Sexually Transmitted Diseases Progress Review - June 1998

The Assistant Secretary for Health and Surgeon General chaired the third review of
progress on Healthy People 2000 (HP2000) objectives for sexually transmitted diseases
(STDs). As lead agency for this priority area, the Centers for Disease Control and
Prevention (CDC) presented an overview of actions needed to develop an effective national
system for the prevention of STDs in the U. S., as recommended by the Institute of
Medicine’s Report, The Hidden Epidemic: Confronting Sexually Transmitted Diseases.
Organized under three themes, the review outlined the steps necessary for: building
capacity to promote healthy sexual behaviors and to provide essential STD services;
focusing the system on populations with special STD prevention needs and challenges,
especially minority communities, adolescents, and uninsured populations; and improving the
quality of the system by building evaluation capacity and establishing performance-based
funding. The following objectives were considered in the overview and discussion:
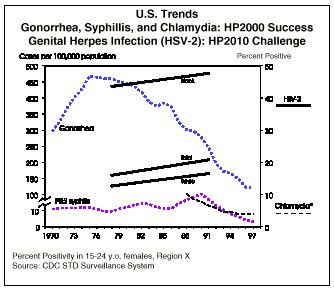
19.1 Since 1990, gonorrhea incidence has decreased by 56 percent, from 300 per
100,000 to 123 per 100,000. Although this rate remains above the HP2000 objective of 100
per 100,000, it is the lowest rate ever reported in the U.S. Between 1992 and 1997, the
black-to-white ratio decreased from 40 to 1 to 31 to 1. Adolescents aged 15 -19 account
for one-third of reported gonorrhea cases and have the highest rate of all age groups.
19.2 Chlamydia is the most commonly reported STD, but reported cases still
represent a gross underestimate of the true disease burden. The HP2000 target rate for
sexually active women under 25 years of age is 5 percent. Among family planning clients in
1996, the incidence rate of chlamydia in females aged 15-19 was 5.4 percent, and in
females aged 20-24, 3.4 percent. The states reported chlamydia incidence rates in
15-24-year-old females ranging from 2.5 percent to 10.9 percent. Women and men aged 15-24
who were screened in STD clinics had chlamydia rates of 11.2 percent and 14.4 percent,
respectively.
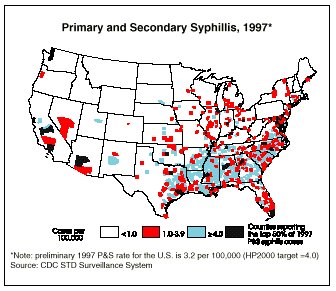
19.3 The incidence rate for primary and secondary syphilis in 1997, 3.2 per
100,000, is below the HP2000 target of 4 per 100,000. It is the lowest rate ever recorded
and represents an 84 percent reduction from the peak incidence in 1990. This improvement
is evident across all racial and ethnic groups, particularly for blacks, whose rate
decreased from 118 per 100,000 in 1989 to 22 per 100,000 in 1997. The black to white rate
ratio of primary and secondary syphilis decreased from 65 to 1 in 1990 to 44 to 1 in 1997.
The Hispanic to white rate ratio decreased from 6 to 1 in 1990 to 3 to 1 in 1997.
19.4 Congenital syphilis rates have fallen below the HP2000 targets for the
total population, blacks, and Hispanics. In 1997, the congenital syphilis rate for the
total population was 24.6 per 100,000 live births, down from 91.0 per 100,000 live births
in 1990. Rates for blacks and Hispanics respectively decreased from 417.8 and 134.6 per
100,000 in 1992 to 99.3 and 32.0 per 100,000 in 1997.
19.5 The annual number of first-time consultations for genital herpes increased
from the baseline of 163,000 in 1988 to 176,000 in 1997. However, one in five adults is
infected with HSV-2, the virus that causes genital herpes. There has been a 30 percent
increase in seroprevalence since the late 1970s. Among white teenagers, the prevalence is
five times higher than in the 1970s. The annual number of first-time consultations for
genital warts decreased from 290,000 in 1988 to 145,000 in 1997, surpassing the HP2000
target of 246,000. These numbers do not reflect the true disease burden since an estimated
one-half of sexually active adults are infected with the human papillomavirus (HPV),
including 34 percent of college-age women.
H I G H L I G H T S
The U. S. leads industrialized countries in rates
of STDs. For example, in 1996, the reported gonorrhea rate for the U.S. was
50 times that of Sweden, and the primary and secondary syphillis rate was 30
times that of Canada.
By 1997, 75 percent of all counties in the U. S.
had eliminated syphilis.
Half of all primary and secondary syphilis cases
were reported in only one percent (31) of U.S. counties in 1997, suggesting
that the disease is susceptible to elimination nationwide.
Numerous studies demonstrate at least a two- to
five-fold increase in the risk of new HIV infection when other STDs are
present. The presence of other STDs increases the likelihood of both
transmitting and acquiring HIV infection by increasing susceptibility and
infectiousness. Effective STD prevention has been demonstrated to reduce HIV
transmission by more than 40 percent.
Human papillomavirus (HPV) is the single most
important etiological risk factor for cervical cancer and has been
identified in more than 90 percent of cervical cancer cases.
One in 5 Americans has serological evidence of
genital herpes (HSV-2). Like other genital ulcer diseases, genital herpes
may increase the likelihood of HIV transmission per sexual exposure as much
as 10 to 50 times for male-to-female transmission and 50 to 300 times for
female-to-male transmission.
There is a strong link between STDs and adverse
pregnancy outcomes, including congenital infections, pre-term birth, and
low-birthweight. Screening and treating women during pregnancy for bacterial
vaginosis, gonorrhea and chlamydia may help to prevent thousands of these
adverse pregnancy outcomes.
Pelvic inflammatory disease (PID) is a leading
cause of infertility. A greater than 50 percent reduction in its incidence
is possible when young women are routinely screened for chlamydia.
Only 50 percent of local health departments provide STD prevention services and only 60
percent of those are able to see patients the same day they appear for services. With the
increased role of managed care organizations in public health, there is an opportunity for
the private sector to address population-based health concerns, such as STDs. In Georgia,
landmark legislation was signed into law that requires coverage of chlamydia screening by
individual or group accident and sickness insurance policies and managed care plans.
F O L L O W U P
Launch efforts to change attitudes toward STDs and
sexual health, emphasizing that the most common STDs are preventable and
treatable health problems that can have severe long-term consequences,
particularly for women, adolescents, infants and HIV Transmission.
Use multiple strategies for information outreach,
including the National STD hotline (800-227-8922), web sites, and other
interactive information sources, to provide quality information to both the
general public and health care providers.
Link categorical programs, such as family planning,
STD, and HIV, as well as funding mechanisms, such as the Maternal and Infant
Block Grant, to provide comprehensive services that address the needs of all
individuals and their partners at risk for STDs regardless of service venue.
Promote inclusion of STD prevention as a critical
component of the national HIV prevention strategy.
Build partnerships with managed care organizations
and assure that all third-party payers, especially Medicaid, provide
coverage for STD prevention services.
Focus efforts at the federal, state, and local
levels on the elimination of syphilis.
Build community-based STD prevention programs to
reach minorities, adolescents, incarcerated people, and other underserved
populations, in partnership with schools, correctional systems, faith-based
institutions, and other non-governmental organizations.
Increase skills and knowledge of the health care
workforce through training and continuing education to ensure that providers
are aware of the prevalence of STDs and can diagnose, treat, and counsel
patients at risk for STDs.
Strengthen the public health system’s capacity to address STDs through improved
surveillance and outbreak response.
P A R T I C I P A N T S
Academy for Educational Development *
American Social Health Association
California Department of Health Services
Centers for Disease Control and Prevention
Columbia University School of Public Health
Family Planning Council of Southeast PA, Inc.
Georgia Department of Human Resources
Harvard Pilgrim Health Care
Health Resources and Services Administration
Illinois Department of Public Health**
Metropolitan Interdenominational Church (TN)
National Association for People with AIDS
Office of Disease Prevention and Health Promotion
Office of Population Affairs
Pan American Health Organization
Society for the Advancement of Women’s Health Research*
University of Alabama at Birmingham
White House Office of National AIDS Policy
* Also representing the STD Prevention Partnership
** Also representing the National Coalition of STD Directors

David Satcher, M.D., Ph.D
Assistant Secretary for Health and
Surgeon General
Back to Progress Review Page
|

