Several factors increase the risk of serious infection in term newborn infants, for example, the presence in the birth canal of a bacterium that causes infection in the newborn (group B streptococcus), rupture of membranes more than a day before delivery, or high temperature in the mother during labour. Some paediatricians routinely prescribe an antibiotic for the newborn infant if any of these factors is present, even if the infant appears to be completely well. Others believe that it is safe and appropriate to observe these infants and only treat those who develop signs of illness, or have other evidence of infection during the first day after birth. We found two small trials that addressed this question. Neither provided enough evidence to guide practice. A further larger randomized trial is needed.
The two main sources of neonatal bacterial infection are the mother and the environment. Infections that appear in the first two days of life are usually the result of exposure to microorganisms of maternal origin (WHO 2002). Risk factors for perinatally acquired bacterial infection in the neonate include maternal fever during labour, preterm or prolonged rupture of membranes, preterm onset of labour, chorioamnionitis, maternal urinary tract infection, and maternal genital tract colonization with Group B streptococcus at 35-37 weeks of pregnancy (Schuchat 1994).
Babies born to mothers with such risk factors may be symptomatic at birth or, more commonly, show no signs of disease. Among the latter, there are some who will develop clinical changes that may suggest infection over the first hours or days of life. Those alterations include temperature instability, respiratory distress, vomiting, abdominal distension, poor feeding, lethargy or irritability, hypotension, tachycardia, pallor, petechiae, cyanosis and jaundice.
Laboratory evidence of neonatal bacterial infection is provided by a positive culture from blood or other normally sterile sites such as urine or cerebrospinal fluid. Although a positive blood culture constitutes the criterion for a diagnosis of sepsis, this test does not usually provide a rapid diagnosis, and it is not always available in some parts of the world. Ancillary evidence is provided by abnormalities in the white blood cell count and differential (e.g. low or high neutrophil count, left shift or elevated band/neutrophil ratio). Other laboratory tests of some diagnostic value include the platelet count and C-reactive protein. Apart from blood culture, the sensitivity, specificity and predictive values of laboratory tests for the diagnosis of neonatal infection are variable and often low (Anwer 2000).
The dilemma posed by the apparently asymptomatic newborn of a mother with risk factors for neonatal infection is that the signs of neonatal infection can be very subtle and difficult to differentiate from other conditions, especially during the early stages, and clinical deterioration can occur very rapidly. Delay in initiating antibiotic treatment when it is needed may significantly increase neonatal morbidity and mortality. On the other hand, prophylactic use of antibiotics in all asymptomatic newborn babies born to mothers with risk factors for infection will result in antibiotic treatment of many such infants who are not infected, and may lead to more frequent complications of antibiotic therapy. Among the latter are infections resistant to the antibiotics used, including non-bacterial infections, particularly fungal infections.
Guidelines for prevention of vertical transmission of group B streptococci, and thus the prevention of early-onset group B streptococcal infection in neonates, have been issued by the American Academy of Pediatrics (AAP 1997) and other bodies. These guidelines focus largely on the role of intrapartum antibiotic treatment of women colonized with group B streptococci. The AAP guideline recommends also that, because group B streptococcal infection can progress very rapidly, immediate antibiotic treatment of all at-risk newborn infants should be undertaken, and continued for at least 48-72 hours or until sepsis can be ruled out (AAP 1997). However, Lopez 2001 recommends no treatment for asymptomatic infants as long as close clinical surveillance is maintained.
There does not appear to be a generally accepted strategy for the use of antibiotics in asymptomatic neonates born to mothers with other risk factors for infection. The use of antibiotics in these circumstances is highly variable and often dependent on hospital preferences and personal experience. Thus, there is a need for a systematic review of randomized controlled trials of prophylactic versus selective use of antibiotics in asymptomatic newborns at risk for perinatally-acquired bacterial infection. We intended to restrict this review to trials carried out in term newborn infants because of important clinical differences in the preterm population. In order to take into account the important role of intrapartum use of maternal antibiotics in preventing vertical transmission of group B streptococcal and possibly other infections from mother to newborn, we planned subgroup analyses according to whether intrapartum antibiotics were or were not given to the mother.
Prophylactic use of antibiotics was considered to be the introduction of antibiotic use immediately after birth. Selective use of antibiotics was considered to be the introduction of antibiotic treatment after clinical or laboratory evidence suggesting neonatal infection. Clinical evidence suggesting infection was considered any of: respiratory signs (tachypnoea, apnea, irregular respirations, hypoxia); temperature instability (<36 degrees centigrade or >38 degrees centigrade); gastrointestinal signs (vomiting, diarrhea, abdominal distension, poor feeding, ileus); neurologic signs (lethargy, irritability, tremor or seizures, hypotonia or hyporeflexia, high-pitched cry, swelling of fontanel); cardiovascular signs (hypotension, tachycardia, metabolic acidosis); skin changes (pallor or skin mottling, petechiae or purpura, cold or clammy skin, cyanosis, jaundice). Laboratory evidence proving infection was considered to be positive blood culture, or positive culture of urine, cerebro-spinal fluid or other normally sterile site. Laboratory evidence suggesting infection was considered any of the following: abnormal white blood cell count (low or high), left shift, elevated band/neutrophil ratio; thrombocytopenia (< 100,000 per cubic mm); elevation of C-reactive protein.
MeSH terms used were:
"antibiotic", "antibiotic prophylaxis", "bacterial infections", "sepsis",
"streptococcus agalactiae", "infant, newborn", "infant mortality", "pregnancy",
"labor", "pregnancy, high-risk", "pregnancy outcome", "pregnancy complications,
infectious", "fever", "chorioamnionitis", "urinary tract infection", "fetal
membranes, premature rupture".
Non MeSH terms used were:
"neonatal infection", "neonatal sepsis", "antibiotic prophylaxis in the
neonate", "perinatal infection", "PROM", "prolonged rupture of membranes",
"maternal infection during labour", "maternal fever during labour", "maternal
colonization with Streptococcus B", "maternal colonization with Streptococcus
agalactiae", "urinary tract infection during labour" "amnionitis".
We did not apply a language restriction. We examined the reference lists
and "related articles" (in PubMed MEDLINE) in studies identified as potentially
relevant.
2. Three reviewers used the criteria and standard methods of the Cochrane Neonatal Review Group to assess the methodological quality of the included trials in terms of allocation concealment, blinding of parents or care takers and assessors to intervention, and completeness of assessment in all randomized individuals.
3. We used a data collection form to aid extraction of relevant information and data from each included study. Three reviewers extracted the data separately, compared these data and resolved differences by consensus.
4. We used the standard method of the Cochrane Neonatal Review Group to analyze and synthesize the data. We examined heterogeneity between trial results using the chi-squared test. We used the fixed effect model for meta-analysis. For categorical data, we expressed the treatment effects as relative risk with 95% confidence intervals and risk difference with 95% confidence intervals.
Two trials were considered to have fulfilled the inclusion criteria (Wolf 1976; Gerard 1979). Detailed information on these studies can be found in the "Characteristics of Included Studies" table.
Wolf 1976: The investigators conducted the trial in a hospital in Johannesburg, South Africa. The trial evaluated the effect of giving parenteral antibiotics immediately after birth to neonates born to mothers with rupture of membranes for more than 24 hours prior to birth. Forty nine infants were randomly assigned by card selection into a treatment (n = 24) and a non-treatment group (n = 25). Infants in the treatment group received penicillin G 50000 U/kg/day and kanamycin 10 mg/kg/day intramuscularly for seven days. Infants in the control group received no prophylactic antibiotics, but received selective antibiotics if there was clinical evidence of sepsis. The report provides data on clinical evidence of sepsis and neonatal mortality.
Wolf 1976 included both term and preterm
infants; 40 per cent of the infants were born before the completion of 37
weeks' gestation. The average gestational age was 37.4 weeks in the treatment
group and 37.7 weeks in the non-treatment group. Although these population
characteristics did not match our pre-specified criterion of only including
trials involving infants born at term, we (consensus of reviewers) decided
to include this trial since:
1. the majority (60%) of participating infants were born at term,
2. the vast majority (probably > 90%) of participating infants were born at "near-term", and
3. there are insufficient data in the published report to allow us to extract the data relating only to the term infants.
Gerard 1979: This was a quasi-random trial undertaken in a hospital in Charleroi, Belgium, to evaluate the effect of immediate post-natal treatment with parenteral penicillin of neonates with a maternal history of last trimester Group B streptococcus vaginal carriage. Women were screened for vaginal carriage of Group B streptococcus at between 32 and 34 weeks' gestation. There is no mention in the trial report that women who were found to carry Group B streptococcus received antepartum or intrapartum antibiotics. Sixty seven live born infants were included in this study. The gestational age of participating infants was reported inadequately. It appears, however, that both term and preterm infants were included. Nevertheless, the majority of infants, 56 of 67, are likely to have been term. For reasons similar to those discussed for Wolf 1976, we agreed unanimously to include this trial. We also decided to include this study even though the trial screened women for Group B streptococcal colonization at 32 to 34 week of gestation instead of 35 to 37 as pre-specified in the Cochrane protocol.
Infants born on an odd date (n = 29) received prophylactic penicillin 50000 to 100000 U/kg/day intramuscularly divided in two equal doses. Treatment continued until results of microbiological cultures of the external auditory canal, gastric aspirate, and fetal side of the placenta obtained at birth were known. Blood cultures were not obtained. Infants born on an even date (n = 38) were allocated to no prophylactic treatment. The indication for selective antibiotic administration in this trial was the growth of a pathogen from any of the sites from which microbiological cultures were obtained at birth (external auditory canal, gastric aspirate, and fetal side of the placenta). Antibiotic treatment was then prescribed for seven days. The report provides data on clinical evidence of sepsis and neonatal mortality.
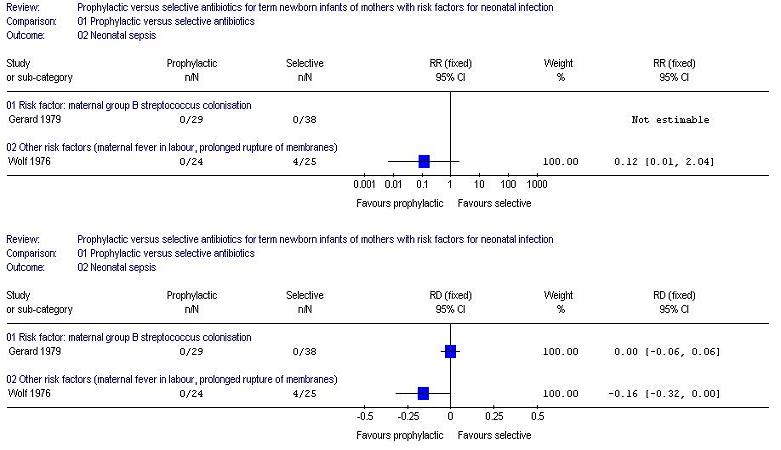
2) Neonatal sepsis:
(i) Studies enrolling babies born to mothers with group B streptococcal colonization during pregnancy: Gerard 1979
reported that none of the participating infants had evidence of neonatal
sepsis. Relative risk not estimable, risk difference 0.00 (95% confidence
interval -0.06, 0.06).
(ii) Studies enrolling babies born to mothers with other risk factors for neonatal infection: Wolf 1976 reported that four infants in the selective treatment group compared to none in the prophylactic treatment group developed signs consistent with neonatal sepsis (all four had positive cultures of placental blood obtained immediately after birth). Relative risk 0.12 (95% confidence interval 0.01, 2.04), risk difference -0.16 (95% confidence interval -0.32, 0.00).
3) Any systemic infection (sepsis, pneumonia, meningitis, other deep infection such as osteomyelitis): No further episodes of systemic infection in addition to the episodes of neonatal sepsis (described above) were reported in either trial.
4) Admission to neonatal intensive care unit with signs of infection: Not reported in either study.
Secondary outcomes:
1) Neonatal mortality due to infection: None of the infants who participated in either trial died in the neonatal period.
2) Use of antibiotics (proportion receiving any antibiotics):
(i) Studies enrolling babies born to mothers with group B streptococcal colonization during pregnancy: Gerard 1979.
All of the infants who were randomly allocated to the prophylactic group
received antibiotics. 16 (of 38) infants in the selective group received
antibiotics: Relative risk: 2.38 (95% confidence interval 1.64, 3.45), risk
difference: 0.58 (95% confidence interval -0.42, 0.74).
(ii) Studies enrolling babies born to mothers with other risk factors for neonatal infection: Wolf 1976. All of the infants who were randomly allocated to the prophylactic group received antibiotics. Four (of 25) infants in the selective group received antibiotics because of clinical evidence of sepsis: Relative risk: 6.25 (95% confidence interval 2.55, 15.34), risk difference: 0.84 (95% confidence interval 0.68, 1.00).
3) Unsatisfactory clinical or bacteriologic response after 48-72 hours of treatment, necessitating change in antibiotic regimen: Not reported in either study.
4) Total days of antibiotics: Seven days in Wolf 1976. In Gerard 1979, antibiotics were given in the treatment group until results of cultures were obtained, usually around 48 hours. If a positive culture was observed, antibiotics were given for seven days, independent of group allocation.
5) Side effects of antibiotics (fungal infection, diarrhea, other): Not reported in either study.
6) Readmission to hospital with signs of infection: Not reported in either study.
7) Length of hospital stay: Not reported in either study.
For all of the above outcomes, the available data did not permit any subgroup analysis of studies in which mothers did, or did not routinely receive intrapartum antibiotic treatment.
The included trials did not provide evidence that prophylactic versus selective antibiotic use affects neonatal mortality or the incidence of neonatal sepsis. However, because the trials were small, recruiting in total only 116 infants, these findings should be interpreted with caution. None of the infants who participated in either study died, and only four infants (all in one trial) developed clinical evidence of sepsis. The trials were therefore under-powered to detect an important effect of the intervention on these uncommon outcomes. We did not undertake any meta-analyses of the outcome data as we had specified at protocol stage that we would assess the evidence of effect in separate comparisons of 1) studies enrolling babies born to mothers with group B streptococcal colonization during pregnancy, and 2) studies enrolling babies born to mothers with other risk factors for neonatal infection. The risk of neonatal sepsis, the causal pathogens, and possibly the outcomes differ between these two populations. Therefore, as the potential impact of intervention might also be expected to differ, it was considered reasonable not to undertake meta-analyses.
In the absence of strong evidence from randomized controlled trials, the decision whether to administer antibiotics prophylactically or selectively (because of laboratory or clinical evidence of sepsis) to term infants of mothers with risk factors for sepsis will continue to be based upon data from observational studies that have estimated the increase in incidence of early onset systemic infection associated with various individual sepsis risk factors (intrapartum fever, prolonged rupture of the membranes, or maternal carriage of Group B streptococcus), or combinations of these risk factors. Policy will be influenced by the prevailing practice regarding antepartum screening for Group B streptococcus and the intrapartum use of antibiotics for women who are found to carry Group B streptococcus. Intrapartum antibiotic treatment of women colonized with group B streptococcus appears to reduce neonatal infection (Smaill 2004). It such circumstances, that is when infants have received appropriate intrapartum prophylaxis, clinicians and policy-makers have felt that additional postpartum antibiotic prophylaxis is unwarranted (AAP 1997).
Group B streptococcal infection is the commonest, but not the only, cause of severe neonatal sepsis. There is some concern that targeted screening and treatment for Group B streptococcal infection may result in a change in the epidemiology of neonatal infection and an increase in the incidence of early onset sepsis caused by other pathogens such as Gram-negative bacilli. There is evidence that this has occurred in the very low birth weight population in North America since the introduction of intrapartum antibiotic prophylaxis (Stoll 2002). There is also concern that the widespread use of intrapartum ampicillin has resulted in the emergence of ampicillin-resistant E. coli neonatal infection (Joseph 1998). There is a continued need for microbiological surveillance to identify changes in the epidemiology of early-onset infection, particularly the emergence of antibiotic resistance, in newborn infants. There is also a need to determine if the overall burden of mortality and morbidity associated with neonatal sepsis can be reduced by targeted intervention in the presence of sepsis risk factors such as maternal fever or prolonged rupture of the amniotic membranes. At present, there is not sufficient evidence that intrapartum antibiotic prophylaxis in women with prolonged rupture of the membranes at term improves neonatal outcomes (Flenady 2004). It is therefore important to continue to attempt to determine whether postpartum antibiotic prophylaxis can improve important outcomes for these neonates and their families.
Specifically with regard to the prevention of Group B streptococcal sepsis, the priority given to undertaking a randomized controlled trial of prophylactic versus selective antibiotics may be affected by the established approach to antepartum Group B streptococcus screening and intrapartum antibiotic prophylaxis. Such trials might be considered to be more of a priority in countries where a universal antepartum screening and intrapartum treatment policy has not been introduced.
Future trials should ideally aim to determine clinically important outcomes such as mortality and longer term neurodevelopment, rather than just incidence of microbiologically-confirmed early onset neonatal sepsis. This is especially important in settings where intrapartum antibiotics are given to mothers with risk factors for sepsis as intrapartum antibiotics may reduce the sensitivity of neonatal blood culture without improving clinical outcomes. It is also important that future studies consider the impact of antibiotic prophylaxis on antibiotic sensitivity patterns of potential pathogens, particularly if broad-spectrum prophylactic antibiotics are used.
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Gerard 1979 | Blinding of randomisation: no (quasi-randomised) Blinding of intervention: can't tell Complete follow-up: yes Blinding of outcome measurement: can't tell | 67 liveborn infants born to mothers who were Group B streptococcus carriers. | Intramuscular penicillin G 50,000 to 100,000 U/kg/day divided into two equal doses (N=29). One dose given in the delivery room and the other given after culture samples were taken. Treatment continued until results of culture were available. If one site was positive for GBS, antibiotics were given for seven days. Control group had no prophylactic antibiotics (N= 38). | Mortality. Neonatal sepsis. | C | |
| Wolf 1976 | Blinding of randomisation: unclear Blinding of intervention: can't tell Complete follow-up: yes Blinding of outcome measurement: can't tell | 49 asymptomatic infants born to mothers with prolonged rupture of membranes for more than 24 hours. | Intramuscular penicillin 50,000 U/kg/day and kanamicin 10 mg/kg/day divided into two doses during a period of seven days (N=24) versus no prophylactic antibiotics (N=25). | Mortality. Neonatal sepsis. | B |
| Study | Reason for exclusion |
| Boyer 1986 | This trial evaluated the effect of intrapartum prophylaxis, that is ampicillin given to women with risk factors for Group B streptococcal disease during labour, and then to her newborn infant following birth. |
| Ghaey 1985 | This study evaluated the effect of administering prophylactic intra-muscular penicillin to all newborn infants, rather than just those with risk factors for infection. |
| Patel 1999 | This trial assessed the effect of administering prophylactic intramuscular penicillin to all newborn infants, rather than just those with risk factors for infection. |
| Siegel 1980 | This trial assessed the effect of administering prophylactic penicillin to all newborn infants, rather than just those with risk factors for infection. |
Gerard P, Verghote-D'Hulst, Bachy A, Duhaut G. Group B Streptococcal colonization of pregnant women and their neonates. Acta Paediatrica Scandinavica 1979;68:819-23.
Wolf 1976 {published data only}
Wolf RL, Olinsky A. Prolonged rupture of fetal membranes and neonatal infections. South African Medical Journal 1976;50:574-6.
Boyer K, Gotoff S. Prevention of early-onset neonatal group B streptococcal disease with selective intrapartum chemoprophylaxis. New England Journal of Medicine 1986;314:1665-9.
Ghaey 1985 {published data only}
Ghaey K, Tolpin M, Schauf V, Chakinis C, Pyati S, Nelson K, Pildes R, Riff L. Penicillin prophylaxis and the neonatal microbial flora. The Journal of Infectious Diseases 1985;152:1070-3.
Patel 1999 {published data only}
Patel DM, Rhodes PG, LeBlanc MH, Graves GR, Glick C, Morrison J. Role of postnatal penicillin prophylaxis in prevention of neonatal group B streptococcus infection. Acta Paediatrica 1999;88:874-9.
Siegel 1980 {published data only}
* Siegel J, McCracken Jr. GH, Threlkeld N, Milvenan B, Rosenfeld CR. Single-dose penicillin prophylaxis against neonatal group B streptococcal infections. A controlled trial in 18738 newborn infants. New England Journal of Medicine 1980;303:769-75.
Siegel J, McCracken Jr. GH, Threlkeld N, Milvenan B, Rosenfeld CR. Single-dose penicillin prophylaxis against neonatal group B streptococcal infections. Conclusion of a 41 month controlled trial. Lancet 1982;1:1426-30.
* indicates the primary reference for the study
American Academy of Pediatrics. Revised guidelines for prevention of early-onset group B streptococcal (GBS) infection. Pediatrics 1997;99:489-496.
Anwer SK, Mustafa S. Rapid identification of neonatal sepsis. Journal of the Pakistan Medical Association 2000;50:94-100.
Bellig LL. Neonatal sepsis. eMedicine Journal 2002;3(7).
Centers for Disease Control and Prevention. Prevention of Perinatal Group B Streptococcal Disease Revised Guidelines. 2002.
Flenady V, King J. Antibiotics for prelabour rupture of membranes at or near term (Cochrane Review). In: The Cochrane Library, Issue 2, 2004. Chichester, UK: John Wiley & Sons, Ltd.
Garcia-Prats JA, Cooper TR, Schneider VF, Stager CE, Hansen TN. Rapid detection of microorganisms in blood cultures of newborn infants utilizing an automated blood culture system. Pediatrics 2000;105:523-7.
Gerdes JS, Polin R. Early diagnosis and treatment of neonatal sepsis. Indian Journal of Pediatrics 1998;65:63-78.
Joseph TA, Pyati SP, Jacobs N. Neonatal early-onset Escherichia coli disease. The effect of intrapartum ampicillin. Archives of Pediatrics and Adolescent Medicine 1998;152:35-40.
Lopez AR, Hernandez GM, Domenech ME. Vertically transmited bacteremias: to treat or not to treat? Anales Espanoles de Pediatria 2001;54:160-4.
Schrag SJ, Zell ER, Stat M, Lynfield R, Roome A, Arnold KE, Craig AS, Harrison LH, Reingold A, Stefonek K, Smith G, Gamble M, Schuchat A. A population-based comparison of strategies to prevent early-onset group B streptococcal disease in neonates. New England Journal of Medicine 2002;347:233-9.
Schuchat A, Wenger JD. Epidemiology of group B streptococcal disease. Risk factors, prevention strategies, and vaccine development. Epidemiologic Reviews 1994;16:374-402.
Smaill F. Intrapartum antibiotics for Group B streptococcal colonisation (Cochrane Review). In: The Cochrane Library, Issue 2, 2004. Chichester, UK: John Wiley & Sons, Ltd.
Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, Lemons JA, Donovan EF, Stark AR, Tyson JE, Oh W, Bauer CR, Korones SB, Shankaran S, Laptook AR, Stevenson DK, Papile LA, Poole WK. Changes in pathogens causing early-onset sepsis in very-low-birth-weight infants. New England Journal of Medicine 2002;347:240-7.
World Health Organization. Perinatal Mortality: A listing of available information. WHO Report Geneva Switzerland 2002.
01.01 Neonatal mortality
01.02 Neonatal sepsis
01.03 Use of antibiotics (proportion receiving any antibiotics)
| Comparison or outcome | Studies | Participants | Statistical method | Effect size |
|---|---|---|---|---|
| 01 Prophylactic versus selective antibiotics | ||||
| 01 Neonatal mortality | RR (fixed), 95% CI | No numeric data | ||
| 02 Neonatal sepsis | RR (fixed), 95% CI | No total | ||
| 03 Use of antibiotics (proportion receiving any antibiotics) | RR (fixed), 95% CI | No total | ||
Dr Ornella Lincetto
Medical Officer
Reproductive Health and Research
World Health Organization
Geneva SWITZERLAND
E-mail: lincettoo@who.int
Dr William McGuire
Senior Lecturer in Neonatal Medicine
Tayside Institute of Child Health
Ninewells Hospital and Medical School
Dundee
UK
DD1 9SY
Telephone 1: +44 1382 632179
Facsimile: +44 1382 632597
E-mail: w.mcguire@dundee.ac.uk
Dr Haroon Saloojee
Division of Community Paediatrics
Department of Paediatrics and Child Health
University of the Witwatersrand
Witwatersrand SOUTH AFRICA
E-mail: saloojeeh@medicine.wits.ac.za
| This review is published as a Cochrane review in The
Cochrane Library, Issue 4, 2004 (see http://www.thecochranelibrary.com/ for information.)
Cochrane reviews are regularly updated as new evidence emerges and in response
to comments and criticisms, and The Cochrane Library should be consulted
for the most recent version of the Review. |
{kind=link}
{kind=link}
{kind=link}