
The Assistant Secretary for Health and Surgeon General chaired the third and final review of progress in achieving Healthy People 2000 objectives for Mental Health and Mental Disorders. The review was organized by the Center for Mental Health Services of the Substance Abuse and Mental Health Services Administration and the National Institute of Mental Health, National Institutes of Health, co-lead agencies for this Healthy People priority area. The discussions among the participants addressed three principal topics – 1) Resilience: The Road to Health; 2) Access and Availability of Quality Care in Evolving Delivery Models; and 3) Mental Disorders and Their Impact on the Global Burden of Disease.
Resilience
6.6 The proportion of people aged 18 and older with severe, persistent mental disorders (excluding substance abuse disorders) who sought help from community mental health services was 34.6 percent in 1994, an increase to more than double the 1986 baseline. This surpasses the year 2000 target of 30 percent.
6.7 The proportion of people aged 18-54 years of age (non-institutionalized, non-rural, white, black, or Hispanic) with a 12-month major depressive disorder who obtained treatment was 34.2 percent in the early 1990s, reflecting little change from the previous decade.
6.8 The proportion of people aged 18 and older who sought help (e.g., from a family member, minister, or rabbi) in coping with personal and emotional problems increased from 11.1 percent in 1985 to 18.9 percent in 1995. The year 2000 target is 20 percent. People with disabilities sought help for such problems at rates of 14.7 percent in 1985 and 26.6 percent in 1995. The target is 30 percent.
6.9 In 1994, 35 percent of people aged 18 and older who reported experiencing significant levels of stress did not take steps to reduce or control their stress, a considerable increase from 24 percent in 1985. The year 2000 target is 5 percent.
Evolving Service Delivery Models
6.10 In 1996, there was only one State in which all jails had established official protocols to engage mental health, alcohol and drug, and public health authorities to facilitate identification and appropriate intervention to prevent suicide by male inmates. The year 2000 target is to have all States establish such protocols.
6.11 The year 2000 target is to have 40 percent of work-sites employing 50 or more people provide programs to reduce employee stress. In 1992, 37 percent did so, an increase of more than a third from 1985. In 1999, only 26 percent offered stress management programs at the work-site, but 48 percent of work-sites provided stress management either on-site or through the work-site health care plan.
6.12 Two clearinghouses/networks have been established to provide information about self-help resources and groups for people with serious mental illness and their families. During the 1990s, both became accessible by 800 numbers and through the Internet. The year 2000 target to provide coverage for all the States has been met.
6.13 This objective could not be updated due to limitations in the data collected.
6.14 This objective could not be updated due to limitations in the data collected.
Burden of Mental Disease
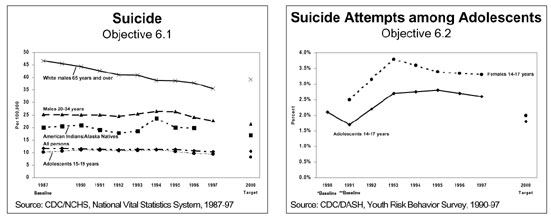
6.1 The age-adjusted rate of suicide for the total population decreased from 11.7 per 100,000 in 1987 to 10.6 in 1997, nearly meeting the year 2000 target of 10.5 per 100,000. Over the same time period, the rate of suicide for select populations also generally decreased, as depicted in the first graph.
6.2 The incidence of injurious suicide attempts among adolescents aged 14-17 moved away from the year 2000 target of 1.8 percent, increasing from 2.1 percent in 1990 to 2.6 percent in 1997, as depicted in the second graph.
6.3 No data are available to update the objective to reduce to less than 17 percent the prevalence of mental disorders in children and adolescents. In 1988, the prevalence was 20 percent.
6.4 Data representative of the national population for non-institutionalized, non-rural, white, black, or Hispanic persons aged 18-54 estimate a one-year prevalence of mental disorders (exclusive of substance abuse) as 20.4 percent in 1981-1985, decreasing to 16 percent in 1990-92. The year 2000 target for this objective (10.7 percent) was set based on a one-month prevalence from 1981-1985.
6.5 Among people 18 years of age and older who report experiencing stress within the preceding year, the proportion who experienced adverse health effects as a result decreased from 44.2 percent in 1985 to 33.9 percent in 1995, surpassing the year 2000 target of 35 percent. The proportion of people with disabilities (i.e., those who report any limitation in activity due to chronic conditions) who experienced such effects of stress decreased over the same time period from 53.5 percent to 49.1 percent. The target is 40 percent.
6.15 In 1990-92, data representative of the national population for non-institutionalized, non-rural, white, black, or Hispanic persons aged 18-54 estimate the one-year prevalence of depressive disorders as 11.1 percent, a slight increase from the 1981-1985 baseline of 10.9 percent. For women, the prevalence in 1990-92 was 13.1 percent, a slight decrease from the 1981-1985 baseline of 14.2 percent. The targets for the objective and sub-objective were set using one-month prevalence data and are not comparable with the 1992 updates.
DEVELOPMENTS
Data from the Youth Risk Behavior Survey indicate that 20 percent of students aged 14-17 have seriously considered suicide; 7.7 percent have attempted suicide; and 2.6 percent required medical attention after their suicide attempt.
A Harris Poll has reported that 60 percent of Internet users seek out health topics, of which depression ranks first. The World Health Organization ranks depression as the leading component of the global burden of disease for people under 45.
Since enactment of the Mental Health Parity Act of 1996, there has been substantial progress in closing the gap between physical illness and mental disorders in group health benefits. The majority of employers who made changes to comply with the Act reported that doing so did not increase their costs or require major changes to other benefits provisions.
Resilience approaches increasingly are being utilized to prevent and ameliorate mental disorders; they focus on the physical, psychological, and social resources of the individual throughout the life cycle.
A Nurse Home Visitation Program model in which nurses visit mothers beginning during pregnancy and continuing through their children’s second birthday strengthens the resilience of children and their mothers. The model has been replicated in multiple sites and is now being tested in special populations.
An experimental community-based study of mastery learning methods in first grade has been tested in 19 ethnically and demographically mixed public schools in Baltimore, Maryland, and is now being incorporated into teacher training curricula.
Half of all years lived with a disability in the U.S. involve mental disorders.
FOLLOW-UP
Determine the levels of exposure at which risk factors such as poverty, illness, and violence threaten mental health.
Seek a better understanding of resilience, its effectiveness, and its limits in reducing mental disorders and build on this understanding to control risk factors.
Explore the role of culture, spirituality, and family and community support as protective factors against the threat of mental disorders.
Ensure that mental health services reflect client needs and preferences.
Pursue further research on mental health as a factor in economic and social development.
Follow through on strategies and action to implement recommendations of the White House Conference on Mental Health, the Surgeon General’s Call to Action to Prevent Suicide, and Mental Health: A Report of the Surgeon General.
Stimulate the production of national, as well as State-specific, data on mental health and mental disorders, with break-outs for population groups.
Strive to achieve an optimal balance between funds allocated for treatment of mental disorders and those directed to prevention.
Increase access to mental health and substance abuse counseling in jails and other penal institutions.
PARTICIPANTS
Centers for Disease Control and Prevention
Georgetown University Medical Center
Harvard Medical School
Howard University
Johns Hopkins School of Public Health
National Asian Pacific American Families against
Substance Abuse
National Institutes of Health
Office of Disease Prevention and Health
Promotion
Office of Public Health and Science
Substance Abuse and Mental Health Services
Administration
Suicide Prevention Advocacy Network
University of Colorado Health Sciences Center
University of Maryland
ValueOptions
The World Bank
World Federation for Mental Health
Progress Review Page | Healthy People 2000 Home Page | ODPHP | NHIC