Higher doses of selenium supplements may be able to reduce some complications for preterm babies, but more research is needed
Selenium is an essential trace element gained from nutrients. Babies are born with lower selenium concentrations in their blood than their mothers. In very preterm babies, low selenium is associated with an increased risk of complications. The review of trials of selenium supplementation for preterm babies found that it reduces sepsis (blood infection). It has not been shown to reduce other complications or increase survival. No adverse effects were reported. Higher than usual levels of selenium supplementation may be beneficial, but more research is needed as most of the evidence comes from a country where selenium levels were unusually low.
Selenium levels in the soil vary considerably in different geographical locations with blood selenium concentrations in both animal and human populations reflecting these variations. Plasma selenium concentrations in newborn infants in all regions of the world are lower than those of their mothers (Litov 1991) and, in breast fed infants, then rise after birth. Preterm infants are born with slightly lower selenium and glutathione peroxidase concentrations than term infants, have low hepatic stores of selenium and, particularly if fed parenterally with solutions lacking selenium, these concentrations decline further in the first months of life (Lokitch 1989; Sluis 1992). In some preterm infants selenium concentrations may fall as low as 0.13 micromol/L (10 micrograms/L) and are amongst the lowest recorded in humans.
The consequences of low selenium concentrations are not fully known. A range of selenium deficiency diseases have been described in animals and in some selenium deficient geographical areas, such as New Zealand, selenium supplements are essential for maintaining animal health. During the late 1970s reports from endemically selenium deficient areas of China described two human diseases associated with severe nutritional selenium deficiency. However, both Keshan disease, a juvenile cardiomyopathy, and Kaschin-Beck disease, a chondrodystrophy, seem to require other causative co-factors in addition to selenium deficiency (Litov 1991; Rayman 2000). Outside of China, selenium deficiency diseases have been rarely recognised and then only following exceptional circumstances such as prolonged parenteral nutrition or severe malnutrition when selenium concentrations fall to <0.20 micromol/L (16 micrograms/L). Clinical features have included muscle pain and tenderness, macrocytosis and pigmentary changes in hair and nails, and fatal cardiomyopathy (Litov 1991). The only reported adverse effect of low selenium levels in preterm infants has been increased erythrocyte fragility, which was accentuated by a diet high in polyunsaturated fatty acids and by iron supplements (Gross 1976).
In experimental animals, selenium deficiency has been associated with increased susceptibility to oxidative lung injury (Hawker 1993; Kim 1991). Sick very preterm infants are exposed to many possible sources of oxygen radical products, including high concentrations of inspired oxygen, frequent alterations of blood flow to major organs, and inflammation with accumulation of neutrophils and macrophages. Low blood selenium concentrations in preterm infants have therefore been suggested as a potential risk factor for chronic neonatal lung disease (Amin 1980; Lokitch 1989) and retinopathy of prematurity (DeVoe 1988; Kretzer 1988). Darlow 1995 in a study from New Zealand, which has low soil and population selenium concentrations, reported that low selenium concentrations at 28 days were associated with an increased risk of adverse respiratory outcome in very low birthweight infants. However, uncertainty exists as to whether selenium supplementation in preterm infants will prevent such morbidity.
Secondary Questions:
1. Does the route of supplementation (enteral or parenteral) affect outcome?
2. Does the dose of selenium supplementation affect outcome?
3. Does the gestation or birthweight of the infant affect outcome?
4. Does selenium supplementation lead to higher blood or plasma selenium
concentrations at or beyond 28 days of age?
Secondary outcomes measures: plasma or blood selenium and/or glutathione peroxidase concentrations at or beyond 28 days of age.
Side effects: skin eruptions, diarrhoea or other pre-defined clinical problems.
Data were be collected on:
Analysis
Separate analyses were conducted for each of the outcomes: death, neonatal
chronic lung disease, retinopathy of prematurity (any and stage 3 or 4) and
one or more proven episodes of sepsis. All analyses were conducted on an intention
to treat basis. The data were analysed using the standard method of the neonatal
review group using a fixed effect model, with use of relative risk, risk
reduction, number needed to treat and their 95% confidence intervals.
Participants
The three included studies reported outcomes on 297 infants receiving selenium
supplements and 290 control infants. One study (Darlow
2000) was much the largest and included 85% of all infants. This study
was a multicentre study involving 8 New Zealand neonatal units and included
infants with birthweight <1500g admitted to a participating unit by 72
hours of age and without major abnormalities. Five hundred and thirty-four
infants were randomised but five infants were withdrawn from the study, three
by parents and two by the neonatal team caring for the infants and no data
are available for these infants. Daniels 1996
included infants with birthweight <2000g, who were expected to have parenteral
nutrition for more than 5 days and no major congenital anomalies, liver or
renal disease. Forty-four infants were enrolled but six excluded, including
two who died (day 3 and day 11), three who received parenteral nutrition for
less than 6 days and one because of protocol violations. Data, including group
assignment, are not available for these infants. in addition, two further
infants died before hospital discharge and again group assignment for these
infants is not available. The study by Huston 1991
included infants with birthweight <1000g with no congenital, metabolic
or chronic white blood cell disease.
Interventions
The study by Daniels 1996 gave 3 micrograms/Kg/d
selenious acid in parenteral nutrition, and received for a mean 18 days, in
the treatment group versus nothing in controls. The study by Darlow 2000 gave 7 micrograms/Kg/d of sodium selenate
added to parenteral nutrition in the treatment group versus nothing in controls,
and 5 micrograms/Kg/d of sodium selenite in the treatment group or an equivalent
volume of sterile water for control infants, when fed orally until 28 days
of age. The study by Huston 1991 gave 1.5 micrograms/Kg/d
of selenious acid added to parenteral nutrition, and received for a mean 38
days, in the treatment group versus nothing in controls.
Outcome measures
Daniels 1996 reported CLD (an oxygen requirement
plus chest Xray changes) at 28 days, and one or more episodes of sepsis (defined
as microbiologically confirmed or requiring antibiotics for at least five
days). Darlow 2000 reported deaths pre-hospital
discharge, CLD (an oxygen requirement) at 28 days and at 36 weeks post-menstrual
age, any ROP in infants who were examined (ROP screening in New Zealand being
routinely carried out in infants <31 weeks gestation or <1250g birthweight),
and one or more episodes of sepsis (defined as clinical sepsis and a positive
culture from either blood or cerebrospinal fluid) after the first week of
life. Huston 1991 reported CLD at a mean 35 weeks
post-menstrual age, any ROP, and one or more episodes of sepsis (not defined
further).
Death pre-hospital discharge, Table 01.01
The studies by Darlow 2000 and Huston 1991 reported deaths pre-hospital discharge
with no significant differences between selenium supplementation and control
groups.
Oxygen use at 28 days in survivors, Table 01.02
The studies by Daniels 1996 and Darlow 2000 reported oxygen use at 28 days in survivors
with neither showing a significant difference between groups. The pooled
data also showed no significant difference [summary RR 0.99 (0.82, 1.18);
RD -0.01 (-0.09, 0.08)].
Death or oxygen use at 28 days, Table 01.03
Only the study by Darlow 2000 reported death
or oxygen use at 28 days with no significant difference between selenium supplementation
and control groups.
Oxygen use at 36 weeks PMA in survivors, Table 01.04
The studies by Darlow 2000 and Huston 1991 reported oxygen use at 36 weeks post-menstrual
age in surviving infants. Whilst there was no significant difference between
groups in the study by Darlow 2000, the study
by Huston 1991 did show a reduction in oxygen
use associated with selenium supplementation of borderline statistical significance
[ RR 0.33 (0.09, 1.27); RD -0.40 (-0.79, -0.01)]. The pooled data showed no
significant difference between groups [summary RR 1.02 (0.75, 1.39); RD 0.01
(-0.07, 0.08)].
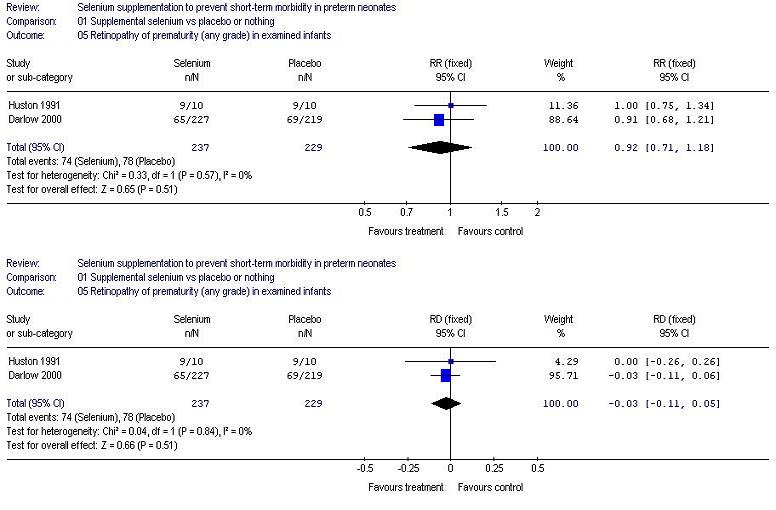
Retinopathy of prematurity (any grade) in examined infants, Table 01.05
The studies by Darlow 2000 and Huston 1991 reported on retinopathy of prematurity
of any grade, with neither showing a significant difference between groups.
The pooled data also showed no significant difference [summary RR 0.92 (0.71,
1.18); RD -0.03 (-0.11, 0.05)].
One or more episodes of sepsis, Table 01.06
All three studies reported on one or more episodes of sepsis and in Daniels 1996 and Darlow
2000 there was a significant reduction associated with selenium supplementation.
The pooled data show a significant reduction in sepsis associated with selenium
supplementation [summary RR 0.73 (0.57, 0.93); RD -0.10 (-0.17, -0.02); NNT
10 (5.9, 50)], with no significant heterogeneity.
Side effects
Only the study by Darlow 2000 reported on side
effects of selenium supplementation (skin rashes, diarrhoea or garlic odour
on breath), and noted that none were recorded.
Secondary outcomes
Blood or plasma selenium concentrations at or beyond 28 days of age.
Data on selenium concentrations have not been reported in a similar manner
across the studies and do not allow a meta-analysis to be performed. The study
by Huston 1991, which used the lowest dose of
selenium supplementation added to parenteral nutrition (1.5 micrograms/Kg/d),
found supplemented infants had significantly higher serum concentrations when
oral feeds were commenced (mean day 14-15) than control infants, although
these concentrations were below pre-randomisation concentrations. The study
by Daniels 1996 used a dose of 3 micrograms/Kg/d
added to parenteral nutrition and found plasma selenium concentrations fell
compared with pre-randomisation concentrations by three weeks of age in control
infants, whilst this decline was prevented by supplementation. By six weeks
of age there was no significant difference between the groups with selenium
concentrations in both being similar to pre-randomisation concentrations.
The study by Darlow 2000 supplemented parenteral
nutrition with 7 micrograms/Kg/d and enteral feeding with 5 micrograms/Kg/d
of selenium. Supplemented infants had plasma selenium concentrations significantly
higher (nearly two-fold) at 28 days and 36 weeks post-menstrual age than pre-randomisation
concentrations and these were similar to concentrations found in healthy
breast-fed term infants in this population. By contrast, selenium concentrations
in control infants showed a non-significant fall at these times compared
with pre-randomisation concentrations. Plasma glutathione peroxidase concentrations
were also significantly higher at 28 days and 36 weeks post-menstrual age
compared with control infants and with pre-randomisation concentrations.
The study by Darlow 2000 included 243 infants with birthweight <1000g and noted that confining analysis to this subgroup of infants did not reveal significant differences between the groups with respect to primary or secondary outcomes, however the data have not been reported.
The study by Darlow 2000 reported that lower plasma selenium concentrations before randomisation were associated with an increased risk of adverse respiratory outcome at 28 days and a trend to increased risk of adverse outcome at 36 weeks post-menstrual age, after controlling for gestational age, antenatal steroids, CRIB score and hospital. There was a similar association between maternal selenium concentrations at enrolment and neonatal outcome. The relationship between pre-randomisation infant selenium concentrations and total days in oxygen was non-linear with a threshold of between 0.2 and 0.4 micromols/L below which, in this population, selenium concentrations had an effect on days of oxygen requirement. These findings suggest that if oxidative damage contributes to respiratory morbidity in preterm infants, and selenium has a role in preventing or ameliorating such damage, that it may be critical to achieve improved selenium status earlier than was the case in the studies included in this review. Low selenium concentrations at birth reflect low body stores (Bayliss 1985) and also correlate with maternal concentrations. At least in populations with low selenium status, the role of maternal selenium supplementation from perhaps 20 weeks' gestation could be the subject of further study, although given that very preterm infants constitute only around 1% of births, large numbers of pregnant women (at least 5,000) would have to be recruited.
Two of the studies in this review come from geographical areas recognised as having low soil and population concentrations of selenium. There are good theoretical reasons to expect that, if selenium supplementation does result in decreased morbidity, this would be more readily apparent in studies from populations with low selenium concentrations. Nevertheless, the fact that the one large study is from such a population and that no large trials have been carried out in populations with higher concentrations, does mean that the results may not be generalisable.
The mean pre-randomisation plasma selenium concentrations in the study by Daniels 1996 (South Australia) were 0.34 and 0.36 micromols/L, in the study and control groups respectively, and in the study by Darlow 2000 (New Zealand) were 0.33 micromols/L in both groups. In contrast the mean pre-randomisation serum selenium concentrations in the study by Huston 1991 (Portland, Oregan) were 0.91 and 0.81 micromols/L in the study and control groups. Preterm infants generally have lower selenium concentrations than term infants in the same population, and in healthy term breast-fed infants concentrations then rise after birth. North American recommendations are for preterm infants to be supplemented with 2 micrograms/Kg/d selenium whilst receiving parenteral nutrition (Reifen 1993). The data from Huston 1991 show that a slightly lower dose (1.5 micrograms/Kg/d) resulted in serum concentrations still below starting concentrations after two weeks. In another study from North America, Ormsby 1998, reported that a dose of 4 micrograms/Kg/d added to parenteral nutrition for an average of more than three weeks did not maintain day one plasma selenium concentrations in preterm infants. Taken together, the studies of Daniels 1996 and Darlow 2000 suggest that 3 micrograms/Kg/d selenium supplementation in preterm infants may maintain cord concentrations but supplementation of 5-7 micrograms/Kg/d may be required to raise concentrations above those in cord blood to close to those found in healthy breast-fed term infants. Additional factors that may influence selenium concentrations in preterm infants include the form of selenium supplementation, route of administration and interactions with other nutrients, and the selenium content of enteral feeds.
Two studies, Daniels 1996 and Darlow 2000, as well as the pooled data showed a significant reduction in one or more episodes of sepsis associated with selenium supplementation, with the number needed to treat to prevent sepsis in one infant being 10. Selenium is known to have a role in immunocompetence (Rayman 2000). Neutrophils and macrophages from selenium deficient animals have low glutathione peroxidase concentrations, which may affect their antimicrobial properties, and animal studies have also shown that immunoglobulin antibody responses may be enhanced by selenium supplementation (Turner 1991). The relationship between selenium status and infections in preterm infants in different populations and the role of selenium supplementation is an important area for further research.
Limitations of this review.
Two included studies did not report outcome for all participants. Daniels 1996 did not report any data, including
group assignment, for six infants, two of whom died. In the study by Darlow 2000 examination for retinopathy of prematurity
followed national guidelines (<31 weeks gestation or <1250g birthweight
as a routine) and hence not all surviving infants were examined. Darlow 2000 also defined sepsis as episodes after
the first week of life.
Two of the studies in this review, one of which accounts for 85% of participants, come from geographical areas recognised as having low soil and population concentrations of selenium. There are good theoretical reasons to expect that, if selenium supplementation does result in decreased morbidity, this would be more readily apparent in studies from populations with low selenium concentrations. Nevertheless, the fact that the one large study is from such a population and that no large trials have been carried out in populations with higher concentrations, does mean that the results may not be generalisable.
Further studies are warranted on the relationship between selenium status and infections in preterm infants.
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Daniels 1996 | Single centre randomised controlled trial Blinding of randomisation: yes Blinding of intervention: yes Complete follow-up: no Blinding of outcome measures: yes |
N=38 [44 infants randomised but data only reported for 38 - see
text] Birthweight less than 2000g; stratified as less than 1000g or 1000-1999g Expected to have TPN for more than 5 days No major congenital anomalies, liver or renal disease |
19 infants randomised to treatment and 19 to control groups 3 microg/Kg/d of selenious acid added to TPN for as long as this required (mean 18-19 days) vs no supplementation |
CLD (defined as oxygen requirement at 28 days plus chest Xray
changes One or more episodes of sepsis (defined as microbiologically confirmed or antibiotics for at least 5 days) Changes in mean plasma and erythrocyte selenium or glutathione peroxidase activity at 3 and 6 weeks |
Total selenium intake from all sources monitored | A |
| Darlow 2000 | Multicentre randomised controlled trial Blinding of randomisation: yes Blinding of intervention: yes Complete follow-up: yes Blinding of outcome measurement: yes |
N=529 [534 infants randomised but data only reported for 529 -
see text] Birthweight less than 1500g, stratified by hospital and less than 1000g or 1000-1499g No major anomalies |
268 infants randomised to treatment and 261 to control groups 7 microg/Kg/d of sodium selenate added to TPN vs no supplementation when intravenously fed and 5 microg/Kg/d sodium selenite vs equal volume (0.5 ml/Kg) sterile water when orally fed until 36 weeks PMA or discharge home |
Death before hospital discharge CLD defined as oxygen requirement at 28 days of age and at 36 weeks PMA ROP of any stage in examined infants One or more episodes of sepsis (defined as clinical sepsis and positive culture from blood or CSF) after 1 week of age Plasma selenium and glutathione peroxidase concentrations at 28 days and 36 weeks PMA |
Infants changed from parenteral to oral supplements when tolerating 3 ml/hr | A |
| Huston 1991 | Single centre randomised controlled trial Blinding of randomisation: yes Blinding of intervention: yes Complete follow-up: yes Blinding of outcome measurement: yes |
N=20 Birthweight less than 1000g No congenital metabolic or white blood cell diseases |
10 infants randomised to treatment and 10 to control groups 1.5 microg?Kg/d of selenious acid added to TPN for as long as this required (mean 42 days) vs no supplementation |
Death in hospital CLD defined as oxygen requirement at 60 days (equivalent to 35.1 weeks PMA from mean gestation of 26.5 weeks) ROP of any stage and grades III and IV in examined infants One or more episodes of sepsis (not defined further) Serum selenium and WBC glutathione peroxidase concentrations at time enteral feeding commenced (mean 14-15 days) and at time fully enterally fed (mean 42 days) |
Also assessed serum levels of copper and zinc and WBC superoxide dismutase activity | A |
| Study | Reason for exclusion |
| Bogye 1998a | No clinical outcome data Serum selenium and glutathione concentrations at 14 days only The Biofactors report is labelled an "Extended Abstract" and repeats data in primary report |
| Bogye 1998b | No clinical outcome data Serum selenium and glutathione concentrations at 14 days only Report contains similar data to (includes 36 compared with 28 infants), and may overlap with, Bogye 1998a. The author is being contacted for clarification. |
| Ehrenkranz 1991 | No clinical outcome data Main aim of study was to assess enteral selenium absorption and retention using a stable isotope |
| Rudolph 1981 | Not a trial of selenium supplementation |
| Smith 1991 | Oral supplementation begun at mean 15-26 days. Data not reported for 25 of 71 enrolled infants. No clinical outcome data. |
| Tyrala 1996 | Only infants with no evidence of disease process included. Study infants not all feeding study formula exclusively until 4 weeks of age. No clinical outcomes |
* Daniels L, Gibson R, Simmer K. Randomised clinical trial of parenteral selenium supplementation in preterm infants. Arch Dis Child 1996;74:F158-F164.
Daniels LA, Gibson RA, Simmer K. Selenium (SE) supplementation of preterm infants. J Paediatr Child Health 1995;31:A22.
Darlow 2000 {published data only}
Darlow BA, Inder TE, Sluis KB, Buss H, Graham P, Mogridge N, Winterbourn CC, The New Zealand Neonatal Study Group. Randomised controlled trial of selenium supplementation in New Zealand VLBW infants. Pediatr Res 1998;43:258A.
* Darlow BA, Winterbourn CC, Inder TE, Graham PJ, Harding JE, Weston PJ, Austin NC, Elder DE, Mogridge N, Buss IH, Sluis KB, The New Zealand Neonatal Study Group. The effect of selenium supplementation on outcome in very low birth weight infants: A randomized controlled trial. J Pediatr 2000;136:473-80.
Huston 1991 {published data only}
Huston RK, Jelen BJ, Vidgoff J. Selenium supplementation in low-birthweight premature infants: Relationship to trace metals and antioxidant enzymes. J Parent Ent Nutr 1991;15:556-59.
* Bogye G, Alfthan G, Machay T. Bioavailability of enteral yeast-selenium in preterm infants. Biol Trace Elem Res 1998;65:143-51.
Bogye G, Alfthan G, Machay T. Randomized clinical trial of enteral yeast-selenium supplementation in preterm infants. Biofactors 1998;8:139-42.
Bogye 1998b {published data only}
Bogye G, Alfthan G, Machay T, Zubovics L. Enteral yeast-selenium supplementation in preterm infants. Arch Dis Child 1998;78:F225-26.
Ehrenkranz 1991 {published data only}
Ehrenkranz RA, Gettner PA, Nelli CM, Sherwonit EA, Williams JE, Ting BT, Janghorbani M. Selenium absorption and retention by very-low-birth-weight infants: Studies with the extrinsic stable isotope tag 74Se. J Pediatr Gastroenterol Nutr 1991;13:125-33.
Rudolph 1981 {published data only}
Rudolph N, Preis O, Bitzos EI, Reale MM, Wong SL. Hematological and selenium status of low-birth-weight infants fed formulas with and without iron. J Pediatr 1981;99:57-62.
Smith 1991 {published data only}
Smith AM, Chan GM, Moyer-Milieur LJ, Johnson CE, Gardner BR. Selenium status of preterm infants fed human milk, preterm formula, or selenium-supplemented preterm formula. J Pediatr 1991;119:429-433.
Tyrala 1996 {published data only}
Tyrala EE, Borschel MW, Jacobs JR. Selenate fortification of infant formulas improves the selenium status of preterm infants. Am J Clin Nutr 1996;64:860-65.
* indicates the primary reference for the study
Amin S, Chen SY, Collipp PJ, Castro-Magan M, Maddaiah JVT, Klein SW. Selenium in premature infants. Nutr Metab 1980;24:331-40.
Arthur JR, Beckett GJ. New metabolic roles for selenium. Proc Nutr Soc 1994;53:615-24.
Bayliss PA, Buchanan BE, Hancock RGV, Zlotkin SH. Tissue selenium accretion in premature and full-term infants and children. Biol Trace Elem Res 1985;7:55-61.
Darlow BA, Inder TE, Graham PJ, Sluis KB, Malpas TJ, Taylor BJ, Winterbourn CC. The relationship of selenium status to respiratory outcome in the very low birth weight infant. Pediatrics 1995;96:314-9.
DeVoe WM. Prevention of retinopathy of prematurity. Semin Perinatol 1988;12:373-80.
Gross S. Hemolytic anaemia in premature infants: relationship to vitamin E, glutathione peroxidase and erythrocyte lipids. Semin Hematol 1976;13:187-99.
Hawker FH, Ward HE, Stewart PM, Wynne LA, Snitch PJ. Selenium deficiency augments the pulmonary toxic effects of oxygen exposure in the rat. Eur Respir J 1993;6:1317-23.
Kim HY, Picciano MF, Wallig MA, Milner JA. The role of selenium nutrition in the development of neonatal rat lung. Pediatr Res 1991;29:440-45.
Kretzer FL, Hittner HM. Retinopathy of prematurity: clinical implications of retinal devlopment. Arch Dis Child 1988;63:1151-67.
Litov RE, Combs GF. Selenium in pediatric nutrition. Pediatrics 1991;87:339-51.
Lockitch G, Jacobson B, Quigley G, Dison P, Pendray M. Selenium deficiency in low birth weight neonates: an unrecognized problem. J Pediatr 1989;114:865-70.
Ormsby AR, Tyrala EE. Se sufficiency is not achieved with currently recommended dosages of IV Se intake. Ped Res 1998;43:268A.
Rayman MP. The importance of selenium to human health. Lancet 2000;356:233-41.
Reifen RM, Zlotkin S. Microminerals. In: Tsang RC, Lucas A, Uauy R, Zlotkin S, editor(s). Nutritional needs of the preterm infant: scientific basis and practical guidelines. Baltimore: Williams and Wilkins, 1993:195-207.
Sluis KB, Darlow BA, George PM, Mogridge N, Dolamore BA, Winterbourn CC. Selenium and glutathione peroxidase levels in premature infants in a low selenium community (Christchurch, New Zealand). Pediatr Res 1992;32:189-94.
Turner RJ, Finch JM. Selenium and the immune response. Proc Nutr Soc 1991;50:275-85.
01.01 Death pre-hospital discharge
01.02 Oxygen use at 28 days in survivors
01.03 Death or oxygen use at 28 days
01.04 Oxygen use at 36 weeks PMA in survivors
01.05 Retinopathy of prematurity (any grade) in examined infants
01.06 One or more episodes of sepsis
| Comparison or outcome | Studies | Participants | Statistical method | Effect size |
|---|---|---|---|---|
| 01 Supplemental selenium vs placebo or nothing | ||||
| 01 Death pre-hospital discharge | 1 | 549 | RR (fixed), 95% CI | 0.92 [0.48, 1.75] |
| 02 Oxygen use at 28 days in survivors | 2 | 548 | RR (fixed), 95% CI | 0.99 [0.82, 1.18] |
| 03 Death or oxygen use at 28 days | 1 | 529 | RR (fixed), 95% CI | 0.97 [0.80, 1.16] |
| 04 Oxygen use at 36 weeks PMA in survivors | 2 | 521 | RR (fixed), 95% CI | 1.02 [0.75, 1.39] |
| 05 Retinopathy of prematurity (any grade) in examined infants | 2 | 466 | RR (fixed), 95% CI | 0.92 [0.71, 1.18] |
| 06 One or more episodes of sepsis | 3 | 583 | RR (fixed), 95% CI | 0.73 [0.57, 0.93] |
| This review is published as a Cochrane review in
The Cochrane Library 2003, Issue 4, 2003 (see www.CochraneLibrary.net for
information). Cochrane reviews are regularly updated as new evidence
emerges and in response to comments and criticisms, and The Cochrane Library
should be consulted for the most recent version of the Review. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}