Surfactant for meconium aspiration syndrome in full term/near
term infants
El Shahed AI, Dargaville P, Ohlsson A, Soll RF
Dates
Date edited: 08/06/2007
Date of last substantive update: 16/05/2007
Date of last minor update: 29/01/2007
Date next stage expected / /
Protocol first published: Issue 2, 2000
Review first published: Issue 2, 2000
Contact reviewer
Dr Amr I El Shahed
Fellow, Perinatal/Neonatal Fellowship Program
Paediatrics
Mount Sinai Hospital
Toronto
Ontario CANADA
M5G 1X5
E-mail: amrshahed@yahoo.com
Secondary address (home):
77 Elm Street
Toronto
Ontario CANADA
M5G 1H4
Telephone: + 416 979 7823Contribution of reviewers
Amr I El Shahed:
Updated the search for articles
Excerpted data
Reviewed results
Wrote text of reviewPeter Dargaville:
Performed the original search for articles
Excerpted data
Reviewed results
Edited text of review
Arne Ohlsson:
Updated the search for articles
Excerpted data
Reviewed results
Wrote text of review
Roger F. Soll:
Performed the original search for articles
Excerpted data
Reviewed results
Edited the text of updated review
Internal sources of support
Department of Paediatrics, Mount Sinai Hospital, Toronto, CANADA
External sources of support
NoneWhat's new
This is an update of the review "Surfactant for meconium aspiration syndrome in full term infants" published in The Cochrane Library, Issue 2, 2002 (Soll 2002).
The authorship of this review has been changed to: El Shahed AI, Dargaville P, Ohlsson A, Soll RF.Since this review was first published, two additional trials were identified.
The increase in sample size has allowed for greater precision for some of the treatment effects. Surfactant treatment does not appear to have an effect on mortality, but does reduce the need for treatment with extracorporeal membrane oxygenation (ECMO). Surfactant treatment may reduce respiratory related outcomes and hospital stay in term/near-term infants with meconium aspiration syndrome.
Dates
Date review re-formatted: / /
Date new studies sought but none found: / /
Date new studies found but not yet included/excluded: / /
Date new studies found and included/excluded: / /
Date reviewers' conclusions section amended: / /
Date comment/criticism added: / /
Date response to comment/criticisms added: / /
Text of review
Synopsis
The lungs of newborn babies' can be damaged by meconium aspiration syndrome. Meconium aspiration syndrome is caused when a stressed baby passes a bowel movement while still in the womb and then breathes some of this material into the lungs. Pulmonary surfactant, the complex combination of chemicals that line the surface of the lung, may be altered or inactivated in babies who have meconium aspiration. It is thought that treatment with additional surfactant might be able to help overcome this damage. This review of trials found that surfactant can reduce breathing difficulties and breathing failure in babies suffering from meconium aspiration syndrome.
Abstract
Background
Surfactant replacement therapy has been proven beneficial in the prevention and treatment of neonatal respiratory distress syndrome (RDS). The deficiency of surfactant or surfactant dysfunction may contribute to respiratory failure in a broader group of disorders, including meconium aspiration syndrome (MAS).
Objectives
To evaluate the effect of surfactant administration in the treatment of term/near-term infants with MAS.
Search strategy
Searches were made using The Cochrane Library (Issue 4, 2006), MEDLINE and EMBASE (1985 to December 2006), previous reviews including cross-references, abstracts, conference and symposia proceedings, expert informants, and journal hand searching. No language restrictions were applied. Authors were directly contacted to provide additional data.
Selection criteria
Randomised controlled trials which evaluated the effect of surfactant administration in term infants with meconium aspiration syndrome are included in the analyses.
Data collection & analysis
Data regarding clinical outcomes including mortality, treatment with extracorporeal membrane oxygenation (ECMO), pneumothorax, duration of assisted ventilation, duration of supplemental oxygen, intraventricular haemorrhage (any grade and severe IVH), and chronic lung disease, and were excerpted from the reports of the clinical trails by the review authors. Data analyses were done in accordance with the standards of the Cochrane Neonatal Review Group.
Main results
Four randomised controlled trials met inclusion criteria. The meta-analysis of 4 trials enrolling 326 infants showed no statistically significant effect on mortality (typical relative risk 0.98 (95% CI 0.41, 2.39), typical risk difference 0.00 (95% CI -0.05, 0.05). The risk of requiring extracorporeal membrane oxygenation was significantly reduced in a meta-analysis of two trials (n = 208); (typical relative risk 0.64, 95% CI 0.46, 0.91; typical risk difference -0.17, 95% CI -0.30, -0.04); number needed to treat to benefit 6 (95% CI 3, 25). One trial (n = 40) reported a statistically significant reduction in the length of hospital stay [mean difference - 8 days (95% CI -14, -3 days)]. There were no statistically significant reductions in any other outcomes studied (duration of assisted ventilation, duration of supplemental oxygen, pneumothorax, pulmonary interstitial emphysema, air leaks, chronic lung disease, need for oxygen at discharge or intraventricular haemorrhage).
Reviewers' conclusions
In infants with MAS, surfactant administration may reduce the severity of respiratory illness and decrease the number of infants with progressive respiratory failure requiring support with ECMO. The relative efficacy of surfactant therapy compared to, or in conjunction with, other approaches to treatment including inhaled nitric oxide, liquid ventilation, surfactant lavage and high frequency ventilation remains to be tested.
Background
The deficiency of surfactant or surfactant dysfunction may contribute to respiratory failure in a broad group of disorders, including meconium aspiration syndrome (MAS). Meconium inhibits the surface tension lowering properties of surfactant (Chen 1985; Moses 1991). Instillation of meconium into the airways of term animals leads to acute mechanical obstruction and worsening pulmonary mechanics and gas exchange (Chen 1985; Tran 1980; Tyler 1978). A significant reduction in lung compliance, an increase in expiratory lung resistance and increased functional residual capacity can be demonstrated (Tran 1980). Investigators have postulated that the changes in compliance associated with meconium aspiration result from displacement of surfactant by free fatty acids (Clark 1987). In animals with experimentally induced meconium aspiration, treatment with large doses of natural surfactant extract improves compliance and ventilation (Sun 1993).
Surfactant replacement therapy has been proven beneficial in the prevention and treatment of neonatal respiratory distress syndrome (RDS) (Soll 1992). Respiratory distress syndrome is due to a primary deficiency in the production and release of pulmonary surfactant. Surfactant therapy has been shown to improve oxygenation, decrease the need for ventilatory support, and improve clinical outcome in infants with RDS. Surfactant treated infants have a reduced mortality and a decreased incidence of pneumothorax.
Uncontrolled studies of surfactant treatment in infants with MAS suggest that surfactant may be of benefit in MAS. In a pilot study of 7 infants with MAS treated with surfactant, all 7 infants demonstrated an improvement in respiratory failure (Auten 1991). Khammash and coworkers (Khammash 1993) treated 20 infants with severe MAS. Infants received an intratracheal dose of bovine surfactant extract (100 mg phospholipid/kg). Improvement in oxygenation index (OI) and arterial/alveolar ratio (a/A pO2) was noted in 75% of the treated infants in the six hours following surfactant instillation. None of the treated infants required further experimental therapy including extracorporeal membrane oxygenation (ECMO).
Other approaches to prevent or treat MAS include amnioinfusion (infusion of saline into the amniotic cavity), oro/nasopharyngeal suctioning of meconium stained neonates before delivery and the use of surfactant lavage in infants with the diagnosis of MAS.
In a systematic review, Hofmeyr and coworkers (Hofmeyr 2002) found that amnioinfusion in women with meconium stained liquor was associated with improvements in perinatal outcomes including the occurrence of MAS, particularly in settings where facilities for perinatal surveillance were limited. However, in a recent large multicenter, international, randomised controlled trial of amnioinfusion to prevent MAS (not included in the Hofmeyr review), a benefit from amnioinfusion could not be confirmed (Fraser 2005). Unlike the previous systematic overview, the authors concluded that for women in labor who have thick meconium staining of the amniotic fluid, amnioinfusion did not reduce the risk of moderate or severe MAS, perinatal death, or other major maternal or neonatal disorders (Fraser 2005).
Vain and co-workers (Vain 2004) assessed the effectiveness of intrapartum suctioning for the prevention of MAS in a large multicenter randomised controlled trial. The primary outcome was the incidence of MAS. No significant difference between treatment groups was seen in the incidence of MAS, mortality, or in the duration of ventilation, oxygen treatment, and hospital care. The authors concluded that routine intrapartum oropharyngeal and nasopharyngeal suctioning of term-gestation infants born through meconium stained amniotic fluid does not prevent MAS. These findings led to change in clinical practice and routine suctioning of the oropharynx and the nasopharynx are currently not recommended (AAP 2006).
The following systematic review evaluates randomised controlled trials that studied the effect of surfactant administration for the treatment of term/near term infants with MAS. Studies which utilized dilute surfactant solutions to lavage meconium from the airways are not included in this review.
Objectives
To evaluate the effect of surfactant administration in the treatment of term or near term infants with meconium aspiration syndrome.
Criteria for considering studies for this review
Types of studies
Randomised controlled trials comparing surfactant treatment to routine management of term/near-term infants with MAS.
Types of participants
Term or near-term infants with MAS (modified from the previous review, which planned to include only term infants).
Types of interventions
Intratracheal administration of surfactant vs. placebo or no therapy. Studies that utilized dilute surfactant solutions to lavage meconium from the airways are not included in this review.
Types of outcome measures
For the update of this review, the following primary and secondary outcomes were selected:
PRIMARY OUTCOME:
Mortality
SECONDARY OUTCOMES:
1. Treatment with extracorporeal membrane oxygenation (ECMO)
2. Pneumothorax
3. Pulmonary interstitial emphysema
4. Air leaks (pneumothorax, pneumomediastinum, pulmonary interstitial emphysema)
5. Duration of assisted mechanical ventilation (days)
6. Duration of supplemental oxygen (days)
7. Need for supplemental oxygen at discharge
8. Chronic lung disease defined as need for oxygen therapy at 28 days or 36 weeks postmenstrual age
9. Intraventricular haemorrhage (any grade)
10. Severe IVH (grade III-IV)]
11. Duration of hospital stay (days).
Search strategy for identification of studies
The Cochrane Library (Issue 4, 2006) was searched in December 2006. A search was run in OVID MEDLINE (1966 to December 2006) using the following strategy: (exp Pulmonary Surfactants/ or surfactan:.mp. or Surface-Active Agents/ or (surfactan: adj2 lavage:).mp.) and (Meconium Aspiration Syndrome/ or Meconium/). A search was run in OVID EMBASE <1980 to 2006 Week 06>using the following strategy: (Lung Surfactant/ or exp Surfactant/ or (surfactan: adj2 lavage:).mp. or surfactan:.mp.) and (Meconium or Aspiration/ or meconium/).
Previous reviews including cross references were searched. Abstracts published in Pediatric Research or electronically from Pediatric Academic Societies meetings were searched from 2000 to December 2006. No language restrictions were applied.
Methods of the review
For each included study, information was collected regarding the method of randomisation, blinding, drug intervention, stratification, and whether the trial was single or multicenter. Information regarding trial participants including gestational age criteria, birth weight criteria, cause of respiratory failure, severity of respiratory failure, and postnatal age at the time of treatment was noted. Information on clinical outcome was extracted including mortality, treatment with ECMO, pneumothorax, pulmonary interstitial emphysema, chronic lung disease, duration of assisted ventilation, duration of supplemental oxygen, need for supplemental oxygen at discharge, duration of hospital stay, intraventricular haemorrhage (any grade and grades III and IV). Investigators or study sponsors were contacted for clarification or provision of data not specifically noted in the original report. For this update two review authors (AS, AO) independently evaluated all studies, abstracted the data on abstraction forms and compared the abstracted data and achieved agreement. One review author (AS) entered the data into RevMan 4.2.9 and the other review author (AO) checked the data for accuracy. Unpublished information on the subgroup of infants with MAS obtained from Lotze at al (Lotze 1998) included in the original review were entered unchanged. Unpublished information regarding the multicenter trial conducted in Chile and previously published in abstract form was obtained from the authors (Maturana 2005).
The quality of included trials was evaluated independently by the review authors using the following criteria:
Blinding of randomisation
Blinding of intervention
Blinding of outcome measure assessment
Completeness of follow up
There are three potential answers to these questions: yes, no, cannot tell.
The statistical methods included (typical) relative risk (RR), risk difference (RD), number needed to treat to benefit (NNTB) or number needed to treat to harm (NNTH) for dichotomous outcomes and weighed mean difference (WMD) reported with 95% confidence intervals (CI). A fixed effects model was used for meta-analysis. Heterogeneity was assessed using the I squared (I2) statistic.
Description of studies
For details see the Table 'Characteristics of included studies'.
Studies included in this review:
The study by Findlay and coworkers was a single centre study performed in the USA (Findlay 1996):
- Objective: To determine whether high-dose surfactant therapy improves the pulmonary morbidity of term infants ventilated for MAS.
- Population: Term newborn infants with MAS diagnosed by the presence of meconium below the vocal cords at birth and /or characteristic chest radiographic findings who needed ventilator support before six hours of age with a fractional inspired oxygen (Fi02 ) level of 0.5 or more, mean airway pressure of 7 cm of H2O or more and a/A pO2 ratio of 0.22 or less.
- Intervention: Infants in the study group received up to four doses of 150 mg (6ml)/kg beractant (Survanta), installed every 6 hours by continuous infusion for 20 minutes via a side hole endotracheal tube adapter. Infants in the control group received 6 ml/kg air placebo.
- Outcomes: Primary outcomes included decrease in Oxygen Index (OI), increase in a/A pO2 ratio and decrease in the need for respiratory support [mean airway pressure (MAP), ventilation days]. Secondary outcomes included the need for ECMO, incidence of air leaks, duration of oxygen therapy, discharge with supplemental oxygen, and mortality at less than 28 days of life.
The study by Lotze and coworkers was a multicenter study performed in the USA (Lotze 1998):
- Objective: To determine whether surfactant (beractant) administration to term newborns in respiratory failure and at risk for requiring ECMO treatment would significantly reduce the incidence of severe complications through 28 days of age and the need for ECMO.
- Population: Infants weighing 2000 g or more with gestational ages of 36 weeks or greater with respiratory failure secondary to MAS, sepsis or idiopathic persistent pulmonary hypertension of newborn (requiring FiO2 1.00 with OI of 15 - 39).
- Intervention: Infants were randomly assigned to receive either four doses of beractant 100 mg/kg or air placebo before ECMO treatment and four additional doses during ECMO, if ECMO was required (only infants with MAS are included in this analysis and the data were provided by the authors).
- Outcomes: Need for ECMO and incidence of severe complications (haemorraghic, neurologic, pulmonary, renal, cardiovascular, infectious, metabolic and technical) during the first 28 days of age or at discharge.
The Chinese Collaborative Study was a multicenter study performed in China (Chinese Collab. 2005):
- Objective: To evaluate the safety and efficacy of exogenous surfactant replacement therapy for MAS in term and near-term neonates.
- Population: Term and near term neonates with MAS (diagnosis based on the presence of meconium in the airways and/or meconium-stained amniotic fluid at delivery, typical chest X-ray findings, onset of respiratory distress, and abnormal blood gas findings indicating respiratory failure and acidosis), birth weight > 2500 g, postnatal age < 36 h, a/A pO2 ratio < 0.22, OI >15 and need for mechanical ventilation for 1 - 2 h without improvement.
- Intervention: The infants in the surfactant group received an initial dose of porcine lung derived surfactant (Curosurf) at 200 mg/kg, and repeated doses of 200, 100 and 100 mg/kg were given at 6 - 12 h intervals to a maximum of four doses if OI increased by > 2 from baseline. The control group received the standard of care without a placebo.
- Outcomes: The primary outcomes were a reduction of OI to less than 10 and an increase of the pre-treatment a/A pO2 ratio of 100% over baseline 24 h after surfactant treatment. The secondary outcomes were duration of mechanical ventilation, incidence of complications and survival to discharge from hospital.
The study by Maturana and coworkers was a multicenter study performed in Chile (Maturana 2005):
- Objective: To evaluate if the use of up to 3 doses of surfactant administered as a bolus (150 mg/kg) versus placebo, reduces the number of days on mechanical ventilation in term infants with moderate to severe meconium aspiration syndrome.
- Population: Term newborns > 37 weeks of gestation with moderate to severe MAS (defined as the presence of meconium stained amniotic fluid and/or evidence of meconium in the lower airway, abnormal x-ray consistent with MAS and respiratory insufficiency defined as an oxygen requirement of > 50% in oxyhood to achieve saturation of > 90% or PaO2 > 50 mmHg if the patient was not ventilated, or an OI > 8 if the patient was on mechanical ventilation.
- Intervention: Infants were randomly assigned to receive either 150 mg /kg/dose (6ml) of Survanta or an equivalent amount of air as placebo every six hours for total of three doses if they remained intubated.
- Outcomes: The primary outcome was days on mechanical ventilation. Secondary outcomes included days requiring oxygen therapy with a target arterial oxygen saturation > 90%, air leaks (pneumothorax, pneumomediastinum, interstitial emphysema), persistent pulmonary hypertension (PPHN), OI after two hours following the first treatment dose and mortality before discharge.
Methodological quality of included studies
Randomised controlled trials that evaluated the effect of bolus surfactant administration in term or near term infants with MAS are included in the analysis. Specific methodologic issues are discussed below:
Randomisation: The four included studies allocated treatments by randomisation. The Collaborative Chinese Study (Chinese Collab. 2005) and Maturana (Maturana 2005) used sealed randomisation envelopes. Findlay (Findlay 1996) did not report on the method of randomisation, but stated that physicians and nurses caring for the infants were unaware of the infants' assignment groups. Lotze (Lotze 1998) used a central randomizations service and stratified infants by primary diagnosis and disease severity.
Blinding of treatment: In the study of Findlay and co-workers (Findlay 1996) the attending staff were unaware of treatment assignment. In the study by Lotze (Lotze 1998), the dosing investigator was prohibited from participating in any other aspects of infants' care and from revealing the treatment assignment. In the Chinese Collaborative Study (Chinese Collab. 2005), staff were not blinded to treatment groups. In the study by Maturana (Maturana 2005), the assigned treatment was administered by a person not involved in the direct patient care and was given behind a screen. The number of infants enrolled in the trial differed in the published abstract (Maturana 2005) and in the information obtained from the first author (three additional infants in the surfactant group and one additional infant in the control group). Differences noted between abstracts and full reports may indicate elements of bias/poor data quality control possibly including any of the following methodological issues: multiple looks at the data; changes in the definitions of outcomes; no preset sample size; closure of patient recruitment when statistical significance has been reached for the outcome under study and other sources of bias (Walia 1999).
Blinding of outcome assessment: Outcomes were assessed by staff members unaware of treatment assignment in three of the four studies (Findlay 1996; Lotze 1998; Maturana 2005).
Exclusion after randomisation: There were no exclusions after randomisation reported in any of the studies.
Results
SURFACTANT THERAPY VS. PLACEBO OR NO TREATMENT (COMPARISON 01):
PRIMARY OUTCOME:
Mortality (Outcome 01.01):
All four studies enrolling 326 infants reported on mortality (Outcome Table 01.01). Surfactant had no statistically significant effect on mortality [typical RR 0.98 (95% CI 0.41, 2.39); typical RD 0.00 (95% CI -0.05, 0.05)]. Heterogeneity of treatment effect for this outcome was low (I2 = 0 %).
SECONDARY OUTCOMES:
Treatment with ECMO (Outcome 01.02):
Two studies enrolling 208 patients reported on treatment with ECMO (Outcome Table 01.02). Surfactant statistically significantly reduced treatment with ECMO [typical RR 0.64 (95% CI 0.46, 0.91); typical RD -0.17 (95% CI -0.30, -0.04); NNT 6 (95% CI 3, 25). Heterogeneity of treatment effect for this outcome was moderate for RR (I2 = 50.4%) and low for RD (I2 = 0%)]
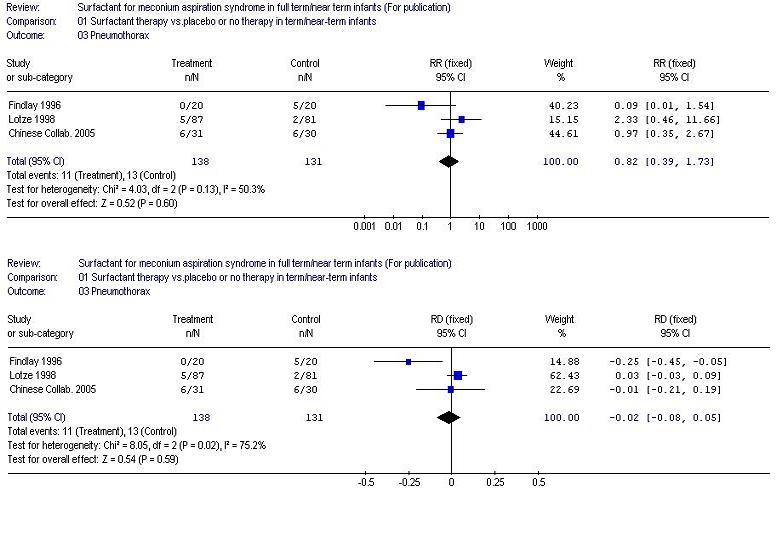
Pneumothorax (Outcome 01.03):
Three studies enrolling 269 infants reported on the occurrence of pneumothorax (Outcome Table 01.03). Surfactant did not statistically significantly reduce the occurrence of pneumothorax [typical RR 0.82 (95% CI 0.39, 1.73); typical RD -0.02 (95% CI -0.08, 0.05)]. Heterogeneity of treatment effect for this outcome was moderate for RR (I2 = 50.3%) and large for RD (I2 = 75.2%).
Pulmonary interstitial emphysema (Outcome 01.04):
One study enrolling 61 infants reported on the occurrence of interstitial emphysema (Outcome Table 01.04). Surfactant had no statistically significant effect on pulmonary interstitial emphysema [RR 0.55 (95% CI 0.18, 1.70); RD -0.10 (95% CI -0.30, 0.09)]. Tests for heterogeneity were not applicable.
Air leaks (pneumothorax, pneumomediastinum, interstitial emphysema) (Outcome 01.05):
One study enrolling 57 infants reported on a combination of air leaks (Outcome Table 01.05). Surfactant did not have a statistically significant effect on air leaks [RR 1.04 (95% CI 0.23, 4.71); RD 0.00 (95% CI -0.16, 0.16). Tests for heterogeneity were not applicable.
Duration of assisted mechanical ventilation (days) (Outcome 01.06):
Three studies enrolling 158 infants reported on duration of assisted mechanical ventilation (Outcome Table 01.06). Mechanical ventilated was stated as the outcome in all three studies, but if this included continuous positive airway pressure was not indicted. Surfactant had no statistically significant effect on the duration of assisted ventilation [WMD 0.60 days ( -0.41, 1.62)]. Heterogeneity of treatment effect for this outcome was moderate (I2 = 72.6%).
Duration of supplemental oxygen (days) (Outcome 01.07):
Two studies reported on duration of supplemental oxygen (Outcome Table 01.07). Surfactant did not statistically significantly reduce the duration of supplemental oxygen [WMD 0.40 (95% CI -2.83, 3.64). Heterogeneity of treatment effect for this outcome was large (I2 = 87.8%).
Need for supplemental oxygen at discharge (Outcome 01.08):
One study enrolling 40 infants reported on the need for oxygen at discharge (Outcome Table 01.08). Surfactant had no statistically significant effect on need for supplemental oxygen at discharge [RR 0.75 (95% CI 0.32, 1.77) RD -0.10 (95% CI -0.39, 0.19). Tests for heterogeneity were not applicable.
Chronic lung disease (age at diagnosis not stated) (Outcome 01.09):
One study enrolling 168 infants reported on chronic lung disease (Outcome Table 01.05). Surfactant had no statistically significant effect on chronic lung disease [RR 0.47 (95% CI 0.12, 1.80); RD -0.04 (95% CI -0.11, 0.03)]. Tests for heterogeneity not applicable.
Intraventricular haemorrhage (any grade) (Outcome 01.10):
Two studies enrolling 229 infants reported on the incidence of intraventricular haemorrhage (any grade) (Outcome Table 01.10). Surfactant had no statistically significant effect on intraventricular haemorrhage (any grade) [typical RR 0.67 (95% CI 0.31, 1.46); typical RD -0.04 (95% CI -0.12, 0.04)]. Heterogeneity of treatment effect for this outcome was moderate (RR, I2 = 47.5%; RD, I2 = 50.8%)].
Severe intraventricular haemorrhage (grades III and IV) (Outcome 01.11):
One study enrolling 168 infants reported on the incidence of severe intraventricular haemorrhage (grades III and IV) (Outcome table 01.11). Surfactant had no statistically significant effect on severe intraventricular haemorrhage (grades III and IV) [RR 2.79 (95% CI 0.30, 26.31); RD 0.02 (95% CI -0.02, 0.07).Tests for heterogeneity were not applicable.
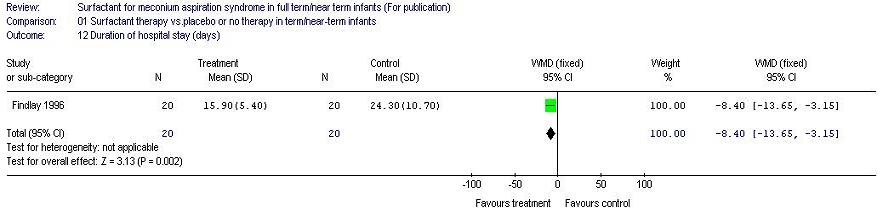
Duration of hospital stay (days) (Outcome 01.12):
One study enrolling 40 infants reported on the duration of hospital stay. Surfactant statistically significantly reduced the duration of hospital stay [MD -8 days (95% CI -14, -3)]. Tests for heterogeneity were not applicable.
Discussion
Deficiency and/or dysfunction of pulmonary surfactant may contribute to respiratory failure in a broad group of disorders including pneumonia, MAS, and adult respiratory distress syndrome. Four randomised controlled trials were identified that studied the effect of surfactant therapy in term/near-term infants with MAS. Three of the studies were placebo controlled using air as the placebo and in these three studies the outcomes were assessed blinded to group of allocation (Findlay 1996; Lotze 1998,Maturana 2005). In the fourth study, the clinical staff were not blinded to group allocation (Chinese Collab. 2005). The sample sizes of the studies were small with 40, 57, 61, and 168 infants enrolled (Findlay 1996; Maturana 2005; Chinese Collab. 2005; Lotze 1998). The number of infants enrolled in the study by Maturana and coworkers differed in the published abstract (Maturana 2005) and in the information obtained from the author. There were four more infants included in the report that we obtained from the authors.
Surfactant treatment did not have a statistically significant effect on the primary outcome of mortality. In the meta-analysis of the results from two studies (Findlay 1996; Lotze 1998), surfactant treatment resulted in a statistically and clinically important reduction in the need for ECMO treatment with a NNTB of 6 (95% CI 3, 25). ECMO treatment was not available for the units in the Chinese Collaborative study (Chinese Collab. 2005) nor in the study from Chile (Maturana 2005). The one study (Findlay 1996) that reported on duration of hospital stay reported a reduction in hospital days. There were no other statistically significant reductions in any of the other important clinical outcomes (duration of assisted ventilation, duration of supplemental oxygen, air leaks, chronic lung disease, duration of assisted ventilation, need for supplemental oxygen at discharge and intraventricular haemorrhage). The trends for all respiratory tract associated outcomes favoured the use of surfactant.
A number of investigators have attempted to treat meconium aspiration syndrome with diluted surfactant solutions used as a lavage to wash residual meconium from the airway (Ibara 1995; Ogawa 1996; Lam 1999). Wiswell and coworkers (Wiswell 2002) enrolled twenty-two infants [15 surfactant (Surfaxin) and 7 control]. There were non-significant trends for surfactant-lavaged infants to be weaned from mechanical ventilation earlier (mean of 6.3 vs 9.9 days, respectively), as well as to have a more rapid decline in their OI compared with control infants. The authors concluded that dilute Surfaxin lavage seemed a safe and potentially effective therapy in the treatment of MAS. The data support future prospective, controlled clinical trials of bronchoalveolar lavage with surfactant in neonates with MAS.
Current evidence indicates that amnioinfusion prior to birth or suctioning of the oropharynx/nasopharynx prior to the delivery of the shoulders do not prevent MAS from occurring. At the present time, the two most promising interventions appear to be treatment with surfactant or surfactant lavage. As few infants have been studied to date further research is warranted possibly using a three armed trial with 1) surfactant administration, 2) surfactant lavage and 3) a control group receiving air.
Clinical experience indicates that persistent pulmonary hypertension of the newborn (PPHN) is one of the major causes of death in infants with MAS (Hsieh 2004). There is evidence that meconium injury may directly trigger postnatal release of vasoconstrictors such as ET-1, TXA2, and prostaglandin E2 (PGE2), which play a role in development of pulmonary hypertension (Soukka 1998).
Infants with MAS and PPHN are usually treated with oxygen, conventional and/or high frequency mechanical ventilation, inotropic support, induction of alkalosis, and sedation. When these measures fail, ECMO has been shown to improve the outcome (UK Collab 1996). Inhaled NO is frequently used for the treatment of newborns with severe pulmonary hypertension and respiratory failure. Consequently, increasing clinical and experimental evidence suggest that exogenous NO, given by inhalation, selectively reduces pulmonary vasoconstriction and improves oxygenation in a variety of pathological conditions of the newborn lungs, including meconium aspiration (Neonatal iNO 1997; Van Meurs 2003). In recent experimental data, Aaltonen (Aaltonen 2007) demonstrated that iNO in MAS is associated with diminished pulmonary hypertensive response as well as decreased DNA oxidation and neuronal damage in hippocampal tissue that may potentially have significant adverse long-term effects on the developmental status of the affected newborns.
ECMO procedures are complex because they require systemic anticoagulation and major vessel cannulation. Studies on inhaled nitric oxide (iNO) therapy for PPHN have shown rapid improvement in oxygenation, reducing the need for ECMO therapy without affecting the mortality (Christou 2000; Clark 2000). Finer and Barrington (Finer 2000) showed that iNO treatment improves oxygenation in approximately 50% of term or near-term neonates with hypoxemic respiratory failure and reduces the combined end point of death or the need for ECMO therapy (relative risk, 0.73) as compared with control subjects. However, lack of an early response to iNO treatment within a few hours in patients who are referred for ECMO therapy and younger age at the time of presentation may indicate the need for ECMO therapy in at least 50% of patients with hypoxic respiratory failure (Fakioglu 2005).
Reviewers' conclusions
Implications for practice
The results of this systematic review provides some support for the use of surfactant treatment in MAS. In infants with MAS leading to moderate to severe respiratory failure, surfactant administration will decrease the number of infants treated with extracorporeal membrane oxygenation. This may have implications especially in resource poor settings where ECMO is not available. In the only study reporting on the duration of hospital stay, this outcomes was significantly reduced.
Implications for research
Although surfactant therapy may be of use in severe meconium aspiration syndrome, the efficacy of surfactant therapy compared to other approaches including inhaled nitric oxide, liquid ventilation, and high frequency ventilation remains to be tested. Other approaches to surfactant therapy, including the use of surfactant lavage, may prove to be effective in the treatment of MAS. Trials that compare surfactant treatment to surfactant lavage and air (control) would be appropriate. The findings of this review need to be confirmed in randomised controlled trials of appropriate size.
Acknowledgements
For the original review we would like to thank Ms. Elizabeth Zola, PharmD for providing diagnosis specific data from the Survanta in Term Infants Study Group. For the updated review, we thank Dr. Andres Maturana for providing us with unpublished data from his study previously published in abstract form only. For the update of this review we thank Ms. Elizabeth Uleryk, Chief Librarian, the Hospital for Sick Children, Toronto, Ontario, Canada, for developing the search strategy for the literature retrieval.
Potential conflict of interest
Dr. R. Soll has acted as a consultant and invited speaker for several of the pharmaceutical companies which manufacture or distribute surfactant preparations (Abbott Laboratories, Ross Laboratories, Chiesi Pharmaceuticals, Dey Laboratories, Burroughs Wellcome). Dr. P. Dargaville has received support for basic science research in surfactant lavage studies from Abbott Australasia. Neither Dr. El Shahed nor Dr. Ohlsson have conflicts of interest to disclose.
Characteristics of included
studies
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Chinese Collab. 2005 | Multicenter
Blinding of randomizations: Yes
Blinding of treatment: No
Complete follow-up: Yes
Blinding of outcome measure: No | Term and near term neonates with MAS, BW > 2500 g, postnatal age <36 h, a/A pO2 ratio <0.22, OI >15 and needed mechanical ventilation for 1-2 h without improvement.
No lethal congenital anomalies, IVH grade II-IV, Apgar score <3 at 10 min or clinically unstable.
| The treatment group (n = 87) received modified bovine surfactant extract (Survanta, 100 mg/kg) or air placebo (up to 4 doses prior to ECMO and 4 additional doses if ECMO was required)
The control group (n = 81) received air placebo | PRIMARY: Reduction of OI to less than 10 and an increase of the pre-treatment a/A pO2 ratio of 100% over baseline 24 h after surfactant treatment
SECONDARY: Duration of mechanical ventilation, incidence of complications and survival to discharge from hospital. | | A |
| Findlay 1996 | Single center
Blinding of randomizations: Yes
Blinding of treatment: Yes
Complete Follow-up: Yes
Blinding of outcome measure: Yes | Term infants with MAS, requiring assisted ventilation, supplemental oxygen >50%, MAP >7cm H20, a/A pO2 ratio <0.22, age <6 hrs
and no major congenital anomaly | The treatment group (n = 20) received modified bovine surfactant extract (Survanta 150 mg/kg), repeated at 6 hr intervals for a maximum of 4 doses, infused intratracheally via a side port adaptor over 20 minutes
The control group (n = 20) received air placebo | PRIMARY: Improvement in OI, improvement in a/A pO2 ratio
SECONDARY: Pneumothorax, need for ECMO, duration of assisted ventilation, duration of oxygen therapy, mortality | | A |
| Lotze 1998 | Multicenter
Blinding of randomization: Yes (central randomization)
Blinding of treatment: Yes (dosing investigators)
Complete follow-up: Yes
Blinding of outcome measurement: YesStratification: primary diagnosis disease severity (oxygenation index) | Infants >2000 g, gestational age >36 wks, age <120 hours with MAS, PPHN or sepsis and severe respiratory failure but without any major congenital anomalies or IVH > Grade I | The treatment group (n = 87) received modified bovine surfactant extract (Survanta, 100 mg/kg) or air placebo (up to 4 doses prior to ECMO and 4 additional doses if ECMO was required)
The control group (n = 81) received air placebo | PRIMARY: Need for ECMO, severe complications, mortality
| Only infants with MAS are included in this review
Data for this group were obtained by the authors of the first version of this review | A |
| Maturana 2005 | Multicenter (13 centers)
Blinding of randomizations: Yes
Blinding of treatment: Yes
Complete follow-up: Yes
Blinding of outcome measure: Yes
| Term infants > 37 weeks of gestation with moderate to severe MAS and respiratory insufficiency within the first 12 hours after birth | The treatment group (n = 28) received 150 mg /kg/dose (6ml) of Survanta every 6 hours for a total of three doses if they remained intubated
The control group (n = 29) received an equivalant amount of air as placebo | PRIMARY: Days of mechanical ventilation
SECONDARY: Days requiring oxygen therapy with a target arterial oxygen saturation > 90%, air leaks, PPHN, OI 2 hours after the first treatment dose and mortality before discharge | | A |
a/A pO2 ratio = arterial-to alveolar oxygen tension ratio
BW = birth weight
IVH = Intraventricular hemorrhage
MAS = meconium aspiration syndrome
OI = oxyggen index
PPHN = persistent pulmonary hypertension of the neonateCharacteristics of excluded studies
| Study | Reason for exclusion |
| Auten 1991 | Sequential case study; no control group |
| Blanke 1993 | Not randomized, no control group |
| Diniz 1995 | Not randomized |
| Halliday 1996 | Retrospective, not randomized |
| Ibara 1995 | Saline lavage and surfactant replacement, not randomized |
| Khammash 1993 | Sequential case study; no control group |
| Lam 1999 | Not randomized, historical controls, surfactant used as lavage |
| Nakamura 2000 | A randomized trial conducted in piglets |
| Ogawa 1996 | Surfactant lavage |
| Wiswell 2002 | Surfactant lavage |
References to studies
References to included studies
Chinese Collab. 2005 {published data only}Chinese Collaborative Study Group for Neonatal Respiratory Diseases. Treatment of severe meconium aspiration with porcine surfactant: a multicentre, randomized, controlled trial. Acta Paediatrica 2005;94:896-902.
Findlay 1996 {published data only}
Findlay RD, Taeusch HW, Walther FJ. Surfactant replacement therapy for meconium aspiration syndrome. Pediatrics 1996;97:48-52.
Lotze 1998 {published data only}
Lotze A, Mitchell BR, Bulas DI, Zola EM, Shalwitz RA, Gunkel HJ, et al. Multicenter study of surfactant (beractant) use in the treatment of term infants with severe respiratory failure. Journal of Pediatrics 1998;132:40-7.
Maturana 2005 {unpublished data only}
Maturana A, Torres-Pereyra J, Salinas R, Astudillo P, Moya FR, The Chile Surf Group. A randomized trial of natural surfactant for moderate to severe meconium aspiration syndrome. In: PAS2005:57:1545.
References to excluded studies
Auten 1991 {published data only}Auten RL, Notter RH, Kendig, JW, Davis JM, Shapiro DL. Surfactant treatment of full-term newborns with respiratory failure. Pediatrics 1991;87:101-7.
Blanke 1993 {published data only}
Blanke JG, Jorch G. Surfactanttherapie bei 10 Neugeborenem mit Mekoniumaspirationssyndrom [Surfactant therapy in severe neonatal respiratory failure - multicenter study - II. Surfactant therapy in 10 newborn infants with meconium aspiration syndrom]. Klinische Padiatrie 1993;205:75-8.
Diniz 1995 {published data only}
Diniz EMA, Fiori RM. Curosurf therapy in severe meconium aspiration (MAS). Biology of the Neonate 1995;67:86.
Halliday 1996 {published data only}
Halliday HL, Speer CP, Robertson B. Treatment of severe meconium aspiration syndrome with porcine surfactant. European Journal of Pediatrics 1996;155:1047-51.
Ibara 1995 {published data only}
Ibara S, Ikenoue T, Murata Y, Sakamoto H, Saito T, Nakamura Y et al. Management of meconium aspiration syndrome by tracheobronchial lavage and replacement of surfactant -TA. Acta Paediatrica Japonica 1995;37:64-7.
Khammash 1993 {published data only}
Khammash H, Perlman M, Wojtulewicz J, Dunn M. Surfactant therapy in full-term neonates with severe respiratory failure. Pediatrics 1993;92:135-9.
Lam 1999 {published data only}
Lam BCC, Yeung CY. Surfactant lavage for meconium aspiration syndrome: a pilot study. Pediatrics 1999;103:1014-8.
Nakamura 2000 {published data only}
Nakamura T, Matsuzawa S, Sugiura M, Tamura M. A randomised control study of partial liquid ventilation after airway lavage with exogenous surfactant in a meconium aspiration syndrome animal model. Archives of Disease in Childhood. Fetal and Neonatal Edition 2000;82:F160-2.
Ogawa 1996 {published data only}
Ogawa Y, Ohara Y, Itakura Y, et al. Bronchial lavage with surfactant solution for the treatment of meconium aspiration syndrome. J Jpn Med Soc Biol Interface 1996;26(Suppl):179-87.
Wiswell 2002 {published data only}
Wiswell TE, Knight GR, Finer NN, Donn SM, Desai H, Walsh WF. A multicenter, randomized, controlled trial comparing surfaxin (lucinactant) lavage with standard care for treatment of meconium apsiration syndrome. Pediatrics 2002;109:1081-7.
* indicates the primary reference for the study
Other references
Additional references
Aaltonen 2007Aaltonen M, Soukka H, Halkola L, Jalonen J, Kalimo H, Holopainen IE. Inhaled nitric oxide treatment inhibits neuronal injury after meconium aspiration in piglets. Early Human Development 2007;83:77-85.
AAP 2006
American Academy of Pediatrics, American Heart Association. Textbook of neonatal resuscitation. 5th edition. Elk Grove Village: American Academy of Pediatrics, American Heart Association, 2006.
Chen 1985
Chen CT, Toung TJK, Rogers MC. Effect of intra-alveolar meconium on pulmonary surface tension properties. Critical Care Medicine 1985;13:233-6.
Christou 2000
Christou H, Van Marter LJ, Wessel DL, Allred EN, Kane JW, Thompson JE. Inhaled nitric oxide reduces the need for extracorporeal membrane oxygenation in infants with persistent pulmonary hypertension of the newborn. Critical Care Medicine 2000;28:3722-7.
Clark 1987
Clark DA, Nieman GF, Thompson JE, Paskanik AM, Rokhar JE, Bredenberg CE. Surfactant displacement by meconium free fatty acids: An alternative explanation for atelectasis in meconium aspiration syndrome. Journal of Pediatrics 1987;110:765-70.
Clark 2000
Clark RH, Kueser TJ, Walker MW, Southgate WM, Huckaby JL, Perez JA. Low-dose nitric oxide therapy for persistent pulmonary hypertension of the newborn. New England Journal of Medicine 2000;342:469-74.
Fakioglu 2005
Fakioglu H, Totapally BR, Torbati D, Raszynski A, Sussmane JB, Wolfsdorf J. Hypoxic respiratory failure in term newborns: clinical indicators for inhaled nitric oxide and extracorporeal membrane oxygenation therapy. Journal of Critical Care 2005;20:288-93.
Finer 2000
Finer NN, Barrington KJ. Nitric oxide therapy for the newborn infant. Seminars in Perinatology 2000;24:59-65.
Fraser 2005
Fraser WD, Hofmeyr J, Lede R, Faron G, Alexander S, Goffinet F, et al. Amnioinfusion for the prevention of the meconium aspiration syndrome. New England Journal of Medicine 2005;353:909-17.
Hofmeyr 2002
Hofmeyr GJ. Amnioinfusion for meconium-stained liquor in labour. In: Cochrane Database of Systematic Reviews, Issue 1, 2002.
Hsieh 2004
Hsieh TK, Su BH, Chen AC, Lin TW, Tsai CH, Lin HC. Risk factors of meconium aspiration syndrome developing into persistent pulmonary hypertension of newborn. Acta Paediatrica Taiwan 2004;45:203-7.
Moses 1991
Moses D, Holm BA, Spitale P, Liu M, Enhorning G. Inhibition of pulmonary surfactant function by meconium. American Journal of Obstetrics and Gynecology 1991;164:477-81.
Neonatal iNO 1997
The Neonatal Inhaled Nitric Oxide Study Group. Inhaled nitric oxide in full-term and nearly full-term infants with hypoxic respiratory failure. New England Journal of Medicine 1997;336:597-604.
Soll 1992
Soll RF, McQueen MC. Respiratory Distress Syndrome.. In: Sinclair JC, Bracken MB (eds), editor(s). Effective Care of the Newborn Infant. Oxford: Oxford University Press, 1992.
Soukka 1998
Soukka H, Jalonen J, Kero P, Kaapa P. Endothelin-1, arterial natriuretic peptide and pathophysiology of pulmonary hypertension in porcine meconium aspiration. Acta Paediatrica 1998;87:424-8.
Sun 1993
Sun B, Curstedt T, Song GW, Robertson B. Surfactant improves lung function and morphology in newborn rabbits with meconium aspiration. Biolology of the Neonate 1993;63:96-104.
Tran 1980
Tran N, Lowe C, Sivieri EM, Shaffer TH. Sequential effects of acute meconium obstruction on pulmonary function. Pediatric Research 1980;14:34-8.
Tyler 1978
Tyler DC, Murphy J, Cheney FW. Mechanical and chemical damage to lung tissue caused by meconium aspiration. Pediatrics 1978;62:454-9.
UK Collab 1996
UK Collaborative ECMO Trail Group. UK collaborative randomized trial of neonatal extracorporeal membrane oxygenation. Lancet 1996;348:75-82.
Vain 2004
Vain NE, Szyld EG, Prudent LM, Wiswell TE, Aguilar AM, Vivas NI. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neoantes before delivery of their shoulders: multicentre, randomised controlled trial. Lancet 2004;364:597-602.
Van Meurs 2003
Van Meurs K, Rhine WD, Benitz WE. Meconium staining and the meconium aspiration syndrome. In: Fetal and neonatal brain injury. Mechanisms, management and the risks of practice. 2003:636-62.
Walia 1999
Walia R, Ohlsson A. Differences between information provided in abstracts of randomized controlled trials in neonates submitted to the Annual Meeting of the American Pediatric Society and the Society for Pediatric Research (APS/SPR) and final publications - implications for meta-analyses. In: 7th Annual Cochrane Colloquium Abstracts. 1999.
Other published versions of this review
Soll 2000Soll RF, Dargaville P. Surfactant for meconium aspiration syndrome in full term infants. In: Cochrane Database of Systematic Reviews, Issue 2, 2000.
Comparisons and data
| Comparison or outcome |
Studies |
Participants |
Statistical method |
Effect size |
| 01 Surfactant therapy vs.placebo or no therapy
in term/near-term infants |
| 01 Mortality |
4 |
326 |
RR (fixed), 95% CI |
0.98 [0.41, 2.39] |
| 02 Treatment with ECMO |
2 |
208 |
RR (fixed), 95% CI |
0.64 [0.46, 0.91] |
| 03 Pneumothorax |
3 |
269 |
RR (fixed), 95% CI |
0.82 [0.39, 1.73] |
| 04 Pulmonary interstitial emphysema |
1 |
61 |
RR (fixed), 95% CI |
0.55 [0.18, 1.70] |
| 05 Air leaks (pneumothorax, pneumomediastinum, interstitial
emphysema) |
1 |
57 |
RR (fixed), 95% CI |
1.04 [0.23, 4.71] |
| 06 Duration of assisted mechanical ventilation (days) |
3 |
158 |
WMD (fixed), 95% CI |
0.60 [-0.41, 1.62] |
| 07 Duration of supplemental oxygen (days) |
2 |
97 |
WMD (fixed), 95% CI |
0.40 [-2.83, 3.64] |
| 08 Need for supplemental oxygen at discharge |
1 |
40 |
RR (fixed), 95% CI |
0.75 [0.32, 1.77] |
| 09 Chronic lung disease (age at diagnosis not stated) |
1 |
168 |
RR (fixed), 95% CI |
0.47 [0.12, 1.80] |
| 10 Intraventricular hemorrhage (any grade) |
2 |
229 |
RR (fixed), 95% CI |
0.67 [0.31, 1.46] |
| 11 Severe intraventricular hemorrhage |
1 |
168 |
RR (fixed), 95% CI |
2.79 [0.30, 26.31] |
| 12 Duration of hospital stay (days) |
1 |
40 |
WMD (fixed), 95% CI |
-8.40 [-13.65, -3.15] |
01 Surfactant therapy vs.placebo or no therapy in term/near-term infants
01.01 Mortality
01.02 Treatment with ECMO
01.03 Pneumothorax
01.04 Pulmonary interstitial emphysema
01.05 Air leaks (pneumothorax, pneumomediastinum,
interstitial emphysema)
01.06 Duration of assisted mechanical ventilation
(days)
01.07 Duration of supplemental oxygen (days)
01.08 Need for supplemental oxygen at discharge
01.09 Chronic lung disease (age at diagnosis not
stated)
01.10 Intraventricular hemorrhage (any grade)
01.11 Severe intraventricular hemorrhage
01.12 Duration of hospital stay (days)
Contact details for co-reviewers
Dr Peter A. Dargaville, MBBS FRACP MD
Neonatologist
Department of Paediatrics
Royal Hobart Hospital
Liverpool Street
Hobart
Tasmania AUSTRALIA
7000
Telephone 1: +61 3 62228308
Facsimile: +61 3 62264864
E-mail: peter.dargaville@dhhs.tas.gov.au
Dr Arne Ohlsson
Director Evidence Based Neonatal Care and Outcomes Research
Department of Paediatrics
Mount Sinai Hospital
600 University Avenue
Toronto
Ontario CANADA
M5G 1X5
Telephone 1: +1 416 586 8379
Telephone 2: +1 416 341 0444
Facsimile: +1 416 586 8745
E-mail: aohlsson@mtsinai.on.ca
Dr Roger Soll
Coordinating Editor, Cochrane Neonatal Review Group
Division of Neonatal-Perinatal Medicine
University of Vermont
Fletcher Allen Health Care, Smith 581
111 Colchester Avenue
Burlington
Vermont USA
05401
Telephone 1: 802 847 2392
Facsimile: 802 847 5225
E-mail: Roger.Soll@vtmednet.org
| This review is published as a Cochrane review in The Cochrane Library,
Issue 3, 2007 (see http://www.thecochranelibrary.com for information).
Cochrane reviews are regularly updated as new evidence emerges and in response
to feedback. The Cochrane Library should be consulted for the most recent
version of the review. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}