of development, enrollment of children and providers, and functionality. Some preliminary results from the 2000 Report are provided in the preceding section. It should be kept in mind that the data are self-reported. An American Immunization Registry Association (AIRA) has been formed to foster immunization registry development across the country through provision of technical expertise, research, education, and training; provide a forum for information exchange and innovation; promote use of universal registry standards; and build partnerships among public and private registry networks, vendors, providers, and official agencies. CDC holds monthly conference calls with state and city registry managers and representatives from the Health Care Financing Administration (HCFA), HRSA, U.S. Dept. of Agriculture (USDA), Association of State and Territorial Health Officials (ASTHO), All Kids Count (AKC), Every Child by Two (ECBT), and Information for Public Health Officials (INPHO) to improve communication and discuss contemporary issues. There is increasing evidence of registries being used to improve immunization practice and carry out important public health and assessment functions. A few examples follow:
Major remaining issues: HL7 standards and the ACIP algorithm are not yet fully implemented, certification standards and procedures have not yet been finalized, and many registries are not yet fully making use of the information contained for programmatic activities. Additionally, some technical issues remain to be worked out to facilitate exchange of information between registries. Recommendations:
Action steps:
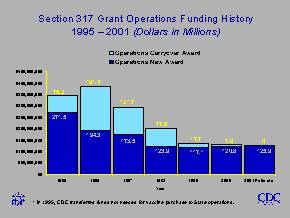
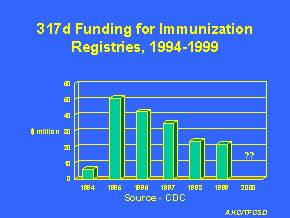
Progress: Both CDC and AKC have completed cost studies of registries; the AKC study has been published in the American Journal of Preventive Medicine. Based on these studies it can be estimated that it will cost approximately $125 million/year to operate a nationwide network of population-based immunization registries covering children from birth through the sixth birthday. The AKC study also estimated that nationwide use of registries would offset approximately $114 million/year now being spent within the health care system. More than half of this represents current efforts to retrieve records, assess adequacy of immunization and transcribe information to provide records for school entry or change of provider. Other savings would accrue from avoiding duplicate immunization and not having to perform the National Immunization Survey. AKC also obtained information from 43 states indicating that their school systems currently spend more than $168 million/year to review immunization records, a task that would be done automatically using registries. Thus, an investment of $125 million/year would offset more than $280 million currently being spent by the health care and school systems. Further studies are needed to fully characterize both the costs and the savings associated with use of registries. CDC ascertained the current sources of funding for immunization registries. It found that 42% of registry costs are currently coming from Immunization Grant (317) funds. States are providing 32% of the costs, and a variety of sources (including local governments, foundations, private sources) provide the remainder. On May 1, 2000, a legislative briefing on Immunization Registries was held, co-sponsored by All Kids Count, Every Child By Two, and several major health and education organizations. Congressional co-sponsors included 8 Senators and 3 Representatives. Major remaining issues: While current cost estimates provide a good foundation for understanding current and future financing needs, further, independent, studies will be needed to reflect new developments. Based on the current level of 317 funding and the proportion of registry costs that are provided from 317, it can be estimated that approximately $50 million/year is currently being spent on registries. Comparing that to the $125 million/year needed to maintain registries, it is apparent there is a shortfall of approximately $75 million/year. Ongoing discussions with a range of stakeholders have identified a variety of possible funding sources. From the federal level these could include increases in support through Section 317, the 5-year grant program recommended by NVAC, use of some of the vaccine excise tax, Vaccines for Children (VFC) operational funds, HCFA/Medicaid, or support from other programs (e.g., newborn metabolic screening). Non-federal sources could include state or local governments (including school systems), insurers and health plans, foundations, or fee-for-service. Each will be considered briefly below. Immunization grant (317) � overall funding for this program has been declining (Figure 3) and the amount of 317 support for immunization registries has also been declining � from a peak of approximately $50 million in 1995 to approximately $21 million/year in 1998 and 1999 (Figure 4). For FY 2001, states requested approximately $75 million more for program operations than was in the budget request. Even if this amount were appropriated, it would mean only approximately $10 million more for registries. New 5 year grant program � no legislation has been drafted. Vaccine excise tax � although this would seem to be an equitable way to spread the cost of registries across the private and public sectors, it seems highly unlikely such a proposal could win approval currently. VFC operational funds � approximately 40% of children less than 7 years of age are uninsured or covered by public insurance only and thereby VFC eligible. An unknown additional number of children are VFC eligible because they are underinsured and seeking care in Federally Qualified Health Centers. Nationwide, approximately 40% of childhood vaccines are purchased through VFC. Given the tremendous benefits to VFC of registries, it seems appropriate for VFC operational funds to be used to help develop and operate registries. Such support seems totally consistent with the VFC legislation, which requires creation of an accurate and complete immunization history on a child, accurate assessment of immunization needs, prevention of unnecessary doses of vaccine, and estimating coverage rates. This could provide a critical and stable base of financial support HCFA/Medicaid � approximately 26% of children less than 7 years of age are covered by public insurance. HCFA has chosen immunization coverage as one of its GPRA indicators. Because registries can both help to improve coverage and document the coverage achieved, it is logical for Medicaid to support immunization registries. An important step has been taken with the July 7, 2000, letter from the Director of Medicaid announcing availability of federal matching funds for registry costs associated with Medicaid eligible children. Matching would be at the 90% or 75% level for registries residing in, and part of, a state's Medicaid Management Information System (MMIS). For registries that exist independent of the state's MMIS (probably the majority), the match would be at the 50% level. Other federal programs � discussions are ongoing with programs such as newborn metabolic screening and newborn auditory screening about ways of integrating and linking systems. However, the level of funding of these programs does not suggest they could make a significant contribution to immunization registry operations. State/local governments � state governments currently contribute 32% of registry costs and local governments 1%. While much of the benefit of registries will accrue to state and local governments (by reducing school system expenditures for assessing immunization records) and some increases might be possible, patterns of state and local expenditures do not indicate a great likelihood that significant increases will be forthcoming. Insurers/health plans � in some areas insurers and health plans are currently providing support for registries. Since 60% of children are covered by private insurance and since both insurers and plans derive considerable benefits from registries (e.g., healthier children, HEDIS reports), it seems logical that insurers and health plans should uniformly provide support for registries. To date this avenue has not been pursued vigorously at the national level. Foundations � several foundations have contributed to registries. For example, the Robert Wood Johnson Foundation has provided approximately $20 million over the past 6 years to support registries (through the All Kids Count program). Other foundations have contributed smaller amounts. However, these do not appear viable as long-term mechanisms for support. Fee-for-service � this approach has been tested in the state of Washington but was not successful. Ongoing discussions with stakeholders indicate that most seem to favor a diversity of funding sources. The 1999 NVAC Report "Strategies to Sustain Success in Childhood Immunizations" stated that: "A stable funding mechanism for immunization registries needs to be developed that combines resources from the federal government, state and local governments, and the private sector." At the National Immunization Conference in July 2000, Secretary Donna Shalala said: "You can be assured that before I leave office, any authority I have through the Medicaid program or the Vaccines for Children programs to support these registries, any decision I can make, will be done before I leave in January. This is the critical piece that we need to put in place." With continuing 317 support and the addition of HCFA and VFC support there will be a clear government commitment to support operation of registries for publicly supported immunizations. Now it is time for the private sector to provide similar support for children cared for in the private sector. Recommendations:
Figure 1.
Figure 2.
Figure 3.
Figure 4.
|
|
Welcome Center | What's New | Publications | Contact Us CDC Home | Search | Health Topics A-Z Last updated: March 28, 2002 Centers for Disease Control
and Prevention |