Not enough evidence to show whether regional anaesthesia is better than general anaesthetic for a preterm baby having surgery for inguinal hernia
Babies born preterm (before 37 weeks) often have serious health problems and sometimes need surgery. Inguinal hernia (where the intestine protrudes through the abdominal wall) is the commonest condition where surgery is needed. General anaesthetics for surgery can disrupt breathing and cause other complications in preterm babies. Regional anaesthetics including spinal block (injection) might avoid complications. Whether this improves outcomes for preterm babies having surgery has been unclear. The review found that there is not enough evidence from trials to show whether or not spinal block improves outcomes for a preterm baby having surgery for inguinal hernia.
A large well designed randomised controlled trial is needed to determine if spinal anaesthesia reduces post-operative apnoea in ex-preterm infants not pretreated with sedatives. Adequate blinding, follow up and intention to treat analysis are required.
Of concern in the preterm group is the high incidence of apnoea with or without bradycardia following operations performed under general anaesthesia. Apnoea in preterm infants has been defined as a pause in breathing of greater than 20 seconds or one less than 20 seconds and associated with cyanosis, marked pallor, hypotonia or bradycardia (NIH 1987). It appears to be related to an immature respiratory musculature and central control mechanism, an unstable elastic rib cage, an upper airway that is prone to obstruction, a lower airway prone to collapse, hypothermia and anaemia (Henderson-Smart 1995).
Most postoperative studies show that approximately 20% to 30% of otherwise healthy former preterm infants having inguinal herniorrhaphy under general anaesthesia have one or more apnoeas in the postoperative period (Sims 1994) and this risk is inversely proportional to postmenstrual age (PMA, gestational age plus postnatal age) (Welborn 1990) . Other specific risk factors for apnoea include anaemia (hematocrit <30%), bronchopulmonary dysplasia and ongoing apnea at home (Cote 1995).
The risk period for apnoea, bradycardia or periodic breathing is from the intraoperative period through to many hours later. Episodes of apnoea may begin at any time in the first 12 hours after surgery. Apnoea can then continue until 48 hours, and even 72 hours after surgery (Sims 1994).
Anaesthetics produce dose-dependent and drug specific changes in the mechanics and central control of the respiratory centre. Inhaled anaesthetics produce a decrease in the muscle tone in the airways, chest wall and diaphragm and may further induce apnoea by augmenting central respiratory responsiveness to inhibitory afferents and reducing the responsiveness to ventilatory stimulants. Inhaled anaesthetics also alter the response to carbon dioxide and the pattern of breathing. Intravenous anaesthetics also alter respiratory function. Opioids produce a dose dependent depression of medullary respiratory centres, which leads to a decreased responsiveness to PaCO2 (Welborn 1997).
In view of the high incidence of postoperative apnoea in preterm infants undergoing anaesthesia, a number of investigators have postulated a safe operating period does not commence until a postmenstrual age of greater than 44 weeks, or even greater than 60 weeks. In addition to a suggested safe period of operation, awake regional anaesthesia has been suggested to reduce, but not abolish the incidence of post-operative apnoea, with an even lower incidence observed when no sedation is used (Frumiento 2000). Prophylactic caffeine has also been used to prevent postoperative apnea following general anaesthesia (Henderson-Smart 2002).
Prespecified subgroup analyses will include:
Gestational age (above and below about 32 weeks)
Birth weight (above and below about 1500 grams)
Postmenstrual age at time of surgery (less than or more than 50 weeks
PMA)
Presence of chronic lung disease (as defined by an oxygen requirement
at 36 weeks corrected gestational age)
Anaemia (hematocrit less than 30%)
The administration of prophylactic caffeine/theophylline to prevent
apnoea
The preoperative use of sedatives
Data were extracted independently by at least two reviewers. The data were checked and entered into the Cochrane Review Manager (RevMan) computer software by one reviewer. Any missing information or data inconsistencies were checked where necessary with the authors of the study.
Meta-analysis was carried out using the RevMan software using the fixed effects model and results were expressed as typical relative risk (RR), typical risk difference (RD) and number needed to treat (NNT) for categorical data, weighted mean difference for continuous data. 95% confidence intervals were used. We tested for heterogeneity of treatment effect to help decide when meta-analysis was appropriate. For effects where typical RD but not typical RR was statistically significant, we termed the result as of "borderline statistical significance" in this review.
Four trials qualified for inclusion in this review: Welborn 1990; Krane 1995; Somri 1998; Williams 2001. All studies were published as complete articles. Complete data from the investigators are awaited for one study (Krane 1995), however we have included the information available to date for this systematic review.
Details of each study are given in the table, Characteristics of Included Studies. Overall, the studies attempted to include ex-premature infants. The inclusion criteria, the intervention (type of anaesthetic agent) and outcomes varied between studies.
All studies compared single shot spinal versus general anaesthesia in premature infants (< 37 weeks) undergoing inguinal herniorrhaphy.
One study (Krane 1995) enrolled 18 infants less than 36 weeks gestation, who were less than 60 weeks corrected gestational age, with an ASA (American Society of Anesthesiologists) physical class of I or II, undergoing inguinal herniorrhaphy. The authors excluded significant chronic lung disease, known symptomatic congenital heart disease or symptomatic central nervous system disease. Preoperative respiratory function of the included infants was assessed by a 12 hour study of respiratory rate, haemoglobin oxygen saturation and ECG in the infant's home. On the day of surgery 10 infants received a single shot spinal anaesthetic with 0.6mg/kg tetracaine HCl made hyperbaric with an equal volume of 10% dextrose. When clinically indicated some infants received 50% N2O blown by their face. In the general anaesthesia group, eight infants received balanced anaesthesia, with halothane and muscle relaxation. At the end of the surgery the ilioinguinal nerve was infiltrated with 0.25% bupivacaine for pain relief. When necessary, at the conclusion of surgery, neuromuscular blockade was antagonised with neostigmine and atropine. One patient in the spinal anaesthetic group had a failed spinal anaesthetic and was then given a general anaesthetic. The outcome measures of postoperative apnoea (cessation of respiratory movement for more than 10 seconds), bradycardia and periodic breathing were reported to be equal in each group, but individual data were not supplied. Postoperative haemoglobin oxygen desaturation (a decrease of SpO2 to < 90% for 10 seconds or more), anaesthetic placement failure and anaesthetic agent failure were measured and reported for the two groups. Three infants required supplemental N2O, in addition to the spinal anaesthetic. One patient with a failed spinal anaesthetic was given a general anaesthetic. Three infants received additional N2O for failed spinal anaesthetic agent and one had a failure to place the spinal anaesthetic needle. Post-operative pain relief in both groups was managed with paracetamol and no opioids were administered.
The second study (Somri 1998) enrolled 40 infants < 37 weeks gestation or who were less than 60 weeks corrected gestational age and/or with one of the following: a history of neonatal respiratory distress syndrome, bronchopulmonary dysplasia documented by radiography or a history of preoperative apnoea. They did not exclude any infants on entry criteria but did exclude from analysis those infants where there was failure to achieve spinal needle placement. On the day of surgery, 20 infants received a spinal anaesthetic with isobaric bupivacaine 0.6-0.8mg/kg. A pacifier was used to soothe restless infants. In the general anaesthesia group 20 infants received thiopentone intravenous induction, 4-5mg/kg, followed by balanced anaesthesia of halothane 0.5-1.5% and muscle relaxation with atracurium, 0.5mg/kg. Neuromuscular blockade was reversed at the end of surgery with neostigmine and atropine. The outcome measures were postoperative apnoea (defined as a respiratory pause of 15 seconds or longer or <15 seconds with bradycardia (defined as a heart rate of <100 beats/minute), postoperative analgesia, postoperative respiratory support, average length of hospital stay, anaesthetic placement failure and multiple spinal placement attempts. Six infants in the spinal anaesthesia group became restless despite successful spinal blockade and supplementary anaesthesia was administered to restore adequate operating conditions: four patients received inhaled halothane and two received intravenous propofol. Failure to achieve lumbar puncture with the spinal needle is a placement failure, whereas successful placement but failure to achieve adequate anaesthesia is an agent failure. In the postoperative period only paracetamol was used for analgesia.
The third study (Welborn 1990) enrolled 36 infants less than 37 weeks gestation, who were less than 51 weeks corrected gestational age and who were healthy, with an ASA physical status I or II. The authors excluded infants who had either cardiac, neurological or metabolic disease and those who were receiving methylxanthines or caffeine. In the spinal anaesthesia group, during the early part of the study, nine infants received IM ketamine for sedation prior to performance of lumbar puncture. These results were presented separately. As the authors gained experience, because of the observed high incidence of side effects, the ketamine was stopped. The remaining 11 infants in the spinal group were comforted with sugar solution. In all patients the spinal anaesthesia was achieved by 1% tetracaine 0.4-0.6mg/kg with an equal volume of 10% dextrose. The 16 infants in the general anaesthesia group received a balanced anaesthetic with halothane and neuromuscular blockade. Neuromuscular blockade was reversed at the end of surgery with neostigmine and atropine. The outcomes measured were postoperative apnoea (defined as a respiratory pause of <15 seconds not associated with bradycardia), and prolonged apnoea defined as a respiratory pause of 15 seconds or longer or less than 15 seconds accompanied by bradycardia (defined as a heart rate less than 100 beats per minute for at least 5 seconds). Other outcomes measured included post-operative respiratory support, length of surgery and temperature on admission to the recovery room.
The fourth study (Williams 2001) enrolled 28 infants <36 weeks gestation, who were less than 46 weeks post conceptional age. The authors excluded infants with pre existing cardiac, neuromuscular or metabolic diseases. Pre-existing abnormal respiratory function with or without the need for supplemental oxygen therapy was noted. On the day of surgery 14 patients received a spinal anaesthetic consisting of 0.5% bupivacaine 1mg/kg. The 14 infants in the general anaesthesia group received a 2 MAC equivalent value for age of sevoflurane in 100% oxygen and muscle relaxation with atracurium. At the end of surgery, neuromuscular blockade was antagonised with neostigmine and glycopyrrolate. Both groups received a single injection of bupivacaine 0.25% 2mg/kg into the caudal epidural space for post-operative analgesia. The outcome measure was postoperative apnoea (a sustained respiratory pause of 15 seconds or longer, or less than 15 seconds if accompanied by an SPO2 less than 90% or bradycardia). Bradycardia was defined as a heart rate of less than 100 beats/minute for at least 5 seconds. Anaesthetic placement failure was also measured.
Overall, the studies included in this review were of inadequate quality. Due to the nature of the intervention contrast, it was not possible to blind the intervention in any of the studies. Specific methodological issues of individual trials are discussed below:
Krane 1995- Randomisation in this study was not described adequately. There was no mention of allocation concealment and there was no blinding of intervention but there was adequate blinding of the outcome, with the results being interpreted by a trained technician not aware of the treatment group assignment. There was complete follow up of all enrolled patients. The one patient with a failed spinal anaesthetic who was given a general anaesthetic was counted as a member of the general anaesthetic group. We have re-analysed this by intention to treat analysis with the patient re analysed in the spinal group. Unfortunately, despite contacting the author further clarification of this patient was unavailable
Somri 1998- Randomisation in this study was not described adequately. There was no mention of allocation concealment and there was no blinding either to intervention or outcome. There was complete follow up of all enrolled patients. Bias was introduced by omitting three infants in which lumbar puncture was unsuccessful and one infant was excluded because of hypothermia.
Welborn 1990- Randomisation in this study was not described adequately. There was no mention of allocation concealment and there was no blinding of intervention, but a pulmonologist unaware of treatment group assessed outcome. There was complete follow-up. Subgroup analysis was performed, with and without pre-anaesthetic ketamine sedation, in the spinal group, following initial concerns of pre-anaesthetic sedation with resultant post-operative apnoeas. Results were reported by the investigators in three groups, general anaesthesia, spinal plus ketamine, spinal without ketamine.
Williams 2001- Randomisation in this study was adequately described with the use of random number tables. There was no mention of allocation concealment and there was no blinding of intervention but the results were analysed by a blinded observer. There was complete follow up. Four patients were excluded following randomisation due to anaesthetic failure in the spinal anaesthesia group. These four infants were given a general anaesthetic but were excluded from further analysis by the authors.
PRIMARY OUTCOME MEASURES
Apnoea/bradycardia: Three studies reported on apnoea/bradycardia. In all four studies the definition of apnoea did not fulfil the NIH 1987 definition of a pause in breathing of greater than 20 seconds or one less than 20 seconds and associated with cyanosis, marked pallor, hypotonia or bradycardia. In studies by Somri 1998; Williams 2001; Welborn 1990, they used a definition of a pause in breathing of 15 seconds or less if associated with bradycardia, and the study by Krane 1995 used a definition of 10 seconds or less associated with bradycardia. Only the study by Somri 1998 showed a significant reduction in the rate of apnoea/bradycardia among infants who received a spinal anaesthetic, RR 0.12 (0.02, 0.89). The other two studies showed no significant difference between intervention groups. Meta-analysis showed no significant difference between the intervention groups, typical RR 0.69 (0.40, 1.21).
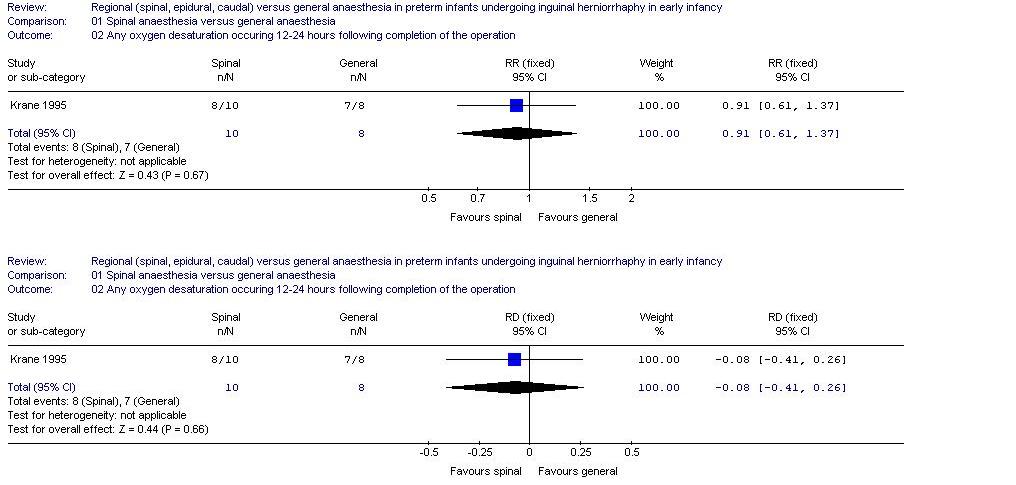
Any oxygen desaturation: Only one study, Krane 1995, reported on oxygen desaturation. This study showed no significant difference in the rate of oxygen desaturation between infants who received a spinal anaesthetic and those who received a general anaesthetic, RR 0.91 (0.61, 1.37).
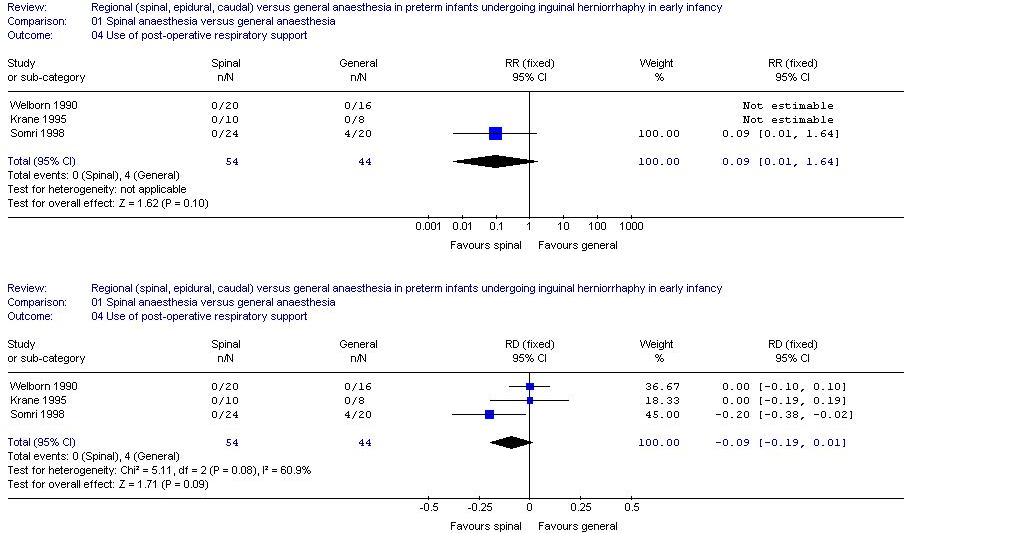
Post-operative respiratory support: Only three studies reported this outcome and in only one (Somri 1998) did any infant require respiratory support (>1 hour post reversal of general anaesthesia). In that study this was required by none of the infants who received spinal anaesthesia, but by four of the infants who received a general anaesthetic. In the meta-analysis this difference was of borderline statistical significance, typical RR 0.09 (0.01, 1.64), typical risk difference (RD) -0.09 (-0.19, -0.01). The number needed to treat with a spinal anaesthetic to prevent one additional infant requiring post-operative ventilatory support is 11.
Postoperative apnoea having excluded preoperative sedatives: Three studies reported postoperative apnoea in patients having no preoperative sedatives. Welborn 1990 ceased the usage of preoperative ketamine because of apnoea. Once ketamine was ceased the incidence of apnoea reduced dramatically. We have thus re analysed the results with and without the ketamine group. The effect on postoperative apnoea became significant once the group with preoperative ketamine was removed, typical RR 0.39 (0.19, 0.81).
SECONDARY OUTCOME MEASURES
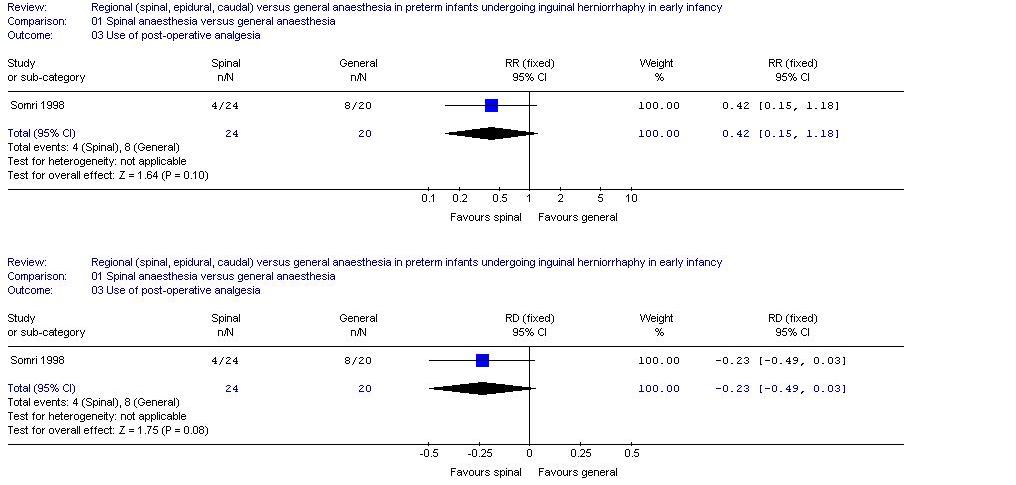
Postoperative analgesia: The only study to report this was Somri 1998 which showed no significant difference in the use of postoperative analgesia between infants who received a spinal anaesthetic and those who received a general anaesthetic, RR 0.42 (0.15, 1.18). In none of the studies were opioids or other respiratory depressants used for post-operative analgesia. All studies used paracetamol for pain relief.
Length of surgery: Only one study (Welborn 1990) reported effect on the length of surgery. This study reported no significant difference between the treatment groups; however, insufficient data were supplied to allow calculation in this systematic review.
Average length of hospital stay: Only one study reported the length of hospital stay (Somri 1998) and there was no significant difference between the treatment groups; however, insufficient data were supplied to allow calculation in this systematic review.
Temperature on admission to recovery: Only the study by Welborn 1990 reported temperature on admission to recovery. The mean temperature on admission to recovery, 36.5 degrees celsius, was the same between the two intervention groups.
Anaesthetic placement failure: Three studies reported on anaesthetic placement failure. In the studies by Somri 1998 and Williams 2001, infants who received a spinal anaesthetic were more likely to have an spinal needle placement failure but in neither study did this reach statistical significance. In the study by Krane 1995, no infant in either group had anaesthetic placement failure. Overall, there was an increase in the risk of having anaesthetic placement failure in the spinal group which was of borderline statistical significance, typical RR 7.38 (0.98, 55.52), typical RD 0.15 (0.03, 0.27). The number of spinal anaesthetics required to result in one spinal needle placement failure was seven.
Anaesthetic agent failure: Two studies, Krane 1995 and Somri 1998, assessed anaesthetic agent failure. Each study found a trend to higher incidence of failure in the spinal group. In the meta-analysis, infants who received a spinal anaesthetic were significantly more likely to have a failed anaesthetic agent, typical RR 9.13 (1.26, 66.27; typical RD 0.29 (0.12, 0.47). The number of spinal anaesthetics required to result in one anaesthetic agent failure was three.
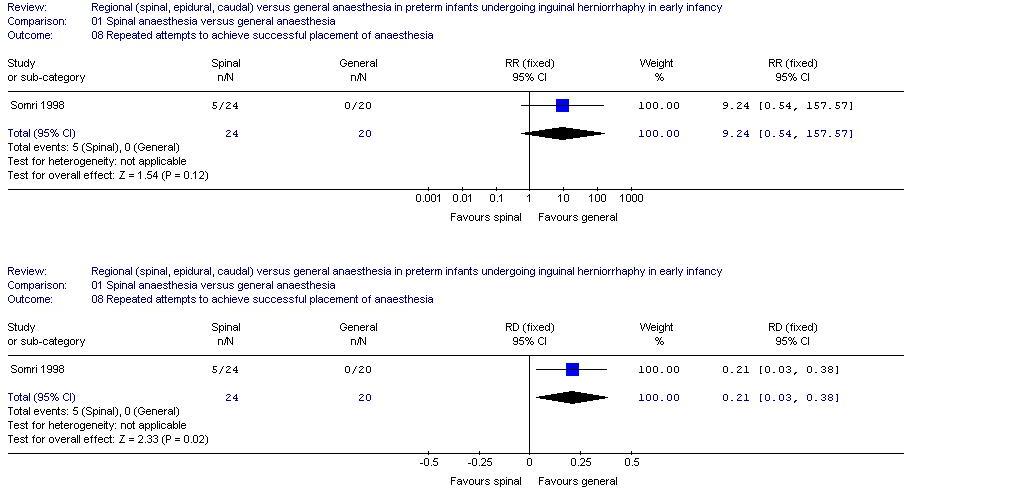
Repeated attempts to achieve successful anaesthesia: In the study by Somri 1998, infants undergoing a spinal anaesthetic were more likely to undergo multiple attempts to achieve accurate placement of the spinal needle. This effect was of borderline statistical significance, [RR 9.24 (0.54, 157.58), RD 0.21 (0.03, 0.39)].
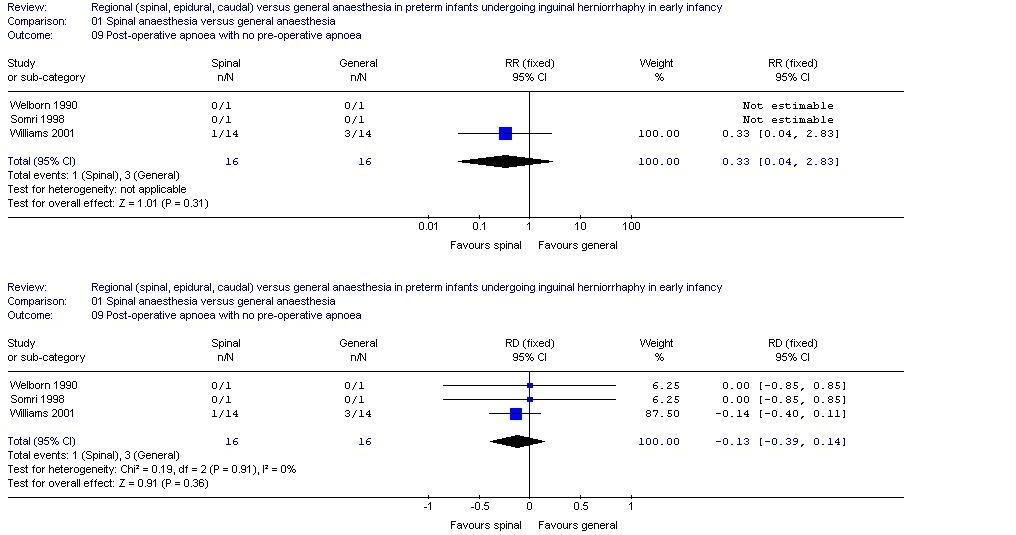
Postoperative apnoea with no pre-operative apnoea: In the study by Williams 2001, fewer infants in the spinal anaesthesia group had post-operative apnoea in the absence of pre-operative apnoea but this was not statistically significant.
Due to the small sample sizes and inadequate data supplied, subgroup analyses were not possible except for looking at the subgroup receiving preoperative sedatives.
The results of this systematic review should be interpreted with caution due to the small sample size, the bias introduced by poor randomisation and the inadequacy of intention to treat analysis in all four studies. The overall results find no evidence that spinal anaesthetic is more effective than general anaesthesia as regards the incidence of post-operative morbidity. However, once we analysed the data after exclusion of the ketamine group in the Welborn 1990 study there was a statistically significant reduction in the incidence of post-operative apnoea in the spinal anaesthetic group. With such small numbers it would be difficult to comment on the homogeneity of the studies, however tests for heterogeneity are non-significant for all outcome measures. Furthermore, the studies reported both short and long apnoeas. For the purpose of this systematic review, we concentrated on long apnoea . Three of the studies used a definition for apnoea as a cessation in breathing for 15 seconds or less associated with bradycardia, and in the study by Krane 1995, they used the definition of 10 seconds or less associated with bradycardia. None of these definitions fulfilled the NIH 1987 definition of apnoea or the criteria prespecified in this review.
Continuous outcome variables for length of surgery, average length of hospital stay and temperature on admission to recovery were reported as means. No standard deviations and confidence intervals were available and therefore our interpretation is based on the conclusions of the individual authors.
Anaesthetic failure was analysed in three categories: anaesthetic placement failure, anaesthetic agent failure, and need of repeated attempts to achieve successful placement of anaesthesia. Overall, there were more technical failures in the spinal group. For every seven infants having a spinal anaesthetic one failed to achieve accurate placement of the spinal needle. For every three patients having a spinal anaesthetic, one experienced an anaesthetic agent failure, requiring additional anaesthetic agent. None of the studies addressed the issue of why there were so many technical failures, and they did not describe the degree of training or pre-study experience of the anaesthetic staff involved in the placement of spinal catheters.
The evidence to date does not support a clinically meaningful benefit of spinal anaesthesia over general anaesthesia for preterm infants undergoing inguinal herniorrhaphy in early infancy. However, studies performed so far are small. The potential benefits of a reduction in postoperative apnoea have to be weighed carefully against the high failure rate to achieve the accurate placement of a spinal needle and the high rate of anaesthetic agent failure. An important outcome, not measured in any of the studies, would have been operator satisfaction, as an awake infant under spinal anaesthesia may prove more technically challenging to operate on than one under general anaesthesia.
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Krane 1995 | Randomised single center trial Blinding of randomisation:
can't tell Blinding of intervention: no Blinding of outcome assessment: yes Complete follow up: yes |
Ex-premature infants (<36 weeks gestation) Corrected gestational
age < 51 weeks. Undergoing surgical repair of inguinal hernia ASA physical class I or II Major exclusions: significant chronic lung disease, known symptomatic congenital heart disease or symptomatic central nervous system disease. Pre operative 12 hour measure of respiratory rate and respiratory pattern in addition to saturation monitorng |
Spinal anaesthesia (N=10). General anaesthesia (N=8) | Any post operative oxygen desaturation. Post operative respiratory support Anaesthetic placement failure Anaesthetic agent failure |
Apnoea- cessation of respiratory movement for >10 seconds Haemoglobin oxygen desaturation was defined as a decrease of SpO2 to less than 90% for 10 seconds or more |
B |
| Somri 1998 | Randomised Single centre trial Blinding of randomisation: can't tell Blinding of intervention: no Blinding of outcome assessment: unknown Complete follow up: yes |
Infants born < 37 weeks gestation or < 60 weeks post
-conceptional age and/or with one of the following a) A history of neonatal respiratory distress syndrome b) BPD documented by radiography c) History of pre operative apnoea |
Spinal anaesthesia ( N=24). General anaesthesia (N=20). |
Postoperative apnoea/bradycardia Post operative analgesia Post operative respiratory support Average length of hospital stay Anaesthetic placement failure Multiple placement attempts |
Spinal anaesthetic failures were excluded from analysis. | B |
| Welborn 1990 | Randomised Single centre Blinding of randomisation: can't tell Blinding of intervention: no Blinding of outcome assessment: yes Complete follow up: yes Preterm infants < 37 weeks . ASA physical status I or II Anaesthesia < 51 weeks post conceptional age All undergoing inguinal hernia repair |
36 former preterm infants< 37 weeks corrected to 51 weeks
post conceptional age ( 35-51 weeks). Healthy infants Exclusion criteria: Cardiac, neurologic, metabolic disease or receiving methylxanthines or caffeine. |
Spinal anaesthesia divided into 2 groups, IIa and IIb. IIa spinal with preoperative ketamine (N=9), IIb spinal with no ketamine (N=11). General anaesthesia (N=16) | Post operative apnoea/bradycardia Post operative respiratory support Length of surgery Temperature on recovery |
Post operative apnoea/ bradycardia results differ within subgroups IIa and IIb | B |
| Williams 2001 | Randomised Single centre trial Blinding of randomisation: yes ( random number tables) Blinding of intervention: no Blinding of outcome assessment: yes Complete follow up: yes |
28 patients undergoing inguinal herniotomy. Born < 36 weeks
gestation. Post conceptional age < 46 weeks. Exclusion criteria: Pre- existing cardiac, neuromuscular and metabolic diseases. Pre-operative haemoglobin and respiratory function were noted |
Spinal anaesthesia (N=14). General anaesthesia (N=14) | Post operative apnoea/ bradycardia Anaesthetic placement failure |
Spinal anaesthetic failures were excluded from analysis | A |
| Study | Reason for exclusion |
| Kunst 1999 | Study published in letter form . This was a prospective randomised controlled study of 17 patients comparing post operative cardio-respiratory events in preterm infants undergoing spinal anaesthesia compared with general anaesthesia. Required outcomes not reported. Personal communication unsuccessful |
Krane EJ, Haberkern CM, Jacobson LE. Postoperative apnea, bradycardia, and oxygen desaturation in formerly premature infants: prospective comparison of spinal and general anesthesia. Anesth Analg 1995;80:7-13.
Somri 1998 {published data only}
Somri M, Gaitini L, Vaida S, Collins G, Sabo E, Mogilner G. Postoperative outcome in high risk infants undergoing herniorrhaphy: comparison between spinal and general anaesthesia. Anaesthesia 1998;53:762-766.
Welborn 1990 {published data only}
Welborn LG, Rice LJ, Hannallah RS, Broadman LM, Ruttiman UE, Fink R. Postoperative apnea in former preterm infants: prospective comparison of spinal and general anesthesia. Anesthesiology 1990;72:838-842.
Williams 2001 {published data only}
Williams JM, Stoddart PA, Williams SAR, Wolf AR. Post-operative recovery after inguinal herniotomy in ex-premature infants: comparison between sevoflurane and spinal anaesthesia. Br J Anaesth 2001;86:366-371.
Kunst G, Linderkamp O, Holle R, Motsch J, Martin E. The proportion of high-risk preterm infants with postoperative apnoea and bradycardia is the same after general and spinal anaesthesia. Can J Anaesth 1999;46:94-95.
* indicates the primary reference for the study
Cote CJ, Zaslavsky A, Downes JJ, Kurth D, Welborn LG, Warner LO, Malviya SV. Postoperative apnea in former preterm infants after inguinal herniorrhaphy. Anesthesiology 1995;82:809-822.
Frumiento C, Abajian JC, Vane DW. Spinal anesthesia for preterm infants undergoing inguinal hernia repair. Arch Surg 2000;135:445-451.
Henderson-Smart DJ. Recurrent apnoea. Bailliere's Clinical Paediatrics 1995;3:203-222.
Henderson-Smart DJ, Steer P. Prophylactic caffeine to prevent postoperative apnea following general anesthesia in preterm infants (Cochrane Review). In: The Cochrane Library, Issue 4, 2002. Oxford: Update Software.
National Institutes of Health Consensus Development Panel on Infantile Apnea and Home Monitoring. Pediatrics 1987;79:292-299.
Peevy KJ, Speed FA, Hoff CJ. Epidemiology of inguinal hernia in preterm neonates. Pediatrics 1986;77:246 -247.
Rescorla FJ, Grosfeld JL. Inguinal hernia repair in the perinatal period and early infancy: Clinical considerations. J Pediatr Surg 1984;19:832-37.
Sims C, Johnson CM. Postoperative apnoea in infants. Anaesth Intens Care 1994;22:40-45.
Tobias JD, Burd RS, Helikson MA. Apnea following spinal anaesthesia in two former pre-term infants. Can J Anaesth 1998;45:985-989.
Welborn LG. Perioperative complications in the former preterm infant. Current Rev Nurs Anest 1997;19:157-168.
01.01 Apnoea/bradycardia occuring 12-24 hours following completion of operation
01.02 Any oxygen desaturation occuring 12-24 hours following completion of the operation
01.03 Use of post-operative analgesia
01.04 Use of post-operative respiratory support
01.05 Post-operative apnoea with preoperative sedatives excluded
01.06 Anaesthetic placement failure
01.07 Anaesthetic agent failure
01.08 Repeated attempts to achieve successful placement of anaesthesia
01.09 Post-operative apnoea with no pre-operative
apnoea
| Comparison or outcome | Studies | Participants | Statistical method | Effect size |
|---|---|---|---|---|
| 01 Spinal anaesthesia versus general anaesthesia | ||||
| 01 Apnoea/bradycardia occuring 12-24 hours following completion of operation | 3 | 108 | RR (fixed), 95% CI | 0.69 [0.40, 1.21] |
| 02 Any oxygen desaturation occuring 12-24 hours following completion of the operation | 1 | 18 | RR (fixed), 95% CI | 0.91 [0.61, 1.37] |
| 03 Use of post-operative analgesia | 1 | 44 | RR (fixed), 95% CI | 0.42 [0.15, 1.18] |
| 04 Use of post-operative respiratory support | 1 | 98 | RR (fixed), 95% CI | 0.09 [0.01, 1.64] |
| 05 Post-operative apnoea with preoperative sedatives excluded | 3 | 99 | RR (fixed), 95% CI | 0.39 [0.19, 0.81] |
| 06 Anaesthetic placement failure | 2 | 90 | RR (fixed), 95% CI | 7.38 [0.98, 55.52] |
| 07 Anaesthetic agent failure | 2 | 62 | RR (fixed), 95% CI | 9.13 [1.26, 66.26] |
| 08 Repeated attempts to achieve successful placement of anaesthesia | 1 | 44 | RR (fixed), 95% CI | 9.24 [0.54, 157.57] |
| 09 Post-operative apnoea with no pre-operative apnoea | 1 | 32 | RR (fixed), 95% CI | 0.33 [0.04, 2.83] |
Prof David J Henderson-Smart
Director
NSW Centre for Perinatal Health Services Research
Queen Elizabeth II Institute for Mothers and Infants
Building DO2
University of Sydney
Sydney
NSW AUSTRALIA
2006
Telephone 1: +61 2 93517318
Telephone 2: +61 2 93517728
Facsimile: +61 2 93517742
E-mail: dhs@perinatal.usyd.edu.au
Dr Michele O'Brien
Anaesthetist
Department of Anaesthetics
The Children's Hospital at Westmead
Corner of Hawkesbury Road and Hainsworth Street
Westmead
NSW AUSTRALIA
2145
Telephone 1: +61 2 9845 0000
E-mail: MicheleO@chw.edu.au
| This review is published as a Cochrane review in
The Cochrane Library 2003, Issue 3, 2003 (see www.CochraneLibrary.net for
information). Cochrane reviews are regularly updated as new evidence
emerges and in response to comments and criticisms, and The Cochrane Library
should be consulted for the most recent version of the Review. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}