

Background - Methods - Results- Characteristics of Included Studies - References - Data Tables & Graphs
Additional long-term neurodevelopmental follow-up data have been included in this update from 7 trials; data for Baden 1972 and Romagnoli 1999 were published in full reports, data for Subhedar 1997 were published as a letter to the editor, data for Stark 2001 were obtained from a presented and published abstract, and data for Sanders 1994, Sinkin 2000 and Watterberg 1999 were provided by the investigators. Two trials reporting short-term outcome data are also newly included; Halac 1990 and Biswas 2002.
Although early steroid treatment facilitates extubation and reduces the risk of chronic lung disease, long-term follow-up studies indicate a possible increased risk of adverse neurosensory outcome. Furthermore, short-term complications such as gastrointestinal bleeding, intestinal perforation, hyperglycaemia, hypertension, hypertrophic cardiomyopathy and growth failure are increased by early steroid treatment.
Chronic lung disease (CLD) is a major problem for newborn babies in neonatal intensive care units. Persistent inflammation of the lungs is the most likely cause. Corticosteroid drugs have been used to either prevent or treat CLD because of their strong anti-inflammatory effects. The review of trials found that the benefits of giving corticosteroids to infants less than 96 hours old may not outweigh the known adverse effects. The beneficial effects were shorter time on the ventilator and less CLD but the adverse effects included high blood pressure, gastrointestinal bleeding and perforation, an excess of glucose in the bloodstream and an increased risk of cerebral palsy at follow-up. Use of early steroids should be curtailed until more research has been performed.
Even more recently corticosteroids have been used to try to prevent CLD by treating at risk preterm babies within the first four days of life. It is not clear if early use of steroids provides long-term benefits. Nor is it clear that adverse neurological outcomes found in animal studies do not apply to the immature human newborn infant.
In total, more than 37 randomised trials of postnatal steroids have been conducted in babies at risk of, or having CLD (see previous reviews by Halliday 1997; Halliday 1999; Halliday 1999a; Arias-Camison 1999; Bhuta 1998; Doyle 2000b and Tarnow-Mordi 1999). There are three existing Cochrane reviews, which review separately the trials in which postnatal steroids were started within 96 hours of birth, 7-14 days after birth, or predominantly after three weeks. This review examines the outcome of trials where preterm infants have been treated with corticosteroids within 96 hours of birth. It is an update of a previous Cochrane review (Halliday 2000) and it includes long-term outcome data from 7 additional trials.
The corticosteroid administered was usually dexamethasone and the commonest treatment regimen was 0.50 mg/kg/day for 3 days followed by 0.25 mg/kg/day for 3 days, 0.12 mg/kg/day for 3 days and 0.05 mg/kg/day for 3 days. There was, however, considerable variation. Three studies used hydrocortisone (Baden 1972, Watterberg 1999, and Biswas 2002) and the treatment regimens for dexamethasone included short courses of 1-2 days and longer courses of up to 4 weeks (see under Description of Studies).
Baden 1972 included 44 infants with respiratory distress syndrome, mild hypoxia and hypercapnia and a chest radiograph compatible with RDS. They were randomised to receive either hydrocortisone 15 mg/kg on admission and 12 hours later intravenously, or a placebo. Their birth weights ranged from 800 to 2805 g and gestational ages from 26 to 36 weeks.
Biswas 2002 was a multicentre randomised trial of 253 infants <30 weeks' gestational age. The infants were mechanically ventilated and were entered within 9 hours of birth. All were give surfactant in the first 24 hours of life. Those in the treatment group (n=125) were randomised to receive an infusion of hydrocortisone 1 mg/kg/day and tri-iodothyronine (T3) 6 microgram/kg/day for 5 days, then hydrocortisone 0.5 mg/kg/day and T3 3 microgram/kg/day for 2 days. The placebo group (n=128) received an equal volume of 5% dextrose.
Garland 1999 was a prospective multicentre randomised trial comparing a 3 day course of dexamethasone therapy beginning at 24-48 hours of life with placebo. 241 preterm infants (dexamethasone n = 118, placebo n = 123) who weighed between 500 g and 1500 g, had received surfactant therapy and were at significant risk for CLD or death using a predictive model at 24 hours were enrolled. Dexamethasone was given in a 3 day tapering course at 12 hour intervals. The first 2 doses were 0.4 mg/kg, the 3rd and 4th doses were 0.2 mg/kg and the 5th and 6th doses were 0.1 mg/kg and 0.05 mg/kg respectively. A similar volume of normal saline was given to placebo treated infants at similar time intervals.
Halac 1990 was a randomised trial to determine if prenatal corticosteroid therapy would reduce the incidence of NEC. Women were randomised to prenatal betamethasone or placebo when they were admitted in preterm labor and expected to deliver within 24 hours. Infants of mothers who had received placebo were then randomised to postnatal dexamethasone or placebo; only the infants randomised to postnatal therapy are included in this review. Study infants were <1501 g birth weight or <34 weeks' gestation and had evidence of "birth asphyxia" (1 minute Apgar score <5, prolonged resuscitation and metabolic acidosis [HC03 <15 mmol/L within 1 hour of birth]). Treatment was assigned by a table of random numbers. The treatment group (n=130) received 2 mg/kg/day of dexamethasone phosphate intravenously for 7 days; the control group (n=118) received an equal volume of 10% dextrose. The major endpoint of the study was NEC.
Kopelman 1999 was a prospective blinded randomised controlled trial of 70 babies of less than 28 weeks gestation who required mechanical ventilation. 37 infants received dexamethasone 0.20 mg/kg at delivery and 33 babies received a placebo of an equal volume of saline.
Lin 1999 - a randomised trial with a sequential design involving infants of 500-1999 g. Infants were stratified by birth weight into 3 groups: 500-999 g, 1000-1500 g and 1501- 1999 g. Within each group equal numbers of dexamethasone-treated or control cards were placed in envelopes for random selection of the first infant of each pair. The next infant of the appropriate birth weight stratum was enrolled for the match. A pharmacist opened the envelope and the dexamethasone or saline placebo was administered blind. Entry criteria were: severe radiographic RDS, need for assisted ventilation within 6 h of birth, and given 1 dose of surfactant. Treated infants were given dexamethasone, starting within 12 h of birth, at 0.25 mg/kg/dose 12 hourly for 7 d, 0.12 mg/kg/dose 12 hourly for 7 d, 0.05 mg/kg/dose 12 hourly for 7 d and 0.02 mg/kg/dose 12 hourly for 7 d giving a total of 4 weeks treatment. Results are presented for 20 treated and 20 control infants.
Mukhopadhyay 1998 - a randomised trial with untreated controls. Method of randomisation was not described. Treated infants received dexamethasone 0.5 mg/kg/dose 12 hourly for 3 days beginning within 6 hours of birth. 19 infants of < 34 wk and < 2000 g who could be provided with mechanical ventilation were included in the study. They had severe RDS but were not given surfactant.
Rastogi 1996 recruited 70 infants with birth weights 700 to 1500 g who had severe RDS (assisted ventilation with 40% or more oxygen and/or 7 cm H2O mean airway pressure, a/A PO2 ratio of 0.24 or less) and had been treated with surfactant before entry. The infants were < 12 hours old. Infants were excluded if they had major malformations, chromosome abnormalities, 5 minute Apgar scores of < 3 or the presence of severe infection. The intervention group had dexamethasone intravenously every 12 hours according to the following schedule: 0.50 mg/kg/d on days 1-3, 0.30 mg/kg/d on days 4-6, 0.20 mg/kg/d on days 7-9 and finally 0.10 mg/kg/d on days 10-12. A saline placebo was given intravenously to the control group.
Romagnoli 1999 - a randomised trial using numbered sealed envelopes involving 25 dexamethasone treated infants and 25 untreated controls. Entry criteria were: birth weight <1251 g, gestational age < 33 wk, ventilator and oxygen dependent at 72 h and at high risk of CLD using a local scoring system that predicted a 90% risk. Treated infants were given dexamethasone beginning on the 4th day at a dose of 0.5 mg/kg/d for 3 d, 0.25 mg/kg/d for 3 d and 0.125 mg/kg/d for 1 d.
Sanders 1994 enrolled 40 babies < 30 weeks' gestation who had RDS diagnosed by clinical and radiographic signs, required mechanical ventilation at 12-18 hours of age, and had received at least one dose of exogenous surfactant. Exclusion criteria at entry included a strong suspicion of sepsis or pneumonia, congenital heart disease, chromosome abnormalities and those infants who received an exchange transfusion. The babies were randomised to receive either dexamethasone 0.50 mg/kg between 12 and 18 hours of age and a second dose 12 hours later, or a saline placebo. Both treatments were given intravenously.
Shinwell 1996 was a multicentre trial which randomised 248 infants of birth weight 500 to 2000 g if they had clinical and radiographic evidence of RDS, required mechanical ventilation in more than 40% oxygen, were less than 12 hours old and had no contraindications to steroid treatment, such as a bleeding tendency, hypertension, hyperglycaemia or active infection. Babies with lethal congenital malformations were also excluded. The intervention group received dexamethasone 0.25 mg/kg intravenously every 12 hours for a total of six doses. The control group received intravenous saline.
Sinkin 2000 was a multicentre randomised double-blind trial of 384 babies of less than 30 weeks' gestation with RDS. 189 babies received dexamethasone 0.50 mg/kg at 12 - 18 hours of age and with a second dose 12 hours later, and 195 babies had an equal volume of saline placebo.
Soll 1999 was a multicentre randomised double-blinded controlled trial comparing dexamethasone given at 12 hours of age with selective late dexamethasone therapy in premature infants weighing 501-1000 g (early dexamethasone n = 272, late selective therapy n = 270). The babies required assisted ventilation, had received surfactant therapy, were physiologically stable, had no obvious life threatening congenital anomaly, had blood cultures obtained and antibiotic therapy started. Infants were randomly assigned to early dexamethasone therapy or saline placebo. Intravenous dexamethasone was administered for 12 days according to the following schedule: 0.5 mg/kg/day for 3 days, 0.25 mg/kg/day for 3 days, 0.1 mg/kg/day for 3 days and 0.05 mg/kg/day for 3 days. Infants in either group could receive late postnatal steroids beginning on day 14 if they needed assisted ventilation with supplemental oxygen > 30%.
Stark 2001 was a randomised multicentre controlled trial to compare a tapering course of stress dose corticosteroid started on the first day with placebo. Infants with birth weight 501 - 1000 g needing mechanical ventilation before 12 hours of age were eligible for the study. Infants with birth weight > 750 g also needed to have received surfactant and required an oxygen concentration of 30% or greater. The initial dose of dexamethasone was 0.15 mg/kg/day for 3 days, then tapered over 7 days. After enrolling 220 infants (sample size was 1200), the trial was halted for unanticipated adverse events. 111 infants had been randomised to receive dexamethasone and 109 placebo.
Subhedar 1997 was a randomised trial which enrolled infants into one of four treatment groups using a factorial design. Both inhaled nitric oxide and early dexamethasone were compared separately with controls. 42 infants were randomised: 10 receiving inhaled NO alone; 11 dexamethasone alone; 10 both treatments; and 11 neither treatment. The 21 infants receiving dexamethasone were compared with 21 controls. Infants were eligible for entry into the trial at 96 hours of age if they met the following criteria: gestational age < 32 weeks, mechanical ventilation from birth, had received surfactant therapy and were thought to be at high risk of developing CLD using a scoring system (Ryan et al 1996). Exclusion criteria included major congenital anomaly, structural cardiac defect, significant ductus shunting, culture positive sepsis, IVH with parenchymal involvement, pulmonary or gastrointestinal haemorrhage, disordered coagulation or platelet count < 50,000. Dexamethasone was given intravenously at 12 hourly intervals for six days: 0.50 mg/kg/dose for six doses, and 0.25 mg/kg/dose for a further six doses. Control infants were not given a placebo.
Suske 1996 randomised 26 infants with gestational ages 24 to 34 weeks who had RDS that had been treated with surfactant. Infants with known septicaemia during the first week of life, haemodynamically relevant cardiac anomalies except for PDA, or malformations of the lung or CNS were excluded. Randomisation was by drawing lots prior to the age of two hours. The intervention group received dexamethasone 0.50 mg/kg intravenously in two divided doses for five days and the controls received no placebo.
Tapia 1998 was a multicentre double-blind placebo controlled trial of 109 preterm infants with RDS and birth weights between 700 and 1600 g who were treated with mechanical ventilation and surfactant. 55 babies were randomised to receive dexamethasone 0.50 mg/kg/day for 3 days, followed by 0.25 mg/kg/day for 3 days, followed by 0.12 mg/kg/day for 3 days and then 0.06 mg/kg/day for 3 days. 54 control infants received an equal volume of saline.
Wang 1996 - a randomised trial of a 21 day course of either dexamethasone or saline placebo given in a double-blind fashion. Method of randomisation not stated. Entry criteria: birth weight 1000 - 1999 g, AGA, clinical and radiological severe RDS, mechanical ventilation and age < 12 h. Surfactant was not given as it was not commercially available in Taiwan at the time of the study. Treated infants were given dexamethasone 0.25 mg/kg/dose 12 hourly for 7 d, 0.125 mg/kg/dose 12 hourly for 7 d, 0.05 mg/kg/dose 12 hourly for 7 d making a total course of 21 days. The first dose of dexamethasone was given during the first 12 h of life. There were 34 infants in the dexamethasone group and 29 in the placebo control group.
Watterberg 1999 was a randomised double-masked placebo controlled pilot study to compare early treatment with low dose hydrocortisone (1.0 mg/kg/day for 9 days, then 0.5 mg/kg/day for 3 days) begun before 48 hours of age with placebo. 40 infants weighing between 500-999 g and who were mechanically ventilated were enrolled at 2 centres, 20 hydrocortisone treated and 20 placebo controls.
Yeh 1990 enrolled 57 infants whose birth weights were < 2000 g and who had severe RDS based upon the appearances on a chest radiograph and the need for mechanical ventilation within four hours after birth. The absence of infection was also required for inclusion. The babies were randomly assigned to receive dexamethasone 0.50 mg/kg per dose every 12 hours from days 1-3, then 0.25 mg/kg per dose 12 hourly from days 4-6, then 0.12 mg/kg per dose 12 hourly from days 7 to 9 and finally 0.05 mg/kg per dose 12 hourly from days 10-12. All doses were given intravenously. A saline solution was used in the placebo group.
Yeh 1997 was a multicentre randomised double-blind clinical trial of 262 preterm infants (< 2000 g) who had RDS and required mechanical ventilation from shortly after birth. The treated group had dexamethasone 0.25 mg/kg/dose every 12 hours i.v. from day 1 to 7; 0.12 mg/kg/dose every 12 hours i.v. from day 8 - 14; 0.05 mg/kg/dose every 12 hours i.v. from days 15 - 21; and 0.02 mg/kg/dose every 12 hours i.v. from day 22 to 28. Control infants had a saline placebo.
Biswas 2002 - Randomisation was conducted by the Perinatal Trials Unit in Oxford, with stratification for centre and gender, and the code held by the study pharmacist. Controls received an equal infusion rate of 5% dextrose. Syringes were made in one pharmacy and transported to individual study centres. Short-term outcomes were reported for all infants enrolled. There was no follow-up component.
Garland 1999 - A multicentre randomised controlled trial with infants randomised at each centre within each of 4 strata based on birth weight (< 1001 g, > 1000 g) and arterial/Alveolar (a/A) ratio before surfactant ( < 0.16, > 0.15). Randomisation codes were maintained by the study pharmacists at each centre. Investigators, caregivers and parents were blinded to treatment allocation. At the first interim analysis (n=75), an increased risk of gastrointestinal perforation was noted in the dexamethasone group. After adjusting for severity of illness the difference was not of statistical significance to stop enrolment. However, to ensure patient safety the data monitoring committee recommended reducing the dexamethasone dose. The dosing schedule was changed to 4 doses of 0.25 mg/kg/dose every 12 hours begun at 24 to 48 hours, followed by doses of 0.125 mg/kg and 0.05 mg/kg at the next two 12 hour periods respectively. After the first interim analysis all enrolled infants received ranitidine therapy during the first 3 days of the study. Outcome measures appear to have been reported for all 241 infants enrolled in the study. There was no follow-up component.
Halac 1990 - Randomisation was by means of a table of random numbers, with placebo blinding. It was stated that deaths before 10 days of age were excluded from the study; there were a total of 5 early deaths from sepsis, but it was not clear how often this occurred in each group. Apart from these infants, outcome data were provided for all remaining infants enrolled. There was limited follow-up to 6 months of age, but no results were given, apart from a statement that "growth and development were not hampered in any of these patients".
Kopelman 1999 - This was a prospective blinded randomised controlled trial with randomisation performed in the pharmacy after stratification for treatment with antenatal steroids. The blinded clinical team provided care. Outcome data were provided for all infants enrolled. There was no follow-up component.
Lin 1999 - Randomisation was by opening sealed envelopes in the pharmacy. The study had a sequential analysis design with 12 infants being paired successfully. Outcome measures were given for all 40 infants enrolled including those who remained unpaired. There was no follow-up component.
Mukhopadhyay 1998 - Method of randomisation not stated. Only 28 of 43 eligible babies could be provided with ventilation. Eight babies were subsequently excluded due to non-availability of blood gases due to a technical fault and 1 baby was excluded because of congenital heart block. This left 19 babies for study; 10 received intravenous dexamethasone and 9 were not treated with any drug. There is no mention of placebo. Outcome measures were reported for these 19 infants. There was no follow-up component.
Rastogi 1996 - Randomisation occurred in the pharmacy using a random number list after stratifying for birth weight into three groups: 700-999 g, 1000 to 1249 g and 1250 g to 1500 g. The clinical team and other study personnel were blinded to the assignments until the study was completed and all outcome variables were recorded for all infants. There was no follow-up component.
Romagnoli 1999 - Randomisation, obtained
by random number allocation, was achieved by opening numbered sealed envelopes.
Infants with prenatal infections, congenital malformations and evidence
of sepsis at randomisation were excluded. There is no mention of placebo.
Outcome measures were reported for all 50 infants enrolled.
Follow-up component: Survivors were seen at 34-42 months of age, corrected
for prematurity, by one pediatrician and one neurologist, with observers
blinded to treatment group allocation. The follow-up rate of survivors
was 100% (45/45). Cerebral palsy was diagnosed by the neurologist, but
the criteria were not specified, neither were there specific criteria for
blindness or deafness. Psychological assessment included the Stanford-Binet
- 3rd Revision; intellectual impairment comprised an IQ <70. "Major
neurosensory impairment" comprised either blindness or deafness.
Sanders 1994 - Randomisation occurred in
the pharmacy after opening a sealed envelopes. Dexamethasone or placebo
were dispensed in labelled syringes. Clinical personnel were not aware
of the assignment of the intervention. Outcomes are given for all 40 babies
enrolled.
Follow-up component: Survivors were seen at mean ages of 64 (SD 8)
months (DEX) and 61 (SD 4) months (controls), not corrected for prematurity,
by a paediatrician, a neurologist, and a psychologist, with observers blinded
to treatment group allocation. Additional data was sought from parents
and teachers. The follow-up rate of survivors was 100% (31/31). Criterion
for the diagnosis of cerebral palsy was a fixed motor deficit diagnosed
by the neurologist. Blindness comprised visual acuity < 6/60 in the
better eye. Deafness comprised the need for a hearing aid. Psychological
assessment included the Wechsler Scales (WISC and WPPSI) - intellectual
impairment comprised a Full Scale IQ <70. Major neurosensory disability
was not specified. Further follow-up at 15 years of age is planned.
Shinwell 1996 - Each participating unit
was supplied with numbered sets of syringes containing either dexamethasone
or physiological saline. Syringes containing dexamethasone were not distinguishable
from those containing saline. Syringe sets were numbered according to a
random number list and randomisation was stratified by centre and by two
birth weight groups: 500 - 1000 g and 1001 - 2000 g. The drug assignment
was not known to any of the investigators until after the three month observation
period of the last enrolled infant. Outcomes are reported for 248 of the
255 infants who were enrolled. The seven infants subsequently excluded
from analysis included three with major congenital abnormalities (two with
myotonic dystrophy and one with cyanotic congenital heart disease), three
with errors in drug administration and one randomised after the age of
12 hours.
Follow-up component: Survivors were seen at a mean age of 53 (SD 18;
range 24-71) months, presumably not corrected for prematurity. Children
were seen in multiple follow-up clinics by multiple pediatricians, with
observers blinded to treatment group allocation. The follow-up rate of
survivors was 83% (159/190). Criteria for the diagnosis of cerebral palsy
were not specified, but the diagnosis was made by neurologists in all cases.
There were no specified criteria for blindness. Deafness comprised the
need for hearing aids. There were no formal psychological assessments;
developmental delay was assigned by judgement of the multiple assessors.
Major neurosensory disability comprised any of non-ambulant cerebral palsy,
global retardation (not specified), blindness or deafness. Further follow-up
is planned at school age.
Sinkin 2000 - A multicentre randomised double-blind
trial where randomisation with stratification by centre was performed using
a set of sealed envelopes in the pharmacy. Outcome data appear to have
been provided for all infants enrolled.
Follow-up component: Data were obtained from one of the 4 original
centres in the study, from follow-up clinic appointments, and from questionnaires
to parents and paediatricians. Survivors were seen at approximately 12
months of age, corrected for prematurity, by a paediatrician, a neurologist,
and a psychologist, with observers blinded to treatment group allocation.
The follow-up rate of survivors was 13% (41/311) of survivors at 36 weeks
postmenstrual age overall, but was confined to one of 4 individual study
centres, within which the follow-up rate was 100% (41/41). The criterion
for the diagnosis of cerebral palsy was a fixed motor deficit diagnosed
by the neurologist. Blindness comprised visual acuity < 6/60 in the
better eye. Deafness comprised the need for a hearing aid. Psychological
assessment included the Bayley Scales of Infant Development. Major neurosensory
disability was not specified.
Soll 1999 - A multicentre randomised double blinded controlled trial with randomisation in hospital pharmacies after opening opaque sealed envelopes supplied by the Vermont Oxford Neonatal Network. The study was stopped prior to completion of sample size goals due to concern regarding adverse effects in the early steroid therapy group. Outcome measures appear to have been reported for most of the 542 infants enrolled. There was no follow-up component.
Stark 2001 - A randomised multicentre controlled
trial with random allocation performed in hospital pharmacies using random
number scheme. The study had a factorial design so that infants were also
randomised to routine ventilator management or a strategy of minimal ventilator
support aimed at reducing mechanical lung injury. After enrolling 220 infants
from a sample size estimate of 1200 the trial was halted for unanticipated
adverse effects. Outcome measures seem to have been reported for all 220
patients enrolled in the trial.
Follow-up component: Survivors were seen at 18-22 months of age, corrected
for prematurity by trained developmental observers blinded to treatment
group allocation. The follow-up rate of survivors was 87.2% (143/164).
Criteria for the diagnosis of cerebral palsy were not specified, and rates
of blindness or deafness were not reported. Psychological assessment included
the MDI and the PDI of the Bayley Scales of Infant Development. Major neurosensory
disability comprised any of abnormal neurological exam, blindness, deafness,
or an MDI or PDI <-2 SD.
Subhedar 1997 - Randomised trial with factorial
design providing four groups. Block randomisation was performed using computer
generated random numbers and sealed envelopes. No placebo was used. There
was no evidence of blinding of clinicians. Outcome measures were reported
for all infants enrolled.
Follow-up component: Survivors were seen at 30 months of age, corrected
for prematurity, by one developmental pediatrician who was blinded to treatment
group allocation. The follow-up rate of survivors was 95% (21/22). Criteria
for the diagnosis of cerebral palsy were specified, but not specific criteria
for deafness; blindness was diagnosed by an ophthalmologist. Psychological
assessment included the MDI and the PDI of the Bayley Scales of Infant
Development. Major neurosensory disability comprised any of cerebral palsy,
an MDI or PDI <71, blindness or deafness.
Suske 1996 - Randomisation was by drawing lots; the lot numbers corresponded to numbers on non-transparent envelopes. The random lots and the envelopes were drawn by a neutral, uninvolved person. The trial was considered as a pilot study before starting a multicentre study and it was planned that the trial would be stopped if a statistically significant difference was found between the groups. The inclusion criteria were met by 41 infants. Due to lack of cooperation and coordination at the beginning of the study, nine infants were not randomised. Four infants were excluded after randomisation because of definite signs of septicaemia. Results are given for 26 of the 28 remaining infants. There was no follow-up component.
Tapia 1998 - A multicentre double-blind placebo controlled study with random assignment at each centre using ampoules of dexamethasone and saline prepared in the hospital pharmacy of one of the centres. Outcomes were reported for 109 of the 113 infants enrolled. Two babies from the dexamethasone group were excluded, 1 because of congenital cystic adenomatoid malformation and 1 because of early sepsis. Two patients from the placebo group were excluded, 1 because of early sepsis and the other was transferred to another hospital at 2 weeks of age and further data on outcome could not be obtained. There was no follow-up component.
Wang 1996 - Random allocation was said to have been double-blind but the exact method was not described. Outcome measures were reported for all 63 babies enrolled in the study. There was no follow-up component.
Watterberg 1999 - A randomised double-masked
placebo-controlled pilot study with infants randomised at each centre by
constant block design with 4 patients per block to minimise bias over time.
Separate randomisation tables were used for infants exposed to antenatal
steroids. The hydrocortisone doses and the placebo of normal saline were
prepared by the hospital pharmacies. Outcome measures were reported for
all of the 40 infants enrolled in the trial.
Follow-up component: Survivors were seen in regular follow-up clinic
for one of the two study sites at a mean age of 11 (SD 2) months, corrected
for prematurity, by a neonatologist and a physiotherapist, with observers
blinded to treatment group allocation. The follow-up rate of survivors
was 52.9% (18/34) for the study overall, but 85.7% (18/21) for the one
study centre with follow-up data. Criteria for the diagnosis of cerebral
palsy were specified and comprised abnormal tone and movement. Blindness
was diagnosed by an ophthalmologist, and deafness was screened for inn
early infancy and at follow-up. There was no formal psychological testing.
Major neurosensory disability was not defined.
Yeh 1990 - Randomisation was performed in the pharmacy using balanced blocks of 10. The vials were labelled in the pharmacy and the clinical staff were unaware of the assignment. Sixty infants were included in the study and three were subsequently withdrawn: one because of death from Haemophilus influenzae septicaemia six hours after enrolment, and two because of an error in the measurement of birth weight (581 and 2200 g). Outcomes for these three infants are not given. There was no follow-up component.
Yeh 1997 - The method of randomisation was by
an assignment list in the central pharmacy. The sample size was calculated
on the basis of an expected 50% reduction in the incidence of CLD with
early dexamethasone, allowing a 5% chance of a type I error and a 10% chance
of a type II error. Outcome data are presented for all 262 infants enrolled.
The study is described as double-blind.
Follow-up component: Survivors were seen at a mean age of 25 months,
corrected for prematurity, by one neurologist and one psychologist, with
observers blinded to treatment group allocation. The follow-up rate of
survivors was 81.1% (133/164). Criteria for the diagnosis of cerebral palsy,
blindness or deafness were not specified. Psychological assessment included
the MDI and the PDI of the Bayley Scales of Infant Development. Major neurosensory
disability comprised severe motor dysfunction (child non-ambulant), or
an MDI or PDI <-2 SD.
Biswas 2002 - There were no significant effects of the infusion of hydrocortisone and T3 on the primary endpoint of death or failure to extubate by 7 days, or death or oxygen dependency at 14 days. PDA was significantly reduced in the treatment group (41/125 vs 60/128; relative risk 0.70, 95% CI 0.51, 0.96), but there were no other significant differences in secondary outcomes.
Garland 1999 - Early dexamethasone treated infants were more likely to survive without CLD (83/118 vs 71/123; P = 0.03) than placebo treated controls. There were also less likely to develop CLD if they survived to 28 days (16/99 vs 27/98; P = 0.042). Mortality rates were not significantly different. Subsequent dexamethasone therapy was used less often in the early dexamethasone treated infants who survived (68/99 vs 81/98; P = 0.01). Intestinal perforation was more common, but not significantly so, in the dexamethasone treated infants (12/118 vs 7/122; P = 0.20); during the first week of life the difference was significant (9/118 vs 1/122; P = 0.009). Babies in the dexamethasone group also spent less time in oxygen (median days 43 vs 50; P = 0.04). Any grade of IVH (36% vs 52%; P = 0.02) and PDA ligation (14% vs 28%; P = 0.01) were also less common in the dexamethasone group. Hypertension and insulin therapy were needed more often in the dexamethasone treated infants (P = 0.007).
Halac 1990 - There were no substantial or statistically significant effects of dexamethasone on neonatal mortality, mortality to hospital discharge, NEC, sepsis, PDA or severe IVH.
Kopelman 1999 - IMV rate and ventilation index improved more rapidly in the dexamethasone treated group. Mean blood pressure was higher after the first day in the dexamethasone group. Dexamethasone treated infants has fewer PDAs (13/37 vs 19/33; P = 0.08), and fewer received indomethacin (8/37 vs 15/33; P = 0.03). At the study hospital where early extubation was practised, more dexamethasone treated infants were extubated during the first week (10/22 vs 2/16, P < 0.03). There was no difference in IVH. No adverse effects occurred.
Lin 1999 - For the end-point of CLD at 28 d statistical significance favouring dexamethasone was reached when 12 consecutive pairs in which one infant had CLD and the other did not showed that 10 pairs favoured dexamethasone and 2 pairs favoured control. Data presented for 40 infants (20 in each group) show a lower incidence of CLD at 28 d in the dexamethasone group (n = 3) compared to n = 9 in the control group (P < 0.05). Duration of oxygen therapy was also shorter in the dexamethasone group, 7+/- 6 d vs 13 +/- 12 d (P < 0.05). Among the survivors 12/15 were extubated in the dexamethasone group compared to 9/16 in the control group at the end of the study. Infants in the treated group had transient hyperglycaemia and hypertension, but there were no differences between the groups for mortality, incidence of sepsis or intraventricular haemorrhage.
Mukhopadhyay 1998 - Oxygen requirement was lower in the treated group on days 3, 4 and 5 compared to the control group, although the differences were not statistically significant (P> 0.05). Mean duration of ventilation was shorter in the dexamethasone group (87 +/- 42 h) vs control group (120+/- 46 h); P value not given. There was 1 case of culture positive sepsis in the dexamethasone group and 2 in the control group. None of the babies developed BPD (definition not given). Four babies in the dexamethasone group developed a pneumothorax versus 3 in the control group. Survival was 60% in the treated group and 55% in the control group.
Rastogi 1996 - Ventilator variables at 5-14 days were significantly improved in those infants who received dexamethasone compared to those who received placebo. The effect seemed to be more marked in infants weighing < 1250 g at birth. Significantly more infants could be extubated by 14 days in the dexamethasone group (26/32 vs 14/32; P = 0.004). Dexamethasone therapy reduced the incidence of CLD at 28 days (odds ratio, 0.10, 95% confidence interval, 0.03 - 0.30) and eliminated CLD at 36 weeks post-conceptional age. Dexamethasone treated infants had a greater weight loss at 14 days (12.9% vs 3.7%; P = 0.01) and higher blood pressures from days 3-10. However, no differences were seen in time to regain birth weight, hypertension (one infant in each group), or incidence of intraventricular haemorrhage.
Romagnoli 1999 - The incidence of CLD at 28 d and 36 wk was significantly lower in the dexamethasone group than the control group ( P < 0.001). Infants in the dexamethasone group remained intubated and required oxygen therapy for a shorter period than those in the control group (P < 0.001). Hyperglycaemia, hypertension, growth failure and hypertrophy of the left ventricle were transient side effects of early steroid administration. There were no significant differences in the rates of cerebral palsy, blindness, deafness, or intellectual impairment, or in mean IQ, or in the combined rate of death or cerebral palsy (Romagnoli 2002).
Sanders 1994 - The dexamethasone group required less ventilatory support (mean airway, peak respiratory and end-expiratory pressures, and intermittent mandatory ventilation) and supplemental oxygen after study day 4 (all P < 0.05, repeated measures analysis of variance). Improved tidal volume in the dexamethasone group, as assessed by pulmonary function testing of infants who remained intubated, was seen on study day 7 (P = 0.02, t test). The dexamethasone group required a shorter time in hospital (median 95 days vs 106 days, P = 0.01, proportional hazards regression). Survival in the dexamethasone group was 89% vs 67% in the placebo group (P = 0.08, chi squared analysis). Survival without CLD was 68% in the dexamethasone vs 43% in the placebo group (P = 0.14). Mean blood pressure was elevated on study day 4 to 7. No differences in the rate of hyperglycaemia, incidence or severity of IVH, or days to regain birth weight were seen. There were no significant differences in the rates of cerebral palsy, blindness, deafness, or intellectual impairment, or in the combined rate of death or cerebral palsy (Sinkin 2002).
Shinwell 1996 - No differences were found in any outcome variable except for a reduction in the need for mechanical ventilation at three days in dexamethasone treated infants (54/122, 44% vs 71/106, 67%; P = 0.001). Gastrointestinal haemorrhage, hypertension and hyperglycaemia were more common in treated infants, but no life threatening complications, such as gastrointestinal perforation, were encountered. Follow-up of survivors at two to six years showed no significant differences in the rates of blindness, deafness, major neurosensory disability, or in the combined rate of death or major neurosensory disability. However, there were significant increases in the rates of abnormal neurologic exam, developmental delay, and cerebral palsy. There was also a significant increase in the combined rate of death or cerebral palsy (Shinwell 2000).
Sinkin 2000 - No differences were found in the dexamethasone and placebo groups respectively for the primary outcomes of survival (79% vs 83%), survival without oxygen at 36 weeks corrected age (both 59%), and survival without oxygen at 36 weeks corrected age and without late steroids (46% vs 44%). No significant differences between the groups were found for median days in oxygen (50 vs 56 days), ventilation (20 vs 27 days), days to regain birth weight (15.5 vs 15.0 days), nor length or stay (88 vs 89 days). Babies given early dexamethasone were less likely to receive late steroids for BPD during their hospital stay (25 vs 35%, P = 0.042). No clinically significant side-effects were noted in the dexamethasone group although there were transient elevations in blood glucose and blood pressure with return to base-line by study day 10. Among infants who died (40 vs 33), there were no differences in the median days on oxygen, ventilation or length of hospital stay. However, in survivors (149 vs 162), the following were observed : median days on oxygen 37 vs 45, ventilation 14 vs 19 d, and length of stay 79 vs 81 d, for the dexamethasone versus placebo groups, respectively. There were no significant differences in the rates of cerebral palsy, or in the combined rate of death or cerebral palsy, or in mean Bayley scores (Sinkin 2002).
Soll 1999 - There were no differences in the primary outcome of CLD or death at 36 weeks adjusted age (early therapy 136/272 vs 143/270; P = 0.50). Infants who received early steroid therapy were less likely to need late treatment (114/272 vs 165/270; P < 0.001). They also had a lower risk of PDA; 92/272 vs 116/270; P < 0.05) and were less likely to receive indomethacin therapy (131/272 vs 178/270; P < 0.001). However, infants who received early steroid therapy were more likely to have complications such as gastrointestinal haemorrhage, (33/272 vs 19/270; P < 0.05), hyperglycaemia (201/272 vs 154/270; P < 0.001), and use of insulin therapy (169/272 vs 103/270; P < 0.001). There was a trend toward increased gastrointestinal perforation (30/272 vs 19/270; P < 0.01 ). In infants who had cranial ultrasound scans there was an increase in PVL in the early steroid group (7% vs 3%; P< 0.05). Infants who received early steroid therapy had fewer days in supplemental oxygen but they experienced poorer weight gain.
Stark 2001 - The steroid treated infants had a lower incidence of the primary outcome, death or CLD at 36 post-menstrual weeks (63% vs 69%; P < 0.05). Fewer infants in the steroid group had pulmonary interstitial emphysema (9% vs 23%; P < 0.05), required oxygen at 28 days (78% vs 94%; P < 0.05) or had subsequent steroid treatment (34% vs 51%; P < 0.05). The rates of severe IVH, PVL, ROP and nosocomial infection were similar. Hypertension and hyperglycaemia were more frequent in the steroid group (27% vs 4% and 23% vs 12% respectively with both P < 0.05). During the first 14 days 14/111 (13%) infants in the steroid group and 3/109 (3%) infants in the placebo group had spontaneous gastrointestinal perforation without NEC (P < 0.05). Spontaneous perforation was also associated with indomethacin treatment ( P = 0.005) and there was an interaction between indomethacin and steroid therapy (P = 0.04). There were no significant differences in the rates of cerebral palsy, developmental delay, major neurosensory disability, the combined rate of death or cerebral palsy, or the combined rate of death or major neurosensory disability (Stark 2001).
Subhedar 1997 - There was no difference in the combined incidence of CLD and/or death before discharge from hospital between either infants treated with dexamethasone and controls (RR 0.95, 95% CI 0.79-1.18) or those treated with inhaled NO and controls (RR 1.05, 95% CI 0.84-1.25). There were no significant differences in the rates of cerebral palsy, blindness, deafness, developmental delay, the combined rate of death or cerebral palsy, or the combined rate of death or major neurosensory disability (Subhedar 2000, Subhedar 2002).
Suske 1996 - Infants in the dexamethasone group were extubated earlier (6.6 d vs 14.2 d; P < 0.02) and required less time in supplemental oxygen (4.2 d vs 12.5 d; P < 0.02); pulmonary complications tended to be lower in the dexamethasone group (1/14 vs 4/12), as was the frequency of retinopathy of prematurity (2/14 vs 6/12; P < 0.05).
Tapia 1998 - There were no significant differences in mortality and/or CLD between the groups. There was a significant reduction in the number of infants requiring oxygen at 36 weeks postmenstrual age in the dexamethasone group (8% vs 33%; P < 0.05). Stepwise logistic regression analysis with oxygen dependency at 36 weeks as the dependent variable and birth weight, gestational age, gender, prenatal steroids and study treatment as the independent variables showed that study treatment was the only variable significantly associated with oxygen dependency at 36 weeks. There were no differences in the number of days of mechanical ventilation and oxygen treatment between the groups. There were no differences in the incidences of major morbidity and possible complications related to steroid administration, except for a lower incidence of NEC in the dexamethasone group.
Wang 1996 - Dexamethasone treatment decreased fractional inspired oxygen concentration, arterial carbon dioxide tension, mean airway pressure and facilitated successful weaning from mechanical ventilation. SP-A concentrations in tracheal aspirates were increased at day 7 and 14, and SP-D concentrations were increased during the period from days 3 - 14 in the dexamethasone treated group, compared with the control group.
Watterberg 1999 - More infants treated with hydrocortisone survived without supplemental oxygen at 36 weeks post-conception (12/20 vs 7/20; P = 0.023). Hydrocortisone treatment was also associated with a reduction in duration of oxygen > 40% (7 vs 28 days; P = 0.06), duration of oxygen > 25% (48 vs 69 days; P = 0.02) and duration of mechanical ventilation (25 vs 32 days; P = 0.03). There were no differences in the rates of death, sepsis, PDA, NEC, gastrointestinal perforation, IVH or ROP. There were no significant differences in the rates of cerebral palsy, blindness, deafness, or the combined rate of death or cerebral palsy (Watterberg 2002).
Yeh 1990 - Infants in the dexamethasone group
had significantly higher pulmonary compliance, tidal volume and minute
ventilation, and required lower mean airway pressure for ventilation than
infants in the placebo group. The endotracheal tube was successfully removed
from more infants in the dexamethasone group (16/28 vs 8/29; P < 0.025)
at two weeks of age. Nineteen infants (65%) in the placebo group and 11
(39%) in the dexamethasone group (P < 0.05) had lung injuries characterised
by:
1. surviving infants with CLD
2. infants who died of intractable respiratory failure and had evidence
of CLD at autopsy, and
3. infants who died of intractable respiratory failure with clinical
evidence of CLD
Dexamethasone therapy was associated with a temporary increase in blood
pressure and plasma glucose concentration and a delay in somatic growth.
Yeh 1997 - Infants in the dexamethasone group had a significantly lower incidence of CLD than those in the placebo group judged either at 28 postnatal days (21/132 vs 40/130, P < 0.05) or at 36 post-conceptional weeks (20/132 vs 37/130, P < 0.05). More infants in the dexamethasone group were extubated during the study. There was no difference between the groups for mortality (39/130 vs 44/132); however a higher proportion of infants in the dexamethasone group died in the late study period, probably attributable to infection. There was no difference between the groups for duration of oxygen therapy and hospitalisation. Significantly more infants in the dexamethasone group had either bacteraemia or clinical sepsis (44/132 vs 27/130, P < 0.05). Other immediate but transient side effects observed in the dexamethasone group were hyperglycaemia, hypertension, cardiac hypertrophy, hyperparathyroidism and delay in growth rate. There were no significant differences in the rates of blindness, developmental delay, major neurosensory disability, the combined rate of death or cerebral palsy, or the combined rate of death or major neurosensory disability. However, there were significant increases in the rates of abnormal neurologic exam and cerebral palsy among survivors (Yeh 1998).
Meta-analysis of these twenty-one studies of early post-natal corticosteroid treatment shows the following results:
• Mortality - There was no evidence that early postnatal steroid treatment reduced mortality either at 28 days (typical relative risk 1.05, 95% CI 0.90, 1.22; 18 studies and 2900 infants), before discharge (typical relative risk 1.02, 95% CI 0.90, 1.17; n=21 and 3068 respectively), or at the latest age possible to determine the outcome (typical relative risk 1.01, 95% CI 0.89, 1.15; n=21 and 3068 respectively).
• Chronic lung disease - Early steroids reduced the incidence of chronic lung disease defined as needing oxygen supplementation at either 28 days (typical relative risk 0.85, 95% CI 0.79, 0.92; typical risk difference -0.07, 95% CI -0.11, -0.04; n=16 and 2621) or 36 weeks' postmenstrual age (typical relative risk 0.69, 95% CI 0.60, 0.80; typical risk difference -0.09, 95% CI -0.12, -0.05; n =15 and 2415). There was also a reduction in CLD at 36 weeks in survivors (typical relative risk 0.72, 95% CI 0.63, 0.83; typical risk difference -0.10, 95% CI -0.14, -0.06; n =13 and 1789). However, there was no significant reduction in the proportion of survivors discharged home on oxygen, although there were fewer studies where this outcome could be determined (typical relative risk 0.75, 95% CI 0.53, 1.07; n =5 and 693). Early steroids reduced the need for later steroid treatment (typical relative risk 0.70, 95% CI 0.63, 0.78; typical risk difference -0.14, 95% CI -0.18, -0.10; n=9 and 1865).
• Death or chronic lung disease - Early steroids reduced the incidence of death or chronic lung disease defined as needing oxygen supplementation at either 28 days (typical relative risk 0.91, 95% CI 0.86, 0.96; typical risk difference -0.07, 95% CI -0.10, -0.03; n =15 and 2295) or 36 weeks' postmenstrual age (typical relative risk 0.86, 95% CI 0.79, 0.94; typical risk difference -0.07, 95% CI -0.11, -0.03; n =15 and 2415).
• Failure to extubate - Early steroids reduced the rates of failure to extubate at 3 days (typical relative risk 0.73, 95% CI 0.62, 0.86; typical risk difference -0.19, 95% CI -0.28, -0.10; n=3 and 381), 7 days (typical relative risk 0.76, 95% CI 0.66, 0.88; typical risk difference -0.12, 95% CI - 0.18, -0.06; n=6 and 963), 14 days (typical relative risk 0.77, 95% CI 0.62, 0.97; typical risk difference -0.10, 95% CI -0.19, -0.02; n=4 and 443) and at 28 days (typical relative risk 0.84, 95% CI 0.72, 0.99; typical risk difference -0.07, 95% CI -0.13, -0.01, n=7 and 902).
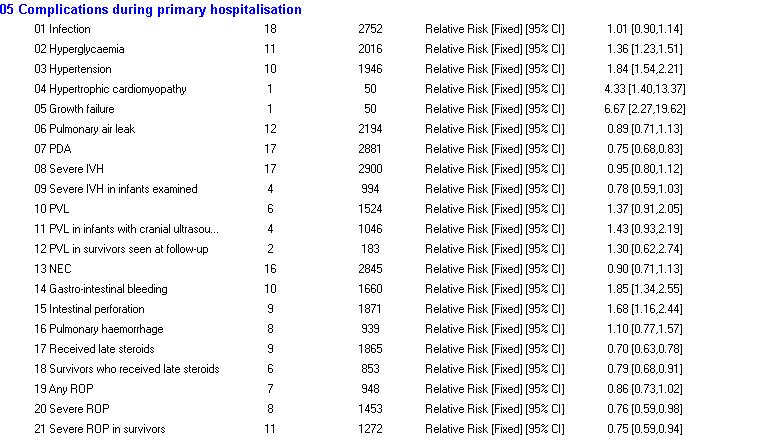
Complications during the primary hospitalisation were as follows:
• Metabolic complications - Early steroids increased the risk of hyperglycaemia (typical relative risk 1.36, 95% CI 1.23, 1.51; typical risk difference 0.11, 95% CI 0.08, 0.15; n=11 and 2016), and hypertension (typical relative risk 1.84, 95% CI 1.54, 2.21; typical risk difference 0.10, 95% CI 0.07, 0.13; n=10 and 1946).
• Gastro-intestinal complications - Early steroids increased the risks of gastro-intestinal bleeding (typical relative risk 1.90, 95% CI 1.35, 2.66; typical risk difference 0.06, 95% CI 0.03, 0.09; n=9 and 1440) and intestinal perforation (typical relative risk 1.98, 95% CI 1.32, 2.95, typical risk difference 0.04, 95% CI 0.01, 0.06; n=9 and 1871) but there was no evidence of effect on the incidence of necrotising enterocolitis (typical relative risk 0.87, 95% CI 0.62, 1.23; n=12 and 1582).
• Other effects - Early steroids increased the risk of hypertrophic cardiomyopathy (relative risk 4.33, 95% CI 1.40, 13.4; risk difference 0.40, 95% CI 0.17, 0.63; n=1 and 50) and growth failure (relative risk 6.67, 95% CI 2.27, 19.6; risk difference 0.68, 95% CI 0.48, 0.88; n=1 and 50) in one study where these were reported. Early steroids reduced the risk of patent ductus arteriosus (typical relative risk 0.75, 95% CI 0.68, 0.83; typical risk difference -0.10, 95% CI -0.14, -0.07; n=17 and 2881), but there was no significant effect on pulmonary air leaks (typical relative risk 0.89, 95% CI 0.71, 1.13; n=12 and 2194), severe intraventricular haemorrhage (typical relative risk 0.95, 95% CI, 0.80, 1.12; n=17 and 2900), pulmonary haemorrhage (typical relative risk 1.10, 95% CI 0.77, 1.57; n=8 and 939), periventricular leucomalacia (typical relative risk 1.37, 95% CI 0.91, 2.05; n=6 and 1524), infection (typical relative risk 1.01, 95% CI 0.90, 1.14; n=18 and 2752), or any retinopathy of prematurity (typical relative risk 0.86, 95% CI 0.73, 1.02; n=7 and 948). However, severe ROP was significantly reduced (typical relative risk 0.76, 95% CI 0.59, 0.98; risk difference -0.04, 95% CI -0.07, 0.00; n=8 and 1453).
Follow-up data were as follows:
• Follow-up studies are limited in number relative to the total number of studies.
• Developmental delay was increased with steroids in one study with the criteria for the diagnosis not explicit (relative risk 1.68, 95% CI 1.08, 2.61; risk difference 0.14, 95% CI 0.03, 0.24; n=1 and 248).
• Cerebral palsy was increased with steroids (typical relative risk 1.69, 95% CI 1.20, 2.38; typical risk difference 0.06, 95% CI 0.02, 0.11; n=9 and 991), but there was an increase of only borderline statistical significance in the combined outcome, death or cerebral palsy (typical relative risk 1.16, 95% CI 1.00, 1.34; typical risk difference 0.06, 95% CI 0.00, 0.12; p=0.05; n=6 and 991).
• There were non-significant effects on major neurosensory disability (typical relative risk 1.16, 95% CI 0.89, 1.52; n=4 and 772) and the combined outcome of death or major neurosensory disability (typical relative risk 1.07, 95% CI 0.93, 1.22; n=4 and 772).
• There was a significant increase in the rate of abnormal neurological exam (typical relative risk 1.81, 95% CI 1.33, 2.47; n=5 and 829) and in the combined outcome of death or abnormal neurological exam (typical relative risk 1.23, 95% CI 1.06, 1.42; n=5 and 829). Although the criteria for this diagnosis were vague and varied between studies, the size of the difference in this outcome in the trials where data were available was similar to the size of the difference in cerebral palsy in the corresponding study.
• There were no significant effects on other long-term outcomes of blindness, deafness, formal psychometric testing, abnormal EEG, behaviour problems, or rehospitalisation.
This review has demonstrated that early corticosteroid treatment facilitates weaning from the ventilator. Additional advantages are increased survival without CLD at 28 days and 36 weeks post-menstrual age, reductions in the risk of CLD at 28 days and at 36 weeks post-menstrual age, the need for late treatment with steroids, and PDA. On the other hand there are increases in the risk of gastrointestinal bleeding, intestinal perforation, hyperglycaemia, hypertension, hypertrophic cardiomyopathy and growth failure.
There are other potential hazards of corticosteroid treatment in the neonate including retardation of growth (Gibson 1993), protein breakdown (van Goudoever 1994), cardiac hypertrophy (Werner et al 1992) and possible adverse effects on development of the central nervous system (Weichsel 1977; Gramsbergen 1998) and lungs (Tschanz 1995). One study has shown a significant decline in the growth of head circumference with early corticosteroid treatment (Papile 1996). Long term follow-up results show that early dexamethasone treatment is associated with a significant increase in the risk of developmental delay and cerebral palsy, but borderline effects on the combined outcome of death or cerebral palsy. One of these studies used a four week tapering course of dexamethasone (Yeh 1997) and so is similar in duration to the six week tapering course of late steroids reported by O'Shea 1999 and included in the systematic review of delayed steroids. However, the follow-up study of Shinwell 1996 (Shinwell et al, 2000) reported adverse long term neurological outcomes in children treated with only a three day course of early dexamethasone starting within 12 hours of birth. This finding is of extreme importance and concern as there was about a three-fold increased risk of cerebral palsy in survivors and this included children with spastic diplegia, spastic quadriplegia and hemiplegia. Why dexamethasone given early for a short course should have such devastating effects is unknown. Certainly some infants would have been treated with repeat courses of dexamethasone but this would have been more likely in the control infants. Periventricular leucomalacia (PVL) is an obvious cause of cerebral palsy but studies have not shown a significant excess of this complication in steroid-treated infants compared with controls. Despite the increase in the diagnosis of cerebral palsy, in two separate studies and overall, of importance is the observation that this does not necessarily translate into major functional disability for the children concerned, in either of the two individual studies with a significant increase in cerebral palsy, or in all studies combined.
This systematic review finds that early (<96 hours) postnatal corticosteroids for preventing chronic lung disease in preterm infants, in the regimens used, have significant short and long-term effects, both beneficial and harmful. An important problem in interpreting the late follow-up data is that only nine of the 21 trials of early postnatal steroids have reported late follow-up results; therefore, the possibility of follow-up bias and publication bias must be considered. A limitation of the two studies with an increase in the rate of cerebral palsy (Shinwell 1996, Yeh 1997) is that only 84% and 81%, respectively, of surviving infants were examined. No study was designed primarily to test the effect of postnatal steroids on adverse long-term neurosensory outcome, and all were underpowered to detect clinically important differences in long-term neurosensory outcome. It is also important to remember that cerebral palsy has been diagnosed before the children were 5 years of age in most cases; diagnosing cerebral palsy with certainty before 5 years of age is problematic (Stanley 1982).
In a recent observational study of infants born after antenatal steroid therapy there appeared to be an excess of periventricular leucomalacia in those whose mothers had received dexamethasone rather than betamethasone (Baud 1999). Most studies of postnatal steroids have used dexamethasone in high doses of 0.5-1.0 mg/kg/day. Other steroids or lower doses of dexamethasone may prove to be safer. One study has suggested that low dose hydrocortisone has beneficial effects on the neonatal lung (Watterberg 1999). Further studies are probably needed comparing lower doses of steroids, other steroids and alternative routes of administration, e.g. by inhalation (see Cochrane Review by Shah 2000). These studies should include long term follow-up (see DART study; Doyle 2000a).
Future studies are also needed to accurately identify those infants most at risk of developing CLD. Any future placebo-controlled trials of postnatal steroids in preterm infants should include long term neurologic follow-up (see DART study; Doyle 2000a). Studies comparing different doses and durations of corticosteroid treatment, and examining the effects of inhaled steroids, are urgently needed. Studies of potentially safer steroids such as hydrocortisone (and possibly betamethasone or methylprednisolone) also need to be performed.
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Baden 1972 | Random allocation using random numbers and sealed envelopes. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes. Blinding of outcome measurement: yes. | 44 preterm infants < 24 hours old with respiratory distress both clinically and radiologically. | Hydrocortisone 25 mg/kg on admission and 12 hours later intravenously. Control group given placebo. | Death, FiO2, cortisol levels and blood gases. | The oldest study, carried out 1972. Used hydrocortisone in a very short course of treatment. | A |
| Biswas 2002 | Randomisation by Oxford Perinatal Trails Unit. Blinding of randomisation: yes; blinding of intervention: yes; blinding of outcome measurements: yes; complete follow-up: yes. | 253 babies < 30 weeks' gestation, within 9 hours of birth at entry; all mechanically ventilated | Hydrocortisone @ 1mg/kg/day as continuous infusion for 5 days, then 0.5 mg/kg/day for 2 days. Also given T3 @ 6 micrograms/kg/day for 5 days, halving to 3 micrograms/kg/day for 2 days. Controls given equal volume infusion of 5% dextrose. | The primary outcome was death or ventilator dependence at 7 days, or death or oxygen dependence at 14 days. Secondary outcomes included durations of ventilation, oxygen dependence and hospitalisation, oxygen dependency at 36 weeks, IVH, PVL, PDA and NEC | Hydrocortisone combined with T3 infusion | A |
| Garland 1999 | Randomisation by study pharmacists at each centre. Blinding of randomisation: yes; blinding of intervention: yes; blinding of outcome measurements: yes; complete follow-up: yes. | 241 infants weighing between 500 and 1500 g, received surfactant, at significant risk for CLD or death using a model to predict at 24 hours. | 3 day course of dexamethasone beginning at 24-48 hours. The first 2 doses were 0.4 mg/kg, 3rd and 4th doses 0.2 mg/kg and the 5th and 6th doses 0.1 mg/kg and 0.05 mg/kg respectively. Dexamethasone dose reduced slightly after first interim analysis. A similar volume of normal saline was given to control infants. | The primary outcomes were survival without CLD defined as oxygen therapy at 36 weeks to maintain SaO2 above 91% and mortality. Secondary outcomes included duration of ventilation and supplemental oxygen, respiratory support at 28 days, length of stay for survivors, use of subsequent dexamethasone therapy and usual complications of prematurity. | At the first interim analysis (n = 75) an increased risk of GI perforation was noted in the dexamethasone group. The data monitoring committee recommended reducing the dexamethasone dose to: 4 doses of 0.25 mg/kg/dose every 12 hours begun at 24 - 48 hours followed by doses of 0.125 mg/kg and 0.05 mg/kg at the next 2 12 hour periods respectively. | A |
| Halac 1990 | Random allocation using list of random numbers.
Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes. Blinding of outcome measurement: yes. |
248 infants, BW <= 1500 g, GA <34 wks, with evidence of "birth asphyxia" (1 minute Apgar score <5, prolonged resuscitation and metabolic acidosis [HCO3 <15 mmol/l within 1 hour of birth]). | 7 day course of dexamethasone 1 mg/kg 12 hourly beginning on day of life 1 | Neonatal mortality, mortality to discharge, NEC, PDA, sepsis and severe IVH | Possible exclusion of 5 deaths after randomisation but not clear which group they came from. | A |
| Kopelman 1999 | Random allocation in the hospital pharmacy stratified by use of antenatal steroids Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes. Blinding of outcome measurement: yes. | 70 infants of < 28 weeks gestation requiring intermittent mandatory ventilation and arterial catheterisation. | Dexamethasone 0.2 mg/kg within 2 hours of delivery. Control infants given an equal volume of saline. | Ventilation Index (VI), IMV rate, mean blood pressure, incidence of PDA, need for indomethacin and number extubated during the first week and usual complications of RDS. | After an interim analysis showed that the incidence of IVH was much
lower than expected, enrollment was stopped and the analysis was limited
to a comparison of ventilator settings, blood pressure and pressor use
during the first 7 days.
The outcome of successful extubation was available at only one hospital were 38 infants were enrolled. |
A |
| Lin 1999 | Random allocation in a paired sequential trial. Assignment determined by pharmacist and groups stratified by birthweight: 500-999 g, 1000 - 1500 g and 1501 - 1999 g. Blinding of randomisation: yes; blinding of intervention: yes; blinding of outcome measurement: yes; complete follow-up: yes. | 40 infants of 500-1999 g with severe RDS, needing IPPV within 6 h of birth. | Dexamethasone 0.25 mg/kg 12 hourly from 1 - 7 d, 0.12 mg/kg 12 hourly from 8 - 14 d, 0.05 mg/kg 12 hourly from 15-21 d, 0.02 mg/kg 12 hourly from 22 - 28 d. Saline placebo was given to controls. | Mortality at 28 d and discharge, failure to extubate (during study), death or CLD (36 wk), CLD (28 d and 36 wk), infection (clinical), severe IVH, plasma glucose and mean blood pressure on d 2,5,7 and 16, weight at 2 wk. | Sequential analysis for 12 pairs. Data given for 40 infants as randomised into the 2 groups. | A |
| Mukhopadhyay 1998 | Random allocation, method not stated. Blinding of randomisation: not sure; blinding of intervention: not sure; blinding of outcome measurement: not sure; complete follow-up: yes. | 19 infants < 34 weeks and < 2000 g who could be provided with ventilation. Clinical and radiographic evidence of RDS, IPPV with oxygen > 30%. | Dexamethasone 0.5 mg/kg per dose 12 hourly for 3 days starting within 6 hours of birth. The control group did not receive any drug. | Changes in oxygen requirements, mean duration of ventilation, culture positive sepsis, PDA, BPD (not defined), pneumothorax, mortality. | Babies were only entered into the trial if a ventilator was available. Surfactant was not given. | B |
| Rastogi 1996 | Random allocation: using a pharmacy list, stratified for birthweight. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes. Blinding of outcome measurement: yes. | 70 preterm infants < 12 h old, weighing 700 - 1500 g with RDS clinically and radiologically, babies needed mechanical ventilation > 30% O2 and / or MAP 7 cmH2O a/A < 0.25 after surfactant treatment. Exclusions for major malformations, chromosome abnormalities, severe infection, Apgar < 3 at 5 minutes | Intravenous dexamethasone 0.5 mg/kg/day for 3 days, 0.25 mg/kg/day for 3 days, 0.15 mg/kg/day for 3 days, 0.05 mg/kg/day for 3 days. Control group given saline placebo. | FiO2, MAP, BPD (28 days and CXR), severe BPD (36 weeks), duration O2, infections, deaths, PTX, PH, PDA, IVH, NEC, Hyperglycemia, insulin use, hypertension, ROP | A | |
| Romagnoli 1999 | Random allocation using random numbers concealed in numbered sealed envelopes. Blinding of randomisation: yes; blinding of intervention: probably no; blinding of outcome measurements: not sure; complete follow-up: yes. | 50 infants < 1251 g or < 33 weeks, oxygen dependent at 72 h and at high risk of CLD according to a scoring system predicting 90% risk of CLD. | Dexamethasone 0.5 mg/kg/day for 3 days, 0.25 mg/kg/day for 3 days and 0.125 mg/kg/day for 1 day. Control group: no mention of placebo | Survival to 28 days, survival to discharge, PDA, IVH grades 3 & 4, PVL, sepsis, NEC, ROP grades III and above, requiring ventilation at 28 d, CLD at 28 d & 36 wk, hyperglycaemia, hypertension, needed late steroids, growth failure and LVH | A | |
| Sanders 1994 | Random allocation in the Pharmacy using sealed envelopes. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes. Blinding of outcome measurement: yes. | 40 babies < 30 weeks gestation and 12-18 hours old with RDS, both clinical and radiological. The babies were being treated with mechanical ventilation and surfactant and exclusions comprised sepsis, congenital heart disease, chromosome abnormalities or need for exchange transfusion. | Dexamethsone 0.5 mg/kg twice intravenously. Control group given saline placebo. | MAP, FiO2, mortality, extubation < 7 days, PFT, duration IPPV, O2, hospital, mortality, BPD (36 weeks O2), late steroids | A | |
| Shinwell 1996 | Random allocation, stratified by centre and birthweight, from random numbers list in Pharmacy. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes for short term. 84% for long term. Blinding of outcome measurement: yes. | 248 preterm babies with birthweight 500 - 2000 g, 1-3 days old, requiring mechanical ventilation with more than 40% oxygen. Exclusions for active bleeding, hypertension, hyperglycaemia, active infection and lethal congenital anomalies | Intravenous dexamethasone 0.25 mg/kg every 12 h six times. Controls given saline placebo. | Mortality, survival with no O2, MV3 and 7 days, CLD, duration hospital, IVH, PVL, RIO PTX PIE, PDA, sepsis, hypertension, hyperglycaemia | A | |
| Sinkin 2000 | Random allocation in the pharmacy with labelled syringes. Stratification by centre. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes. Blinding of outcome measurement: yes. | 384 babies < 30 weeks' gestation with RDS by clinical and radiographic signs, needing IPPV at 12-18 h of age and had received at least 1 dose of surfactant. | Dexamethsone 0.5 mg/kg at 12-18 hours of age and second dose 12 hours later. Control group given an equal volume of placebo. | Primary outcomes were survival, survival without oxygen at 28 d or 36 wk, and survival without oxygen at 28 d or 36 wk and without late steroids. Length of time in oxygen, on ventilation, to regain birthweight and in hospital. Hyperglycaemia, hypertension, IVH, PDA, sepsis, NEC, isolated intestinal perforation, ROP, air leak, discharged home on oxygen. | A | |
| Soll 1999 | Random allocation in hospital pharmacies by opening opaque sealed envelopes. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes. Blinding of outcome measurement: yes. | 542 infants weighing 501 - 1000 g who required assisted ventilation < 12 h, had received surfactant by 12 hours, were physiologically stable and had no life threatening congenital anomalies. | Dexamethasone 0.5 mg/kg/day for 3 days. 0.25 mg/kg /day for 3 days,
0.10 mg/kg/day for 3 days and 0.05 mg/kg/day for 3 days. Control infants
received a similar volume of normal saline.
Infants in either group could receive late post-natal steroids beginning on day 14 if they were on assisted ventilation with supplemental oxygen > 30%. |
Primary outcome was CLD or death at 36 weeks adjusted age. Secondary outcome measures included clinical status at 14 days and 28 days, duration of assisted ventilation, supplemental oxgyen and hospital stay, treatment with late postnatal steroids, proven sepsis, hypertension and hyperglycaemia requiring therapy, weight at 36 weeks and the usual complications of prematurity. | Published as an extended abstract and presented at a clinical meeting. | A |
| Stark 2001 | Random allocation using random numbers list supplied to pharmacy, stratified by birth weight. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes, blinding of outcome measurements: yes. | 220 infants with birthweight 501 - 1000 g mechanically ventilated < 12 h. Infants > 750 g also need to receive surfactant and have FiO2 > 0.29. | Dexamethasone 0.15 mg/kg/day for 3 days, then tapered over 7 days or saline placebo. | Death or CLD, oxygen at 28 d PIE, late steroid treatment, hypertension, hyperglycaemia, GI perforation. | Factorial design, infants also randomised to routine ventilator management
or a strategy of minimal ventilator support to reduce mechanical lung injury.
After enrolling 220 infants (sample size estimate was 1200) the trial was halted for unanticipated adverse events. |
A |
| Subhedar 1997 | Random allocation by computer generated random numbers and sealed envelopes. Factorial design provided 4 groups: early dexamethasone, inhaled NO, both drugs together and neither drug. Blinding of randomisation: yes. Blinding of intervention: probably not. Complete follow-up: yes. Blinding of outcome measurements: probably not. | 42 preterm babies, entry at 96 hours if gestation < 32 weeks, mechanical ventilation from birth, surfactant treatment and high risk of developing CLD by a score (Ryan et al 1996). Exclusion criteria: major congenital anomaly, structural cardiac defect, significant ductus shunting, culture positive sepsis, IVH with parenchymal involvement, pulmonary or gastrointestinal haemorrhage, abnormal coagulation, or thrombocytopenia (platelets < 50,000). | Intravenous dexamethasone at 12 hourly intervals for 6 days; 0.5 mg/kg/dose for 6 doses and 0.25 mg/kg/dose for a further 6 doses. Inhaled NO 5-20 ppm for 72 hours. Control groups were not given a placebo. | Mortality, CLD at 28 days and > 36 weeks with abnormal chest radiograph. Duration of ventilation, time to extubation, duration of hospitalisation, maximum grade of IVH, pulmonary haemorrhage, pneumothorax, severe PDA, NEC, stage III or IV ROP. Complications including ileal perforation, upper GI haemorrhage, hyperglycaemia, hypertension, septicaemia. | Note factorial design which means that half of the treated and half of the control infants also received 72 hours of inhaled NO. | A |
| Suske 1996 | Random allocation using sealed envelopes. Blinding of randomisation: yes, blinding of intervention: probably not. Complete follow-up: yes. Blinding of outcome measurement: probably not. | 26 preterm infants < 2 h old, with birthweight < 1500 g if FiO2 > 0.50, or > 1500 g birthweight with FiO2 0.70, exclusion for known sepsis, cardiac anomalies, malformations of lung or CNS | Intravenous dexamethasone 0.5 mg/kg/day for 5 days. Controls were not given a placebo. | Blood gases, ventilator settings, mortality IVH, BPD (O2 28 days), NEC, late sepsis, PDA, ROP, air leak, duration hospital | A | |
| Tapia 1998 | Random allocation using ampoules of dexamethasone and saline prepared in the hospital pharmacy. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: almost (109/113). Blinding of outcome measurement: yes. | 113 (4 exclusions for congenital abnormality, early sepsis and failure to obtain follow-up data) infants with birthweight between 700 and 1600 g, clinical and radiological diagnosis of RDS, needing mechanical ventilation and < 36 hours of age. Exclusion criteria were life-threatening congenital malformation or chromosome abnormality, a strong suspicion of infection at birth (maternal chorioamnionitis), or early sepsis (positive blood culture in the first 36 hours of life). | Intravenous dexamethasone 0.5 mg/kg/day for 3 days, 0.25 mg/kg for 3 days, 0.12 mg/kg/day for 3 days and 0.06 mg/kg/day for 3 days. The placebo group received an equivalent volume of saline solution. | The primary outcomes were death before hospital discharge, BPD (defined as oxygen need at 28 days and x-ray changes), death or BPD and oxygen need at 36 weeks. Other outcomes included time on ventilator, time in over 40% oxygen and time in oxygen. Major morbidity and complications included pneumothorax, PIE, PDA, pulmonary haemorrhage, pneumonia, sepsis, NEC, ROP, arterial hypertension, hyperglycaemia and IVH (grades I-II, and III-IV). | A | |
| Wang 1996 | Random allocation in a double-blind fashion, method not stated. Blinding of randomisation: yes; blinding of intervention: yes; blinding of outcome measurements: yes; complete follow-up: yes. | 63 infants with birthweights from 1000 to 1999 g, AGA, clinical and radiographic RDS, IPPV (0-12 age after birth), | Dexamethasone 0.25 mg/kg 12 hourly from 1 to 7 d, 0.125 mg/kg 12 hourly from 8 to 14 d, 0.05 mg/kg, 12 hourly from 15 to 21 d. First dose administered < 12 h. Controls received saline placebo. | Oxygen requirements, PCO2, MAP, SP-A and SP-D in tracheal aspirate, failure to extubate by 3rd d, 7th d, 14th d and 28th d, mortality before discharge, sepsis, CLD at 28 d. | A | |
| Watterberg 1999 | Random allocation at each centre by constant block design with 4 patients
per block to minimse bias over time. Separate randomisation tables were
used for infants exposed to antenatal
steroids. Randomisation was probably performed in hospital pharmacies. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: yes. Blinding of outcome measurement: yes. |
40 infants weighing between 500 and 999 g who were appropriate for gestational age and needed mechanical ventilation < 48 hours of age. Exclusion criteria included maternal diabetes, congenital sepsis and SGA. | Hydrocortisone 1.0 mg/kg/day every 12 hours for 9 days, 0.5 mg/kg/day for 3 days. Control infants were given an equal volume of normal saline. | The primary outcome was survival without supplemental oxygen at 36 weeks post conception. Secondary outcomes included in survivors; CLD at 36 weeks, duration of mechanical ventilation, > 40% oxygen, > 25% coxygen, hospital stay, and weight and head circumference at 36 weeks. | A | |
| Yeh 1990 | Random allocation in blocks of ten using a Pharmacy list. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: almost. Blinding of outcome measurements: yes. | 57 preterm infants weighing between 700 and 1999 g, < 13 hours old with severe RDS both clinically and radiologically. They needed mechanical ventilation < 4 h and were excluded if they had infection. | Intravenous dexamethasone 0.5 mg/kg/day for 3 days, 0.25 mg/kg/day for 3 days, 0.12 mg/kg/day for 3 days, 0.05 mg/kg/day for 3 days. Control infants were given saline placebo. | MAP, FiO2, PFT, BP, glucose, mortality, CLD, duration O2, hospital, weight loss, sepsis, PDA, IVH > grade I, ROP | A | |
| Yeh 1997 | Random allocation by central pharmacy random number list. Blinding of randomisation: yes. Blinding of intervention: yes. Complete follow-up: Almost for short term. 81% for long term. Blinding of outcome measurement: yes. | 262 babies of birthweight < 2000 g with RDS and requiring mechanical ventilation after birth. | Dexamethasone 0.25 mg/kg/dose every 12 hours intravenously on days 1-7; 0.12 mg/kg/dose every 12 hours intravenously from 8-14 days; 0.05 mg/kg/dose every 12 hours intravenously from day 15 to 21; and 0.02 mg/kg/dose every 12 hours intravenously from days 22 to 28. Control infants were given saline placebo. | Chronic lung disease either judged at 28 postnatal days or at 36 post-conceptional weeks. Extubation during the study, mortality, bacteraemia or clinical sepsis, and side effects of hyperglycaemia, hypertension, cardiac hypertrophy, hyperparathyroidism and growth failure. | A |
| Study | Reason for exclusion |
| Gaissmaier 1999 | Primary outcome was need for an epinephrine infusion 12 hours after treatment. No longterm outcomes reported. |
| Tsukahara 1999 | Not a RCT; 26 study infants and 12 historical controls. Early was defined just outside range of up to 4 days (4-7 days) |
| Study | Trial name or title | Participants | Interventions | Outcomes | Starting date | Contact information | Notes |
| Doyle 2000a | Postnatal dexamethasone in tiny babies: Does it do more good than harm? | Extremely low birthweight (<1000g) or very preterm (<28 weeks) infants who are ventilator-dependent after 7 days of age | Dexamethasone 0.15 mg/kg/day for 3 days, 0.1 mg/kg/day for 3 days, 0.05 mg/kg/day for 2 days, 0.02 mg/kg/day for 2 days | Reduction in the rates of ventilator dependence and chronic lung disease, without adversely affecting either mortality or sensorineural impairments or disabilities at two years of age | February 2000 | Dr. Lex Doyle, The Royal Women's Hospital, email lwd@unimelb.edu.au, phone 61 3 9344 2151, fax 61 3 9347 1761 | Intake ceased Nov 1 2002 due to lack of recruitment. |
* Baden M, Bauer CR, Cole E, Klein G, Taeusch HW, Stern L. A controlled trial of hydrocortisone therapy in infants with respiratory distress syndrome. Pediatrics 1972;50:526-534.
Fitzhardinge PM, Eisen A, Lejtenyi C, Metrakos K, Ramsay M. Sequelae of early steroid administration to the newborn infant. Pediatrics 1974;53:877-83.
Biswas 2002 {published data only}
Biswas S. Personal communication. 2002.
* Biswas S, Buffery J, Enoch H, Markiewicz M, Walters D. The pulmonary effects of triiodothyronine (T3) and hydrocortisone (HC) supplementation in preterm infants less than 30 weeks gestation. Results of the THORN trial - Thyroid Hormone Replacement in Neonates. Pediatr Res 2002;(in press).
Garland 1999 {published data only}
Garland JS, Alex CP, Pauly TH, Whitehead VL, Brand J, Winston JF, Samuels DP, McAuliffe TL. A three-day course of dexamethasone therapy to prevent chronic lung disease in ventilated neonates: a randomized trial. Pediatrics 1999;104:91-99.
Halac 1990 {published data only}
Halac E, Halac J, Begue EF, et al. Prenatal and postnatal corticosteroid therapy to prevent neonatal necrotizing enterocolitis: A controlled trial. J Pediatr 1990;117:132-8.
Kopelman 1999 {published data only}
Kopelman AE, Moise AA, Holbert D, Hegemier SE. A single very early dexamethasone dose improves respiratory and cardiovascular adaptation in preterm infants. J Pediatr 1999;135:345-350.
Lin 1999 {published data only}
Lin YJ, Yeh TF, Hsieh WS, Chi YC, Lin HC, Lin CH. Prevention of chronic lung disease in preterm infants by early postnatal dexamethasone therapy. Pediatr Pulmonol 1999;27:21-26.
Mukhopadhyay 1998 {published data only}
Mukhopadhyay K, Kumar P, Narang A. Role of early postnatal dexamethasone in respiratory distress syndrome. Indian Pediatrics 1998;35:117-122.
Rastogi 1996 {published data only}
* Rastogi A, Akintorin SM, Bez ML, Morales P, Pildes PS. A controlled trial of dexamethasone to prevent bronchopulmonary dysplasia in surfactant-treated infants. Pediatrics 1996;98:204-210.
Morales P, Rastogi A, Bez ML, Akintorin SM, Pyati S, Andes SM, Pildes RS. Effect of dexamethasone therapy on the neonatal ductus arteriosus. Pediatr Cardiol 1998;19:225-229.
Romagnoli 1999 {published data only}
Romagnoli C, Zecca E, Vento G, Maggio L, Papacci P, Tortorolo G. Effect on growth of two different dexamethasone courses for preterm infants at risk of chronic lung disease. Pharmacology 1999;59:266-274..
* Romagnoli C, Zecca E, Vento G, De Carolis MP, Papacci P, Tortorolo G. Early postnatal dexamethasone for the prevention of chronic lung disease in high risk infants. Intens Care Med 1999;25:717-721.
Romagnoli C, Zecca E, Luciano R, Torrioli G, Tortorolo G. Controlled trial of early dexamethasone treatment for the prevention of chronic lung disease in preterm infants: a 3-year follow-up. Pediatrics 2002;109:e85.
Sanders 1994 {published data only}
* Sanders RJ, Cox C, Phelps DL, Sinkin RA. Two doses of early intravenous dexamethasone for the prevention of bronchopulmonary dysplasia in babies with respiratory distress syndrome. Pediatr Res 1994;36:122-128.
Sinkin RA. Personal communication. 2002.
Shinwell 1996 {published data only}
* Shinwell ES, Karplus M, Zwora E et al. Failure of early postnatal dexamethasone to prevent chronic lung disease in infants with respiratory distress syndrome. Arch Dis Child 1996;74:F33-37.
Shinwell ES, Karplus M, Reich D et al. Early dexamethasone therapy is associated with increased incidence of cerebral palsy. In: Hot Topics in Neonatology. Ross Laboratories, 1999:240-254.
Shinwell ES, Karplus M, Reich D et al. Early postnatal dexamethasone treatment and incidence of cerebral palsy. Arch Dis Child 2000;83:F177-F181.
Shinwell ES. Personal communication. 2002.
Sinkin 2000 {published data only}
* Sinkin RA, Dweck HS, Horgan MJ, Gallaher KJ, Cox C, Maniscalco WM, Chess PR, D'Angio CT, Guillet R, Kendig JW, Ryan RM, Phelps DL. Early dexamethasone - Attempting to prevent chronic lung disease. Pediatrics 2000;105:542-548.
D'Angio CT, Maniscalco WM, Ryan RM et al. Vascular endothelial growth factor in pulmonary lavage fluid from premature infants: effects of age and postnatal dexamethasone. Biol Neonate 1999;76:266-273.
Sinkin RA. Personal communication. 2002.
Soll 1999 {published data only}
Soll RF for the Vermont Oxford Network Steroid Study Group. Early postnatal dexamethasone therapy for the prevention of chronic lung disease. Pediatr Res 1999;45:226A.
Stark 2001 {published data only}
* Stark AR, Carlo WA, Tyson JE, Papile LA, Wright LL, Shankaran S, Donovan EF, Oh W, Bauer CR, Saha S, Poole WK, Stoll BJ. National Institute of Child Health and Human Development Neonatal Research Network.. Adverse effects of early dexamethasone in extremely-low-birth-weight infants.. N Engl Med J 2001;344:95-101.
Stark AR, Carlo W, Vohr BR, Papile L, Bauer C, Donovan E, Oh W, Shankaran S, Tyson JE, Wright LL, Saha S, Poole K. National Institute of Child Health and Human Development Neonatal Research Network. Neurodevelopmental outcome and growth at 18-22 months in infants treated with early dexamethasone. Pediatr Res 2001;(49):388A.
Subhedar 1997 {published data only}
* Subhedar NV, Ryan SW, Shaw MJ. Open randomised controlled trial of inhaled nitric oxide and early dexamethasone in high risk preterm infants. Arch Dis Child 1997;77:F185-F190.
Subhedar NV, Bennett AJ, Wardle SP, Shaw NJ. More trials on early treatment with corticosteroids are needed. Brit Med J 2000;320:941.
Subhedar NV. Personal communication. 2002.
Suske 1996 {published data only}
Suske G, Oestreich K, Varnholt V, Lasch P, Kachel W. Influence of early postnatal dexamethasone therapy on ventilator dependency in surfactant-substituted preterm infants. Acta Paediatr 1996;85:713-718.
Tapia 1998 {published data only}
Tapia JL, Ramirez R, Cifuentes J, Fabres J, Hubner ME, Bancalari A, Mercado ME, Standen J, Escobar M. The effect of early dexamethasone administration on bronchopulmonary dysplasia in preterm infants with respiratory distress syndrome. J Pediatr 1998;132:48-52.
Wang 1996 {published data only}
Wang JY, Yeh TF, Lin YJ, Chen WY, Lin CH. Early postnatal dexamethasone therapy may lessen lung inflammation in premature infants with respiratory distress syndrome on mechanical ventilation. Pediatr Pulmonol 1997;23:193-197.
* Wang J-Y, Yeh T-F, Lin Y-C, Miyamura K, Holmskov U, Reid KB.. Measurement of pulmonary status and surfactant protein levels during dexamethasone treatment of neonatal respiratory distress syndrome. Thorax 1996;51:907-913.
Watterberg 1999 {published data only}
* Watterberg KL, Gerdes JS, Gifford KL, Lin H-M. Prophylaxis against early adrenal insufficiency to prevent chronic lung disease in premature infants. Pediatrics 1999;104:1258-1263.
Watterberg KL. Personal communication. 2002.
Yeh 1990 {published data only}
Yeh TF, Torre JA, Rastogi A, Anyebuno MA, Pildes RS. Early postnatal dexamethasone therapy in premature infants with severe respiratory distress syndrome: a double-blind, controlled study. J Pediatr 1990;117:273-282.
Yeh 1997 {published data only}
* Yeh TF, Lin YJ, Hsieh WS et al. Early postnatal dexamethasone therapy for the prevention of chronic lung disease in preterm infants with respiratory distress syndrome: a multicenter clinical trial. Pediatrics 1997;100:URL: http://www.pediatrics.org/cgi/content/full/100/4/e3.
Yeh TF, Lin IJ, Hsieh WS, et al. Prevention of chronic lung disease (CLD) in premature RDS infants with early and prolonged dexamethasone (D) therapy--A multicenter double-blind controlled study. Pediatr Res 1994;35:262A.
Peng CT, Lin HC, Lin YJ et al. Early dexamethasone therapy and blood cell count in preterm infants. Pediatrics 1999;104:476-481.
Yeh TF, Lin YJ, Huang CC et al. Early dexamethasone therapy in preterm infants: a followup study. Pediatrics 1998;101:URL:http://www.pediatrics.org/cgi/content/full/101/5/e7.
Lin YJ, Yeh TF, Lin HC, Wu JM, Lin CH, Yu CY. Effects of early postnatal dexamethasone therapy on calcium homeostasis and bone growth in preterm infants with respiratory distress syndrome. Acta Paediatrica 1998;87:1061-1065.
Gaissmaier RE, Pohlandt F. Single-dose dexamethasone treatment of hypotension in preterm infants. J Pediatr 1999;134:701-705.
Tsukahara 1999 {published data only}
Tsukahara H, Watanabe Y, Yasutomi M, Kobata R, Tamura S, Kimura K, Hiraoka M, Mayumi M.. Early (4-7 days of age) dexamethasone therapy for prevention of chronic lung disease in preterm infants. Biol Neonate 1999;76:283-290.
Yaseen H, Okash I, Hanif M et al. Early dexamethasone treatment in preterm infants treated with surfactant: a double blind controlled trial. J Trop Pediatr 1999;45:304-306.
Doyle L, Davis P, Morley C. Postnatal dexamethasone in tiny babies: does it do more good than harm? A multi-centred, placebo-controlled, randomised clinical trial. Funded by NHMRC, Australia. Ongoing study.
* indicates the primary reference for the study
Anonymous. Dexamethasone for neonatal chronic lung disease. Lancet 1991;338:982-983.
Arias-Camison JM, Lau J, Cole CH, Frantz ID. Meta-analysis of dexamethasone therapy started in the first 15 days of life for prevention of chronic lung disease in premature infants. Pediatr Pulmonol 1999;28:167-174.
Baud O, Foix-L'Helias L, Kaminski M et al. Antental glucocortocoid treatment and cystic periventricular leukomalacia in very preterm infants. New Engl J Med 1999;341:1190-1196.
Bhuta T, Ohlsson A. Systematic review and meta-analysis of early postnatal dexamethasone for prevention of chronic lung disease. Arch Dis Child 1998;79:F26-F33.
Collaborative Dexamethasone Trial Group. Dexamethasone therapy in neonatal chronic lung disease: an international placebo-controlled trial. Pediatrics 1991;88:421-427.
Doyle LW, Davis PG. Postnatal corticosteroids in preterm infants: systematic review of effects on mortality and motor function. J Paediatr Child Health 2000;36:101-7.
Egberts J, Brand R, Walti H, Bevilacqua G, Breart G, Gardini F. Mortality, severe respiratory distress syndrome and chronic lung disease of the newborn are reduced more after prophylactic than after therapeutic administration of the surfactant Curosurf. Pediatrics 1997;100(1):URL: http:// www.pediatrics.org/egi/content/full/100/1/e4.
Gibson AT, Pearse RG, Wales JKH. Growth retardation after dexamethasone administration: assessment by knemonetry. Arch Dis Child 1993;69:505-509.
Gramsbergen A, Mulder EJH. The influence of betamethasone and dexamethasone on motor development in young rats. Pediatr Res 1998; 44;105-110.
Groneck P, Speer CP. Inflammatory mediators and bronchopulmonary dysplasia. Arch Dis Child 1995;73:F1-F3.
Halliday HL. A review of postnatal corticosteroids for treatment and prevention of chronic lung disease in the preterm infant. Prenatal Neonatal Medicine 1997;2:1-12.
Halliday HL. Clinical trials of postnatal corticosteroids: Inhaled and systemic. Biol Neonat 1999;76:29-40.
Halliday HL. Clinical trials of postnatal corticosteroids: inhaled and systemic. Biol Neonate 1999;76(Suppl 1):29-40.
Mammel MC, Green TP, Johnson DE, Thompson TR. Controlled trial of dexamethasone therapy in infants with bronchopulmonary dysplasia. Lancet 1983;1:1356-1358.
Ng PC. The effectiveness and side effects of dexamethasone in preterm infants with bronchopulmonry dysplasia. Arch Dis Child 1993;68:330-336.
Kothadia JM, O'Shea TM, Roberts D, Auringer ST, Weaver RG, Dillard RG. Randomized placebo-controlled trial of a 42-day tapering course of dexamethasone to reduce the duration of ventilator dependency in very low birthweight infants. Pediatrics 1999;104:22-27.
Papile L-A, Stoll B, Donovan E et al. Dexamethasone therapy in infants at risk for chronic lung disease (CLD): a multicenter, randomized, double-masked trial. Pediatr Res 1996;39:236A.
Ryan SW, Nycyk J, Shaw BNJ. Prediction of chronic neonatal lung disease on day 4 of life. Eur J Pediatr 1996;155:668-671.
Shah V, Ohlsson A, Halliday H, Dunn MS. Early administration of inhaled corticosteroids for preventing chronic lung disease in ventilated very low birth weight preterm neonates. In: The Cochrane Library, Issue 1, 2000. Oxford: Update Software.
Stanley FJ. Using cerebral palsy data in the evaluation of neonatal intensive care: a warning. Dev Med Child Neurol 1982;24:93-4.
Tarnow-Mordi W, Mitra A. Postnatal dexamethasone in preterm infants is potentially life saving, but follow up studies are urgently needed. BMJ 1999;319:1385-1386.
Tschanz SA, Damke BM, Burri PH. Influence of postnatally administered glucocorticoids on rat lung growth. Biol Neonate 1995;68:229-245.
van Goudoever JB, Wattimena JDL, Carnielli VP et al. Effect of dexamethasone on protein metabolism in infants with bronchopulmary dysplasia. J Pediatr 1994;124:112-118.
Watterburg KL, Scott SM. Evidence of early adrenal insufficiency in babies who develop bronchopulmonary dysplasia. Pediatrics 1995;95:120-125.
Weichsel ME. The therapeutic use of glucocorticoid hormones in the perinatal period: potential neurologic hazards. Ann Neurol 1977;2:364-366.
Werner JC, Sicard RE, Hansen TWR et al. Hypertrophic cardiomyopathy associated with dexamethasone therapy for bronchopulmonary dysplasia. J Pediatr 1992;120:286-291.
Halliday HL, Ehrenkranz RA. Early postnatal (<96 hours) corticosteroids for preventing chronic lung disease in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 2, 2000. Oxford: Update Software.
Halliday HL, Ehrenkranz RA. Early postnatal (<96 hours) corticosteroids for preventing chronic lung disease in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 1, 2001. Oxford: Update Software.
Halliday HL, Patterson CC, Halahakoon CW. A multicenter, randomized open study of early corticosteroid treatment (OSECT) in preterm infants with respiratory illness: comparison of early and late treatment and of dexamethasone and inhaled budesonide. Pediatrics 2001;107:232-40.
02 Chronic lung disease (CLD)/bronchopulmonary dysplasia (BPD)
02.01 CLD (28 days)
02.02 CLD (36 weeks)
02.03 CLD at 36 weeks in survivors
02.04 Late rescue with corticosteroids
02.05 Survivors who had late rescue with
corticosteroids
02.06 Survivors discharged home on oxygen
03 Death or CLD
03.01 Death or CLD at 28 days
03.02 Death or CLD at 36 weeks
04 Failure to extubate
04.01 Failure to extubate by 3rd day
04.02 Failure to extubate by 7th day
04.03 Failure to extubate by 14th day
04.04 Failure to extubate by 28th day
05 Complications during primary hospitalisation
05.01 Infection
05.02 Hyperglycaemia
05.03 Hypertension
05.04 Hypertrophic cardiomyopathy
05.05 Growth failure
05.06 Pulmonary air leak
05.07 PDA
05.08 Severe IVH
05.09 Severe IVH in infants examined
05.10 PVL
05.11 PVL in infants with cranial ultrasound
scans
05.12 PVL in survivors seen at follow-up
05.13 NEC
05.14 Gastro-intestinal bleeding
05.15 Intestinal perforation
05.16 Pulmonary haemorrhage
05.17 Received late steroids
05.18 Survivors who received late steroids
05.19 Any ROP
05.20 Severe ROP
05.21 Severe ROP in survivors
06 Long-term follow-up
06.01 Bayley MDI <-2SD
06.02 Bayley MDI <-2SD in tested survivors
06.03 Bayley PDI <-2SD
06.04 Bayley PDI <-2SD in tested survivors
06.05 Developmental delay (criteria not
specified)
06.06 Developmental delay (criteria not
specified) in tested survivors
06.07 Blindness
06.08 Blindness in survivors assessed
06.09 Deafness
06.10 Deafness in survivors assessed
06.11 Cerebral palsy
06.12 Death before follow-up in trials
assessing cerebral palsy
06.13 Death or cerebral palsy
06.14 Cerebral palsy in survivors assessed
06.15 Major neurosensory disability (variable
criteria - see individual studies)
06.16 Death before follow-up in trials
assessing major neurosensory disability (variable criteria)
06.17 Death or major neurosensory disability
(variable criteria)
06.18 Major neurosensory disability (variable
criteria) in survivors examined
06.19 Abnormal neurological exam (variable
criteria - see individual studies)
06.20 Death before follow-up in trials
assessing abnormal neurological exam (variable criteria)
06.21 Death or abnormal neurological exam
(variable criteria)
06.22 Abnormal neurological exam (variable
criteria) in tested survivors
06.23 Intellectual impairment (IQ <
70)
06.24 Intellectual impairment (IQ <
70) in survivors assessed
06.25 "Major neurosensory impairment"
- blindness or deafness
06.26 "Major neurosensory impairment"
- blindness or deafness - in survivors assessed
06.27 Behavior abnormalities
06.28 Behavior abnormalities in 3 yr old
survivors assessed
06.29 Abnormal EEG
06.30 Abnormal EEG in tested survivors
06.31 Re-hospitalisation in infancy
06.32 Re-hospitalisation in infancy in
survivors
Dr Richard A Ehrenkranz
Department of Pediatrics
Yale University
PO Box 208064
333 Cedar Street
New Haven
Connecticut USA
06520-8064
Telephone 1: 203 688 2318
Telephone 2: 203 688 2320
Facsimile: 203 688 5426
E-mail: richard.ehrenkranz@yale.edu
Secondary address:
333 Cedar Street
New Haven
Connecticut USA
06510
Telephone: 203 688 2320
Facsimile: 203 688 5426