This staff working paper was prepared solely to aid discussion and
does not represent the official views of the Council or of the United
States Government.
Medical Care and the Common Good
By Thomas W. Merrill, Ph.D. and David G. Miller, Ph.D.
Health and medical care have long been objects of moral concern and controversy in the United States . Today, it is common knowledge that millions of Americans lack insurance and thus access to needed care, that the costs of health care are high and growing at an alarming rate, and that the quality of care is mixed. These are problems of widespread concern among Americans—just as the proposed solutions to these problems are matters of pervasive controversy. In the midst of the ongoing debates about the relative priority of these problems and the effectiveness of the proposed solutions, the President's Council on Bioethics hopes to accomplish one aim: to contribute to a sustained focus on the ethical questions at play in these debates. How should we think ethically about health care? How should we think about responsibility and obligation—about individual and social responsibility and obligation—in relation to human need to maintain health and to prevent as well as ameliorate disease?
Our asking these questions is motivated, in part, by the observation that debates about health care policy and reform often seem to turn on assumptions that distort or obscure matters: health care is often described and treated either as a commodity or as the subject of a right that individuals possess and polities are duty-bound to provide. Although there may be grounds for those assertions, they are rarely questioned or examined as claims worthy of careful scrutiny, especially in light of what is at stake in these debates: matters of critical importance to all Americans simply because every American is human and, as such, is vulnerable to illness and needful of healing. In the following, we subject these claims to scrutiny and ultimately conclude that medical care is a human good, specifically an essential element of the common good, and that our society has an obligation to ensure that its citizens who need it have access to it.
In justifying this obligation, we make crucial distinctions between health, health care, and medical care. By “health,” we mean the well-functioning of the human being, and by “health care,” we mean that care necessary for maintaining and preserving an individual in a state of health. By “medical care,” we mean the care that an individual needs when he experiences that departure from health known as illness and when the cause of that illness is objectified as disease or injury. “Health care” is directed to the preservation of health and the prevention of disease and injury through such measures as routine physical examinations and preventive care. “Medical care” is directed to the cure or amelioration of disease or injury, goals that depend on the ministrations of physicians, nurses, and other healing professionals. Depending on the nature of the affront to health, medical care may take one of several forms, that is, it may be emergency, catastrophic, or chronic care. In matters of health, illness, and disease, those distinctions—particularly the distinction between health care and medical care—are important in thinking about individual and collective responsibility and obligation. Every human being should be concerned with his health, and most of us do not think that we have an obligation to secure the health of every other individual. Nonetheless, we argue that medical care is an appropriate object of public concern and a potential motivator of public action.
We develop this argument in four sections. Section One, “Problems of American Health Care,” provides a brief summary of the contemporary problems of American health care and, thus, situates our ethical questions in the relevant context. Although our task here is not to propose or defend specific policy mechanisms for solving these problems, we do contend that some of the more prominent policy proposals risk encouraging us to view health care in distorted ways.
Section Two is concerned with the distortions inherent in seeing health care as a commodity. This view is clearly at work in some proposals for consumer-driven health care, which involve, we will argue, myopic views of the moral realities of the relationship between physician and patient, a relationship distinguished by the vulnerability of patients, the inescapable authority of physicians, and the necessity of trust. The efficacy of the relationship depends on the physician's worthiness of the patient's trust and on the patient's willingness to trust the physician.
Section Three focuses on a different conception of health care—as the object of a right possessed by individuals. Although this conception is fueled by the recognition of the truth that health is a universal aspiration and need, we contend that the language of rights, like that of markets and commodities, can easily skew our moral perceptions and deliberations.
In Section Four, we turn to our arguments on behalf of a different conception of what should be the guiding principle in our debates about what is wrong with and what should be done to improve health care in the United States . We argue that the focus of our moral concern should be medical care—that is, emergency, catastrophic, and chronic care—and that a good society has an obligation to make sure that its citizens have access to it.
I. The Problems of American Health Care
The problems of American health care—especially the problem of access—have been targets of unrealized reform and resolution for almost a century. In 1915, the American Association for Labor Legislation proposed a national insurance system, but the plan was defeated, in large measure, due to the opposition of the American Medical Association and other groups. In the 1940s, a coalition of U.S. Senators and Representatives advocated an expansion of the Social Security system to cover physician and hospital care for workers and retirees. Despite the eventual endorsement of President Harry Truman, this plan was also unsuccessful. In 1965, advocates of reform triumphed when President Lyndon Johnson signed broadly supported legislation to establish Medicare, which covers care for the elderly and disabled, and Medicaid, which provides care for the poor. In the 1970s, Senator Edward Kennedy and Representative Marsha Griffiths sought to replace the private health insurance industry with government-based health insurance, and President Richard Nixon countered with a plan that would have preserved the private insurance industry within a system of universal coverage. Neither of those national health insurance plans was enacted. The last attempt at systemic reform was launched in 1993 and 1994 when President William Clinton proposed a sweeping health care reform package that also failed, despite initial indications of wide public support. 1
The reasons for this nearly unbroken record of frustrated reform vary from era to era and proposal to proposal. As for the stalemate of the last decade and a half, it, too, has multiple and varied causes, but one is undoubtedly this: there is not one overarching problem with American health care; there are several formidable problems. Any differential diagnosis of the ills of our country's “system” would include: the problem of access, the most salient symptom of which is the mounting number of uninsured individuals; the problem of escalating costs; and the problem of mixed quality. Moreover, the complexity of the challenge of health care reform is such that the oft-discussed solutions to one problem will likely exacerbate the others. And so it is that our anxieties about health care are several: we worry about the numbers of the uninsured, who do not get the care they need; we worry about the rising costs of health care, which have outpaced cost growth in other sectors of the economy, pressuring the budgets of individuals and families and threatening to overwhelm spending on other public needs in federal and state budgets; and, we worry about quality, particularly in light of the evidence that perhaps as much as one-third of the health care delivered in the United States brings little or no benefit to the patients who receive it. These are ultimately moral anxieties that issue in ethical questions. One such question is the focus of this white paper: How should we think ethically about health care? This is not an abstract question posed in isolation from the very concrete problems of American health care. It is, rather, a question whose answers shape both our diagnosis of and our proposals for treating these problems. Thus, to prepare the way for a proper posing of this question it is important to enter into this context. We begin with the problem of the access, and specifically, the problem of the uninsured.
A. The Problem of Access and the Uninsured
In today's debates about health care reform, there is an obvious sense of moral urgency, a concern for the fact that millions of individuals in the United States do not get needed care. In our current context, a key means to the end of getting requisite care is insurance. Thus, the population upon which this concern tends to be focused is the population of the uninsured. An uninsured person is unlikely to get all of the care that an insured person gets. According to some estimates, the uninsured receive only about half of the care that the insured receive.2 Getting less care generally results in having substandard health outcomes, especially if the uninsured are poor and sick at the outset of treatment. In a study by the Institute of Medicine , the often deplorable outcomes of being uninsured included death: according to the Institute, some 18,000 deaths a year are due in some significant measure to being uninsured.3 To be sure, the uninsured can obtain some care in emergency rooms, but that care tends to be sporadic, uncoordinated, and often too late to control some preventable health problems. Thus, although our concern about people not getting needed care embraces a wider population than the uninsured, investigating the uninsured offers very concrete and useful ways of understanding—and ultimately addressing—the broader problems of access.
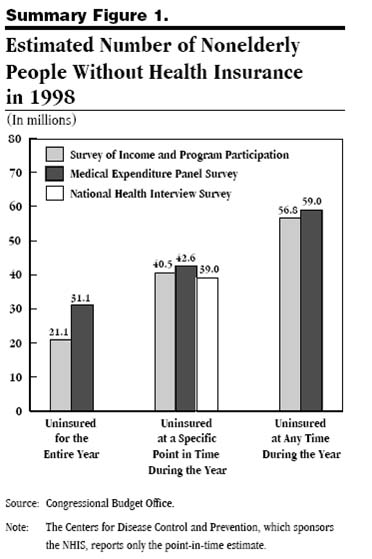
In understanding the problem of the uninsured, answers to two questions are central: first, how many uninsured persons are there in the United States ? And second, who are they? The most cited answer to the first question is this: there are, according to the U.S. Census, approximately 47 million uninsured persons in the United States .4 This one figure, however, conveys only one dimension of the problem, for it is an estimate of how many people in the country are uninsured on any given day . Studies also have shown that a significantly larger number of people—around 60 million—go without insurance during a given year and that perhaps as many as 80 million are uninsured at some point in two years. Many of the individuals captured in those larger totals are uninsured for relatively brief periods of time, perhaps while they are between jobs. By contrast, within these larger totals there is yet another population of individuals who are chronically uninsured—who go without insurance for a full year or more. The number of people who remain uninsured for at least one year has been estimated at 20 million in one study and at 30 million in another.5 Other, more recent studies have counted 17 to 18 million individuals in the group defined by chronic uninsurance of at least four years duration.6
Each of these estimates has different implications for how we think about and assess the likely effects of varying lengths of uninsurance on those who are uninsured, as well as on the health care system itself. For example, even brief periods of uninsurance, such as those caused by transient unemployment or job changes, can be problematic. Changing insurance may mean changing physicians with resulting disruptions in continuity of care—disruptions that may allow health problems to emerge and fester. In addition, there is always the possibility that the briefly uninsured may experience a catastrophic injury or illness, which may prove to be financially catastrophic as well. In the potential for these sorts of problems, one major limitation of our currently employer-based insurance system can be seen: the lack of insurance portability. And given the churning and the flux mirrored in those large totals of 60 to 80 million people, the insurance companies have little incentive to invest in preventive care because it is unlikely that they will maintain the requisitely stable client base required for a good return on their investment. If these are the effects of brief periods of uninsurance, one can, by extrapolation, conclude that the impact of chronic uninsurance is potentially more devastating, as the previously cited study by the Institute of Medicine suggests.
Figure 1:7
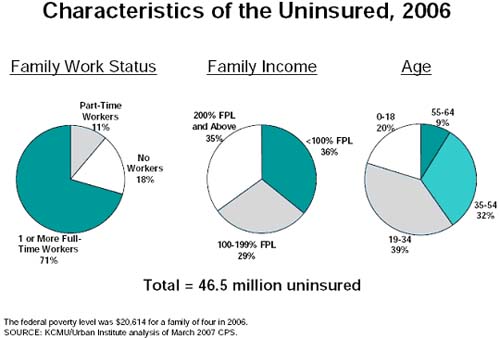
As for the second question— Who are the uninsured? —the most succinct answer is this: the uninsured population is heterogeneous. Unlike the population covered by Medicaid (primarily, mothers and children with incomes under a certain level) or by Medicare (everyone above a certain age as well as the disabled), there is no single defining characteristic that all or even a majority of the uninsured shares. There are, however, associations between being uninsured, on the one hand, and, on the other, such demographic characteristics as income, employment status, age, ethnicity, citizenship status, and geography:8
- Income: About a third of the uninsured population have annual incomes below $25,000, about a third make between $25,000 and $50,000, and the remaining third have yearly incomes of $50,000 or more. Thus, the lack of insurance is not necessarily a result of having a low income, although that is likely the case with the chronically uninsured. Nonetheless, the more a person makes, the less likely he or she is to be uninsured.
- Employment status: Employment in larger companies usually carries with it the benefit of health insurance, while employment in smaller companies—especially those with fewer than 50 employees—often does not include that benefit.
- Age: Nearly 40 percent of the uninsured are young adults between 19 and 34 years of age.
- Ethnicity: Racial minorities are more likely to be uninsured than Caucasians. Of all ethnic groups, Hispanics are the most likely to be uninsured.
- Citizenship status: Noncitizens or naturalized citizens are more likely to be uninsured than native-born citizens. Persons who are not citizens make up a sizeable fraction of the total number of the uninsured—more than a fifth.
- Geography: The South and the West have higher rates of uninsured persons than do the Northeast and the Midwest.
Figure 2:9
From the preceding statistics and demographic correlations, a complicated story about the uninsured emerges. Analyzing the ranks of the uninsured in terms of the length of their status as such reveals levels of concern—about the effects of even brief periods of uninsurance and about the unquestionably damaging impact of chronic uninsurance. Although the typical uninsured person is not necessarily poor (at least in relation to the federal poverty line), the poor are more likely to be uninsured than are the rich. Indeed, the near poor are far more likely to be uninsured than other Americans: according to some studies almost 70 percent of the uninsured population has household income under three times the federal poverty line.10 Also with respect to income, there is the curious problem posed by that fraction of the uninsured with relatively high annual incomes who seem to have chosen not to purchase insurance. These and other dimensions of the problem of uninsurance are all relevant to identifying and clarifying the sources of our ethical concern, especially when that concern is directed to the question of how we should think about individual and social responsibility for health care. But within this problem, the plight of the chronically uninsured—the individuals who lack insurance for long periods of time—is arguably cause for our most acute concern.
B. The Problem of Health Care Costs
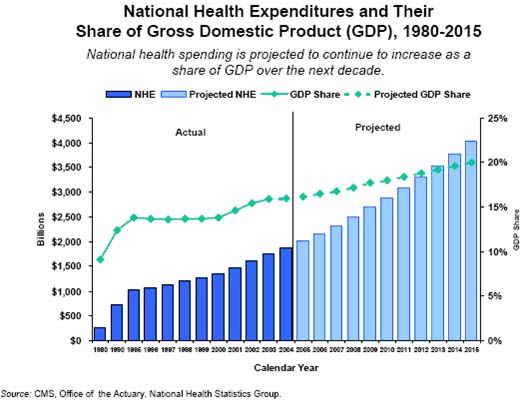
The startling growth in the ranks of the uninsured has occurred in tandem with an alarming growth in the costs of health care—indeed, the problems are related and thus the effort to solve one or the other is all the more complicated. Here, we focus on the problem of cost, although we will, from time to time in what follows, spell out its connections with the problems of uninsurance and quality. We begin with a caveat: it is difficult, perhaps impossible, to determine the “right” level of national spending on health care. A comparative analysis shows, however, that the United States spends more on health care than its peers in the industrialized West. In fact, it spends about $2 trillion a year, which is 16 percent of the gross national product or $6,700 per person. Moreover, the growth rate of health care spending exceeds that of every other sector of the economy. On average, since 1970, health care expenditures in the United States have increased 2.5 percent faster than the growth rate for the gross domestic product as a whole.11
One could argue that rising costs in and of themselves either are not or should not be cause for concern, at least not on par, for example, with the growing ranks of the uninsured. As noted, there is no preordained fraction of the national income that should be spent on health care. If costs in another sector of the economy were rising at a comparable rate, we might not be pleased with the situation, but it is not clear that we would, therefore, define the situation as an ethical problem. Rising health care costs, however, make it difficult to solve or ameliorate the problems of the uninsured, present the nation with exceedingly difficult budget and policy choices, and put pressure on individual and family budgets.
Figure 3:12
Consider, first, the impact of rising health care costs on individuals, families, and employers. The effects of rising health care costs can be measured by comparing the amount that the United States spends per capita on health care to the median family income. By that measure, our national per capita spending on health care is about 14.6 percent of the median family income, up from 11.4 percent as recently as 2000. Although insurance premiums do not always rise at the same rate or at the same time as overall health spending, increased insurance premiums have been a factor in the growth in the ranks of the uninsured in recent years, particularly among higher income Americans making more than $50,000 or $75,000 per year. Moreover, insofar as rising health care costs depress wages or keep wages from growing as quickly as they would have otherwise, increasing health care costs have other deleterious effects on individuals and families. Most economists argue that, despite appearances, employers are not really paying the insurance premiums of their employees. Rather, the insurance premium paid by the employer is simply a part of the total compensation package for the employee. Because of the tax exemption for health insurance, it makes sense for employees to take part of their compensation as untaxed health benefits rather than as taxable income. For most Americans, employers choose insurance providers and plans and arrange financing, but employers do not bear the final cost of the insurance premiums. Insurance premiums are viewed as merely one component of the total amount of compensation paid by employers to their employees. Rising health care costs, therefore, divert compensation received from take home pay to insurance and thereby slow the growth of wages. Again, those data alone might not issue in a conclusion that health care costs are “too high,” particularly in the absence of some estimate of whether the costs are worth the benefits. They do, however, indicate why health care costs are an object of concern for many Americans.
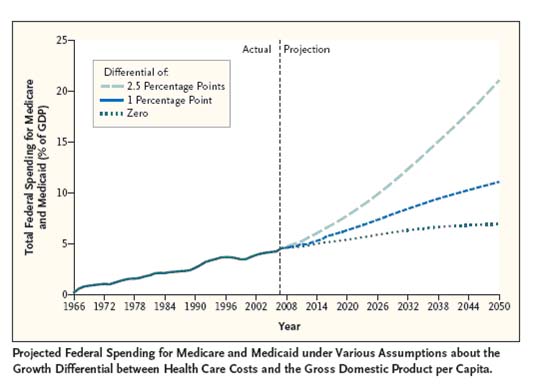
Rising health care costs are generating pressures and difficulties for state and federal budgets as well. Through Medicare, Medicaid, the Veteran's Administration, and other programs, the states and the federal government pay for about 45 percent of total health care spending in any given year.13 For the governmental bodies that subsidize those programs, rising health care costs yield hard choices among such measures as reducing benefits, restricting eligibility, or cutting other public programs—and sometimes result in their use of all three measures. Health care costs constitute the single largest expense in most (if not all) state budgets, and they are rising far more quickly than tax receipts. Their ripple effects include pressures to restrain or to cut other public programs, most frequently funding for public higher education.14 For the federal government, rising health care costs are—and will remain—decisive in choosing among national needs and priorities and, with time and in the absence of concerted change, will leave little room for real choice. The Congressional Budget Office (CBO) predicts that federal spending on Medicare and Medicaid will rise from the 4.6 percent of gross domestic product spent today to 5.9 percent in 2017;15 the primary driver of these projected increases will not be the aging of the population, but rather cost escalation in health care. According to CBO director Peter Orszag: “If costs continue to grow at the same rate over the next four decades [as they have in the last four], federal spending on Medicare and Medicaid would reach about 20 percent of GDP by 2050—roughly the same share of the economy that the entire federal budget accounts for today.”16
Figure 4:17
C. The Problem of Health Care Quality
In explicating the problems of American health care, particularly the ways in which those problems are interrelated, we have noted how increasing costs are implicated in the growing number of uninsured. What about costs and quality? Are increases in the former associated with improvements in the latter? There is no consensus among health policy analysts regarding whether the high costs associated with sophisticated, technology-intensive care yield benefits proportionate to their cost. By some measures of population health—for example, infant mortality and life expectancy—the United States does not do well in comparison to such countries as Australia, Canada, Germany, New Zealand, and the United Kingdom. Those comparisons, however, are controversial, especially with respect to the question of whether a given problem—for example, infant mortality—is due to health care system defects or to more pervasive socio-cultural factors.18 Here we set aside these issues in order to focus on quality-related evidence that is not so contested—evidence of ineffective and inefficient care.
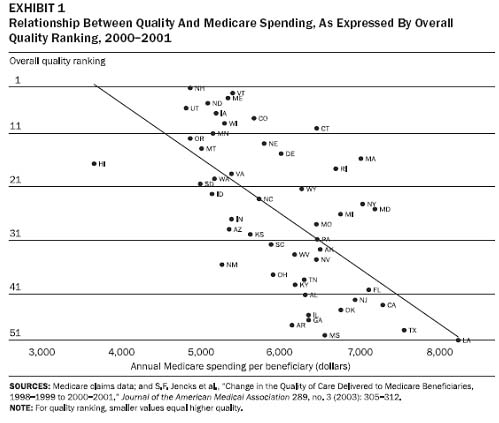
That evidence has been gathered and presented in the body of scholar literature whose central conclusions are two-fold: the quality of American health care is mixed at best, and the amount of resources spent on health care varies greatly in different regions of the country without any correspondingly observable differences in health outcomes. For example, a study in the New England Journal of Medicine found that clinical practice guidelines for the most effective diagnoses and treatments were being followed and patients were receiving recommended care only 54.9 percent of the time, and a recent Institute of Medicine report estimated that there are 98,000 deaths from medical error every year.19 And researchers at Dartmouth led by Jack Wennberg and Eliot Fisher20 have shown that the amount of money spent per capita on Medicare recipients varies widely between different areas of the country—by almost threefold—even after controlling for differences in age, race, and sex. As Eliot Fisher argued in a presentation to the Council in March 2008, the correlation between cost and quality is low, as is illustrated by the figure below. Wennberg and Fisher conclude that much of the health care spending in Medicare, between 20 and 30 percent, does not bring added health benefit, and there is probably a similar proportion of ineffective care in private health care.21 Economists suggest that, in many cases, American health care spending may be at the “flat of the curve,” that is, at the place in a cost-benefit analysis when further resources may not bring more benefit but less, perhaps through greater risk of medical error.22 Taken as a whole, these findings lead some observers to conclude that a considerable portion of health care spending in the United States —which, in light of the fact that health care accounts for 16 percent of GDP, means considerable sums of money—goes to health care spending that cannot be shown to improve health outcomes.23
Figure 5:24
* * *
A blunt, succinct summation of the preceding problem analysis might read as follows: we worry that some of us receive more care than is needed, others receive less than is needed, and the rising cost of care contributes to everyone's anxiety about both our personal budgets and the national budget. The most obvious solutions to these problems seem to lead in different and perhaps even contradictory directions. We might like to do something about the uninsured, but proposals for the government to act directly to help, whether by enrolling them in a public program or by subsidizing their purchase of private insurance, runs into the inevitable objection that our current obligations to provide Medicare seem unsustainable in the long term. If we were to make a public commitment to helping the many uninsured directly, would we not put ourselves at the mercy of the ever-rising costs of health care? In turn, if there is some consensus that the situation of the uninsured is a real problem for us, what to do, if anything, about rising costs is a topic of serious controversy among health policy experts. Some argue that if Americans want to spend their money on care of perhaps doubtful value, they should be able to do so, but that they should have to pay for it themselves. Those proponents would increase deductibles and co-payments in order to induce greater cost-consciousness on the part of patients in order to make them into more prudent consumers of health and medical care, thus restraining cost and perhaps encouraging improvements in quality as well. Some studies show, however, that patients, and particularly poor patients, have difficulty distinguishing necessary from unnecessary care, so such measures may worsen the problem of access to health or medical care. Others argue that the only proven way to keep costs down is more government intervention, perhaps through some form of single-payer health care. Yet that change, despite the claims of its advocates that it is the only ethical and sustainable option, has never proven popular with the American people at large.
For us, what is striking is how these various solutions presuppose certain understandings of what it is that is in dispute and of how to frame public discourse. The recent trend toward consumer-driven health care, for example, implicitly treats health or medical care as nothing more and nothing less than another commodity in a free market. That view makes a certain amount of sense if the primary problem in American health care is patients blithely consuming large amounts of health care without thought to the cost. Indeed, that view might plausibly claim to encouraging responsibility and prudent stewardship. But, taken by itself, that vision does not have very much to say about the numbers of Americans who, we have good reason to believe, are not getting the care they need. Those who see the primary problem in American health care as the uninsured might well claim that we need to assert strongly a moral imperative to get care to everyone. They often talk as though health or medical care is the kind of thing to which human beings, as human beings, have or ought to have a right. While one can understand why someone might be tempted to see health or medical care through either one of these lenses, we argue in what follows that both are one-sided and possibly dangerous if taken as the whole truth about health or medical care. To anticipate, the view that health or medical care is best seen under the rubric of commodity fails to do justice to the traditional orientation of the medical profession toward the care for human beings in need; the view that human beings have a right to health and medical care sends the wrong message about individual and social responsibility for health and threatens to become far too expansive. We take up these matters in the final section, after which we argue that medical care—but not health care—is best seen as a human good and as critical to the common good.
II. Is Health Care a Commodity?
Whether, or to what extent, health care should be conceived and treated as a commodity is a matter of persistent disagreement. Some analysts and policymakers contend that health care is a commodity like any other in a market economy and that a relatively free market will solve or ameliorate our problems with cost and quality. Others oppose this view, arguing that health care cannot and should not be treated as a market good among others and that it is special, in large measure, due to its unique properties and to the moral realities of the relationships between patients and health professionals. This dispute between “marketists” and “medicalists” has deep roots in distinctively American ways of thinking, especially about public policy.25 As we have previously suggested, policy debates often evolve in ways that tend to obscure or to blur the focus on questions that are ethical and philosophical in nature—such questions as: Is medical care best described or interpreted as a commodity? What is gained, and what is lost, by this way of seeing the matter? Here, we examine the rationale for conceiving and treating health care as a commodity and conclude that, perhaps despite the intentions of its advocates, this view does not adequately capture, and in some ways even distorts, essential aspects of health care, especially the moral realities of the relationship between a patient and a physician.
A. The Case for Treating Health Care as a Commodity
What is a commodity? That is, what are the essential features that commodities of different types share? And what is the rationale for conceiving and treating health care as a commodity?
First, for every commodity there is a quantitative value, a price, that specifies what “a seller will receive for surrendering it and a buyer will part with in order to acquire it.”26 The price of a commodity denotes its worth, which fluctuates with the changing dynamics of the supply of, and the demand for, the given commodity. Conditions of short supply and high demand usually drive prices up; surplus supplies and low demand usually drive prices down. Second, a commodity is fungible: it is completely “interchangeable with other goods of like type and quality.”27 Third, the value of a commodity is “instrumental, not intrinsic”: its worth is a function of its ability to satisfy the desires of its owner. Unlike objects that have intrinsic value to those who possess them, objects of purely instrumental value have little to do with the owner's identity.28 Finally, commodities are distributed through markets, which organize the interactions of buyers and sellers and, as noted, they are distributed in accord with their price, rather than, say, need— “to each according to his or her willingness (and ability) to pay.” And, the participants—the buyers and the sellers—in a market also possess the feature of fungibility. Markets operate on the assumption that the only difference between buyers and sellers is that the former wish to acquire what the latter possess.
Turning from the question of what is a commodity to the question of why we might be inclined to conceive and treat health care as a commodity, we begin with consumer-driven health care, whose proponents cite some of our well-known problems as support for the explicit commodification of health care. They point above all to the evidence of rising costs and mixed quality, including the amount of inefficient or inappropriate care, and they argue that these problems are caused, in part, by various distortions in the market for health care.29 Chief among these distortions is the tax exemption for the purchase of employer-based health insurance, which encourages employees to get more generous insurance policies than they would otherwise—policies that insulate patients from the true costs of their care.
Advocates of consumer-driven health care appeal, as well, to the dictum that “an individual is most prudent with his or her own money,” which explains why the well-insured have little or no reason to question or reject excessively expensive care or care of uncertain value. Thus, these advocates contend that the solution to these problems is to remove the insulation, to make patients—that is, consumers—more aware of the price of health care and, thereby, more cost-conscious toward their care. In keeping with the logic of this argument, proponents recommend an ideal form of insurance, that is, a high deductible plan combined with a health savings account for other out-of-pocket spending. Such plans protect health care consumers against high costs, while high deductibles give them incentives to be more prudent about using their resources for most routine health care spending. In brief, in a system of consumer-driven health care, patients would be, first and foremost, savvy, hard-nosed consumers, motivated by self-interest to find and make the best deal. Armed with information and able to take their health care dollars elsewhere, such consumers could theoretically hold doctors and other health care professionals accountable and thus spur them to drive down costs and provide better quality.
In its purest form, consumer-driven health care draws on democratic beliefs about the sufficiency of the individual's ability to recognize and act upon the right course of action for himself at any given time. It envisions individuals with the ability to negotiate their care, and it suggests that relationships between physicians and patients are, at bottom, contractual, reached between two parties of roughly equivalent knowledge and resources—that is, between a patient who is nothing more and nothing less than a consumer and a physician who is, likewise, a service provider, brought together to negotiate with each other with the aim of realizing interests that are ultimately each individual's own.30
B. The Impact of Commodification
Consumer driven health care implicitly, as well as explicitly,
offers a particular account of the relationship between patients
and physicians—an account that we believe is out of sync with the
moral realities of this relationship. In this relationship, born
of the patient's need for healing and of the physician's promise
to heal, inequality is inescapable and essential. The very meaning
of patient, after all, is someone who endures pain or affliction,31
and he or she comes to the doctor in a state of need and vulnerability.
To be sure, many if not all of us like to think of ourselves as
self-sufficient beings, standing tall and requiring the permission
of no one to be ourselves and to act as we wish. But needing a physician,
even when we are well, is in no small tension with such proud aspirations.
As patients, we must bare our bodies, and in some sense, our souls,
revealing what we usually share with only our closest intimates,
if at all. Moreover, illness and disease undermine our proud assertions
of autonomy. They remind us that we are dependent, that being healthy
and being ill are states that are not within the ambit of our strict
control— i.e., that we are vulnerable to our social and
genetic inheritances and to the variety of misfortunes that befall
us as we make our way through the world, and we are thus needful
of the aid and assistance of people we hardly know.
From the physician, a patient needs not simply a service or a good (although services and goods surely support the physician's functions and activities), but even more, the physician's judgment about what can and cannot be done to meet his needs in a particular situation. And in the most extreme cases, such as when a patient is lying in the emergency room after a car accident or waiting for brain surgery, the patient can hardly be the savvy, hard-nosed consumer that we expect in other areas of the economy.
The physician, on the other hand, presents herself to a patient first and foremost as a professional, armed with superior knowledge and judgment about the patient's medical condition.32 A professional is literally one who pro-fesses something, that is, promises in public to do something.33In the case of the physician, she promises to help or aid the patient as best she can. By her very presence before the patient, she offers implicit assurance that she is competent in the skills and practice of medicine, and will use those skills for the benefit of the patient, and not with a view to larger social goals, to her own self interest, or to anyone else's good. As such, the professional presents herself as something different from the seller of a commodity, who avowedly aims to strike the best deal for himself. Moreover, the training and skills of the physician are not and cannot be the proprietary knowledge of the individual physician: although she has expended her own effort to acquire that competence, the knowledge itself and the opportunity to acquire it depend on the community of doctors and the larger community of citizens. The physician holds that competence in trust, a trust that brings with it certain obligations to orient her thinking and her actions to the good of the patient.
In addition to his technical competence, the physician has another, often overlooked advantage: unlike the patient, she is not sick. Neither her proud claim to self-sufficiency nor her very existence is called into question by the all-too-real evidence of vulnerability. For these reasons, the physician can and must act as an authority to the patient. She must tell the patient things the patient does not want to hear, and she must prescribe courses of treatment that the patient may not want to follow.
At this juncture, it is important to add the critical qualification that the patient presents himself to the physician as a human being whose dignity and right to self-determination demand respect in any medical decision or course of treatment. Although the physician may give orders—and in some respect must give orders—she can only do so if the patient is prepared to accept them. Thus, in addition to scientific knowledge and technical skill, the physician must have some facility with the arts of persuasion and with the prudent exercise of her epistemic, technical, and experiential authority. To put the matter succinctly: the physician's authority is successfully exercised only to the extent that she is worthy of, and she encourages and elicits, the patient's trust. It is in light of the centrality of trust that the relationship between physician and patient is described as a fiduciary—a trust-based—relationship oriented to the good of the patient. The moral realities of this relationship—the realities of compromised but cherished autonomy, of inequality ameliorated by trust, of shared commitment to the good of healing—may be distilled into a single phrase: beneficence-in-trust.
C. Health Care and the Physician-Patient Relationship: Evidence of the Market Ethos and Commodification
Those moral realities are the focus of growing concern within and beyond the health professions—concerns that have to do with phenomena and trends that indicate how pervasive the market ethos has become in contemporary health care and how far down the path to commodification we have already traveled. Consider, for example, the roiling controversy within medicine over the alleged influences of pharmaceutical companies on clinical decision making, that is, on physician prescribing practices. At issue here is the argument that marketing practices introduce illegitimate bias into the process of clinical reasoning and divert physician judgment such that interests other than the patient's benefit become controlling. Another prominent example of these concerns is reflected in the claim that fee-for-service medicine introduces strong incentives for physicians to do more than is necessary—to order more diagnostic tests and to perform more interventions. The motivations for “doing more” are undoubtedly complex but in them many see the footprints of defensive medicine—of leaving no stone unturned as a means of avoiding litigation—and of the simple desire to maximize reimbursement. Whatever the motivation, it seems clear that the phenomenon of overtreatment described in the previous analysis of the problem of quality is related to the encroachments of a market ethos into health care.
That ethos is reflected as well in the behaviors and expectations of patients, many of whom seem induced to think of themselves, first and foremost, as consumers. For the would-be buyer of a commodity, the market ethos is distilled in the dictum, caveat emptor —let the buyer beware. The encouraged wariness is to be cultivated and reflected in (1) self-education about one's health or disease to ensure that as a consumer, the patient encounters the physician on as level a playing field as possible with regard to knowledge-based power; and (2) in the demand that everything possible be done, if only because, like any other commodity, the function of the care sought is to satisfy one's desires, and one ought to obtain as much of a good as one can for the same expenditure. And, thus, on the side of patients, who are increasingly described as consumers of health care, we also see evidence of the market ethos. In the literature of bioethics, the impact of that ethos is evident as well in the argument that the relationship between physician and patient is best seen and lived as a contractual relationship that brings together autonomous equals for the purposes of negotiating what the one will provide (that is, sell) and the other will receive (that is, buy).
D. The Dangers of Interpreting Health Care as a Commodity
Both the impetus and desire to interpret health care as a commodity are understandable given our culture's traditional reliance upon markets as the primary means by which goods and services are distributed and the primary framework within which goods and services are interpreted. Moreover, many market ideals are the ideals of all social interactions: all participants have full knowledge, understanding, and rationality; there is equal accessibility for all; there is no collusion or dishonesty on the part of any participants; there is full transparency in all transactions; etc. Nevertheless, viewing health care as a commodity, and the concomitant view of patients as consumers and health care professionals vendors, does a serious injustice to the realities of the relationship between the patient and the professional, to the moral standing and moral obligations of the patient and the professional, and to the nature of the particular good (health care or medical care) that is being provided and its centrality to the patient's very self. The ineradicability of beneficence-in-trust from the relationship between the patient and the health care professional makes any attempt to reduce health care to the status of a mere commodity dangerous and illegitimate.
III. Is There a Right to Health or Health Care?
The argument that health care is or should be seen as a commodity appeals to the traditionally American embrace of the market as the forum for the expression of liberty. Another argument, the claim that there is a right to health care, also appeals to concepts with deep roots in the American tradition of political and ethical thought—the concepts of equality and of rights. These concepts figure prominently in our contemporary debates about the plight of the uninsured, a plight that is often conceptualized as an unjust denial of something, in some sense, owed to every American. Here, we ask if this construal of health care is true to—if it reveals or obscures—the moral realities of health, illness, and disease. We begin with a taxonomy of rights and then turn to a prominent explication and defense of the argument that there is a right, not only to health care but to health itself; this brief on behalf of a right to health has been developed in a series of steps by Norman Daniels of the Harvard School of Public Health.34 The case for a right to health care or to health itself is, in our judgment, open to serious objections.
A. A Taxonomy of Rights
What is a right? The most basic meaning of a right is this: a right is a legitimate claim on the part of an individual on others to do or to forebear from doing some particular thing. It is not simply a desire, a want, or an ability to do something. The assertion of a right always entails an appeal to justice. Thus, the claim of a right always implies a correlative duty on the part of another: my right to life always implies your duty not to kill me. Rights in this sense are often characterized as absolute and unconditional with the danger that they may be asserted as if, once claimed, they require no further justification.
Rights may be distinguished as either natural or civil and negative or positive. In the American tradition, the Declaration of Independence provides one authoritative articulation of natural and negative rights. According to the Declaration, all men are created equal and possess certain inalienable rights, chief of which are rights to life, liberty, and the pursuit of happiness. These rights are natural because they exist prior to governments, which are always instituted by human beings. At most, governments recognize those rights; they do not create them and therefore cannot take them away. These rights are negative because their primary function is to protect certain liberties or freedoms from infringement either by governments or by others. In John Locke's phrase, rights create “fences to tyranny” by demarcating the sphere in which the individual can live his life as he or she sees fit. A right in this sense does not provide a title of property to any one thing in particular but only preserves the freedom of the individual to live his or her own life free of interference by others.
There are, as well, civil and positive rights, which are related to the concept of statutory entitlements. Unlike a natural right, a civil right is a creature of a particular polity, and is dependent for its existence and protection on that polity and, in the case of the United States , is usually understood as protected by the Constitution. For example, the right to vote is not a natural right, because it is a privilege to vote in a particular polity and does not belong to all human beings as such. But it does institutionalize or formalize the more fundamental right to consent to or reject government, which is, according to the Declaration, a natural right. And so civil rights realize or make effective rights that are more properly understood as natural. Civil rights should also be distinguished from statutory entitlements, which are legal recognitions of the claim of an individual to some activity, good, or service. For example, when we acquire a driver's license, we acquire a right to drive motor vehicles under certain conditions in certain jurisdictions. Where civil rights are conventional reflections of more fundamental natural or human rights, statutory entitlements are based only in regular law.
Positive rights, on the other hand, suggest a claim on some specific thing, whether an opportunity or a good. One of the more prominent articulations of positive rights is the United Nations Universal Declaration of Human Rights. 35 Like the American Declaration of Independence, the Universal Declaration of Human Rights speaks of the moral equality and dignity of all human beings. Unlike the Declaration of Independence, however, it goes beyond rights to life and liberty and speaks of rights to social security (Art. 22), a right to rest and leisure (Art. 24), a right to an education (Art. 26), and a right to participate in the cultural life of the community (Art. 27). More importantly for our purposes, the Universal Declaration also speaks of “a right to a standard of living adequate for the health and well-being of [an individual] and his family” (Art. 25), including, among other things, a right to medical care.
The preceding taxonomy orients our discussion about health and health care as putative rights—and underscores the need for clarity in deliberating about the question, is there a right to health care or health? In light of the preceding taxonomy, a more specific form of this question might be, is there a negative right to health or health care? If there is such a negative right, it would appear to be a version of the more general right to life: it would be, that is, a right not to have one's health interfered with by others. Similarly, one could speak of a right to health care and mean no more than a statutory entitlement—just as, for example, it might be said that once one reaches a certain age, one has a right to Medicare benefits. Yet neither of these ways of speaking captures the usual meaning of the claim that there is a right to health care. Those who make such a claim may seek its fruition in a statutory entitlement to the goods and services included under the rubric of health care, but the roots of such an entitlement must be sought in something other than a legislative decision—that is, in some conception of justice or natural rights or human rights. In other words, the proponents of a right to health care must mean that such a right is analogous to a civil right, which is instituted by a specific polity for the sake of its members but which is grounded in an appeal to natural rights. The proponents of a right to health care must mean, therefore, that we ought to see that right as something like a constitutional civil right, like the right to vote, and to make good on their assertion, they must show that health is a matter of justice.
B. The Argument on Behalf of a Right to Health Care
As previously noted, Norman Daniels is, perhaps, the most prominent, articulate advocate of a right to health care—indeed, of a right to health itself.36 In his testimony to the Council, he described his thinking on this topic as evolving in at least two stages, each of which presents distinct and somewhat different considerations as well as important questions. Daniels's initial argument, developed in 1985 and presented in Just Health Care (and elsewhere), turned on the connection between justice, equality of opportunity, and health and health care. A core commitment of liberal democratic societies, Daniels argued, is to promote and to protect equality of opportunity for all of its citizens. Because health care promotes health, understood as normal functioning, and because health is a precondition for realizing opportunity, health care is important to the promotion and protection of opportunity. If justice requires society to protect opportunity, then justice gives special importance to health care. Thus, it is reasonable, on Daniels's account, to speak of a right possessed by individuals to health care—that is, of a legitimate moral claim on the part of individuals to health care that political communities have an obligation to meet.37 Daniels thus provides the kind of argument that, if successful, would support the assertion in the Universal Declaration of Rights of a right to medical care.
As Daniels relates in Just Health , matters prove to be more complicated and he concludes that his initial argument was incomplete and in need of a two-fold elaboration. First, according to Daniels, the concept of “equality of opportunity” is too abstract to convey much about its limits or more generally the recurrent problem of rationing scarce resources. In practice, reasonable people disagree about what those limits are or ought to be—for example, about what procedures should or should not be covered by an insurance plan. If we do not have a principle that allows us to resolve rationing problems, Daniels argues, we need to turn to processes and institutions that will allow us to resolve them in a fair, participatory fashion, a necessity that Daniels has elaborated in a number of works.38
Second, the argument assumes that access to health care is a , if not the , primary determinant of health. But this assumption is flawed: of the factors that epidemiologists think affect health, commonly called the “social determinants of health,” access to health care is not the most important, and may well be less important than other factors. Those factors include a wide variety of nonmedical aspects of life: “income and wealth, education, political participation, the distributions of rights and powers, and opportunity.”39 But if health care is special because it protects health and thus opportunity, and all of these other things affect health even more than health care, how can they fail to be special in the same way access to health care is? The moral logic of a “right to health care” thus also leads to a “right to health.” More precisely, it leads to a positive obligation on the part of a political society to redistribute, to the extent possible, all of those “social determinants of health” in the name of securing the equality of opportunity.40
C. Why Health Care Should Not Be Considered a Right
On our view, the idiom of rights is problematic when applied to health and health care. One problem is this: assertions of a right to health or health care project an inappropriate view of personal and collective responsibility.41 Although Daniels himself is careful to qualify his use of the term “right” to whatever is feasible under the circumstances, the term strongly implies an absolute and unconditional claim made by a person on a larger whole. Defined as the well-working of an organism as a whole, and closely tied to self-maintaining activity of that organism, health is not a state that is generated and sustained, as it were, wholly from without. It is true that, especially when suffering from disease or injury, our needs for healing are satisfied, in part, by medical and surgical procedures, by drugs and techniques. But that state of health and the process of healing itself are the dynamic outcome of exceedingly complex interactions between what is within and what is without, between our native dispositions and our environments. (It is for this reason that health itself also cannot be a commodity.) On this view, health has much to do with how we live and with our habits and customs: “we are in an important way responsible for our state of health.”42 Suggesting that health is the object of a right places a moral burden on the surrounding community and encourages us to see health as the kind of thing that may be demanded from others rather than something for which we are responsible. From this point of view, it is more prudent to begin by acknowledging the central importance of personal responsibility.
In addition to a problematic conception of responsibility, the claim that there is a right to health care entails a troublingly expansive view of justice. Here, the question is not one of which medical treatments are covered (which Daniels handles through procedural mechanisms); rather, the question is, what, if any, aspect of human life is outside the scope of the legitimate power of government once all the social determinants of health are asserted to fall within that scope? One might appreciate the necessity of moving from a right to health care to a right to health, once this argument for a right to health care has been granted. That move, however, suggests that the scope of moral obligation is virtually unlimited, as are the powers of government required to fulfill that obligation. Although reducing inequalities (or ameliorating the living conditions of the worst off among us) may well be the object of prudent statesmanship, claiming that the polity has a specifiable obligation to do so gives the government an almost unlimited reach.
Moreover, the phrase “equality of opportunity” blurs the difference between things that are or should be justly distributed by governments and things that are not. To speak of a “right to health” comes close to implying that individuals have a claim of justice for equality no matter what the source of inequality is. Although we make claims of justice against our fellows, do we really have claims of justice against nature or fortune? Such language runs the risk of raising expectations that are difficult if not impossible to meet and would require more political power than most of us would feel comfortable delegating. Daniels is surely right to point to all the determinants of health beyond “mere” access to health care. But precisely that evidence shows how slippery and expansive such a right must be.
There can be no doubt that the tension between equality and liberty runs deep in the American political tradition and that it will continue to be controversial among Americans of good will. However we resolve this tension as individuals, it is worth raising the fundamental question of whether the language of rights is the most appropriate framework for thinking about health and health care. As we have seen, the language of rights began in the Western tradition as an assertion of negative rights, understood as natural and virtually absolute. Such rights provide every individual, no matter how weak or powerless, with a barrier against the worst excesses of human wrongdoing. The difficulties with the language of rights, however, come into view when this idiom is applied to all of the complex realities of the moral lives of individuals and societies. The natural rights of the Declaration were both unconditional and limited in scope (albeit to fundamental matters of life and liberty), and it might be argued that their vitality depends in part on their clearly delimited sphere. But when the language of rights is extended to all areas of life, that language inevitably brings with it certain rhetorical baggage that makes prudence more difficult by far. By emphasizing the unconditional character of the right asserted, it makes what should be a conversation about the balancing of complicated and conflicting goods appear as a battle of uncompromising principles. By emphasizing the subjective right of the claimant and the corresponding duty of the rest of the world, it fosters an individualism that is forgetful of the responsibilities that always accompany rights. In Rights Talk , former Council member Mary Ann Glendon details some of these defects of the language of rights:
Our rights talk, in its absoluteness, promotes unrealistic expectations, heightens social conflict, and inhibits dialogue that might lead toward consensus, accommodation, or at least the discovery of common ground. In its silence concerning responsibilities, it seems to condone acceptance of the benefits of living in a democratic social welfare state, without accepting the corresponding personal and civic obligations. In its relentless individualism, it fosters a climate that is inhospitable to society's losers, and that systematically disadvantages caretakers and dependents, young and old. In its neglect of civil society, it undermines the principal seedbeds of civic and personal virtue. In its insularity, it shuts out potentially important aids to the process of self-correcting learning. All of these traits promote mere assertion over reason-giving.43
Above all, the idiom of rights distracts us from the necessity of prudence and sober judgment.
It seems evident that health and medical care is one of those areas in which a focus on “rights” does more harm than good. Any public deliberation concerning health and health care will have to grapple with complex questions of how to get care to those who are not now getting it, in a context of rising costs, both private and public, and of ineffective and inappropriate care. These are daunting matters that the idiom of rights tends to obscure rather than clarify. As Daniel Sulmasy puts it in a recent essay, absolute or negative rights, like the rights to life and liberty, entail duties of perfect obligation. But, because health and medical care are relative to the historical, economic, and social conditions of a given society, seeing them, in that way, as the object of a right does not make sense. Our duties with regard to those things can only be duties of imperfect obligation.44 As we saw in the last section, one danger is that patients will come to see health or medical care as commodities of which a rational person would try to consume as much as possible. The absolute character of a rights-centered interpretive framework would seem to accentuate that danger, and lead to expansive expectations that cannot be met. Moreover, there is a real danger that the assertion of a right to health or medical care, to say nothing of health, will provoke counter-assertions of right on the part of those being called upon to fulfill the right. Norman Daniels, of course, is not blind to these dangers and, as we noted, he proposes some institutions and processes to put limits on what services would be covered. The deeper worry, however, is that the rhetorical and philosophical baggage of the language of rights will have a logic of its own, no matter what we intend when we begin to use it in this arena. In the midst of the ongoing policy discussions and debates, we need to remember that how we think and talk about these matters has practical implications for how we design and implement policy.
Of course, recognizing the dangers of a rights-centered framework need not entail a denial of the moral intuitions and sensibilities that motivate recourse to such language. Those intuitions and sensibilities are often expressed in the conviction that a decent society does not countenance the avoidable suffering of its members—the millions who do not get care or who get care through less than optimal means. How to interpret and actualize that conviction is no small matter. It is to this question that we now turn.
IV. Neither a Commodity Nor a Right: Medical Care as a Critical Element of the Common Good
Our reflections thus far have led us to conclude that health care is not properly understood as either a commodity or as something to which individuals have a right. Neither category captures the particular nature of health care. We compensate medical professionals for providing care just as we compensate other service providers for their services. Nevertheless, we recognize that to be in need of care—especially medical as distinguished from health care—is to be in a unique condition: to be in need of medical care is to be in a vulnerable, existential state. This need is so fundamental to our identities and our aspirations that we are often tempted to see a right to medical care as a natural extension of our right to life itself. However, we do not consider our right to life to be a positive right; that is to say, we do not contend that a right to life establishes a legitimate moral or legal claim against humanity in general or against our particular society to provide us with whatever is necessary to sustain life. Thus, the special nature of health and medical care are adequately captured neither by the logic and language of commodities, nor by the logic and language of rights.
In this section, we examine medical care as a particular type of good. We argue that medical care shares some qualities of public goods, but it is best seen as a critical element of the common good, which gives it a special moral standing and makes a special moral demand on a society that seeks to establish a safe and fertile ground for its members' pursuit of happiness.
A. A Taxonomy of Goods and the Relationship of the State to Those Goods
With the traditional American emphasis on protecting and empowering the individual, much of public discourse focuses on the individual and on enforcing (negative) rights, that is, on removing obstacles to the exercise of individual liberty and on protecting private property and the individual's freedom to dispose of private goods as he or she wishes so long as that disposition is respectful of the safety, well-being, and rights of other individuals. Nevertheless, we also expect our government to “promote the general welfare.” The Bill of Rights establishes the boundaries within which our government operates as it seeks to promote and sustain an environment conducive to individual and societal flourishing, that is, to promote the common good . The most direct way in which it advances the common good is by providing and protecting both “public goods,” and, quite often, what we will refer to as “mixed goods.” Let us clarify what is meant by the categories of public and mixed goods and examine their relationship to the concept of the “general welfare” or the “common good.”
In our everyday lives, we usually find ourselves focused on private goods , that is, goods we own and can consume or trade with others as we see fit. In contradistinction to private goods, we earlier alluded to some goods that are commonly accepted as “public goods.” Strictly speaking, public goods are collective goods that (1) benefit all who receive them, (2) are automatically provided to everyone when they are made available to anyone, and (3) do not require removing the good in question from one person in order to provide it to another. The quintessential example of a public good is clean, breathable outdoor air: everyone desires and benefits from it, one cannot provide it to specific individuals while excluding others from it, and one does not have to take it away from one person in order to provide it to another. Another example of a pure public good is national defense: again, the benefits of a safe nation extend to all its citizens; when national security is provided to one individual, it is provided to all; and providing it to one individual does not entail removing it from another. Public goods are protected ( e.g. , clean air) or provided ( e.g. , national defense) by the state in order to enable all its members to pursue more effectively their projects, both individually and cooperatively. In addition to benefiting each individual citizen directly, the state's provision and protection of public goods strengthen community by sustaining an environment conducive to both individual and collective human flourishing.
The state's provision or protection of some public goods, such as public health and sanitation, may require individuals and groups to submit to certain procedures (for example, to being vaccinated) or to follow certain regulations (for example, properly labeling and or disposing of hazardous waste) that are intended to protect both individuals and the population as a whole. Vaccination protocols fight communicable diseases for the benefit of all. Universal vaccination is enforced (with a proviso for principled objection) despite the fact that some would prefer not to be vaccinated, because universal inoculation fosters an environment that is safer and more conducive to the good of all than it otherwise would have been. In such instances, the state requires that individuals make some sacrifices to help sustain the good of the collective and the common good, that is, to sustain the social union that allows them to more fruitfully actualize their potential as individuals and as a community.
Sometimes, public goods, such as protection of public health, require individuals to make sacrifices that will not benefit them directly as individuals. During outbreaks of untreatable infectious diseases, protecting public health may require us to quarantine infected individuals despite the fact that those individuals, themselves, will not benefit directly from the quarantine. Ordinarily, those individuals will willingly participate in such efforts because they will want to protect their friends, family, and compatriots from infection. Indeed, a sense of shared identity, shared fate, and shared responsibility—of community—is what Charles Taylor calls an “irreducibly social good.”45 The common good is an irreducibly social good.
To say that the common good is an irreducibly social good is to say that, like such goods as love and friendship, it cannot be reduced either to a commodity or personal possession or to a “right.” The common good is more than just the collective good or the aggregation of the goods of individuals; the sustenance of the social union, the community itself, is a meaningful source of moral value for its members. This is important to note because, frequently, our public discourse seems to encourage an atomistic individualism—a view of the person as social only insofar as she chooses to relate to others. There is a moral dimension of our lives and our identity— i.e. , our shared sociality, our unchosen social embeddedness and interdependence as beings born into families and communities—that is obscured when we focus on ourselves as autonomous, individualistic, economic agents asserting our rights over and against other equally independent individuals. Our identities, our sense of who we are, our self-conceptions, all are rooted in our belonging in, and to, a family, a community, a people with a common history, a common land, and with common commitments to shared ideals and ways of life. Public goods, collective goods, and the common good challenge us to recognize that moral dimension of human life. Unfortunately, we often take those social bonds for granted until some traumatic event shocks us into recognizing them. As a nation, we experienced such trauma in the wake of 9/11 and Hurricane Katrina; as individuals, families, and communities, we experience such trauma most commonly when we experience illness and injury.
There are some goods that are not purely public goods but which contribute to the common good and, as such, attain a status deserving of societal recognition. One such good is education. Like a public good, education does benefit those who receive it, and providing education to one person does not necessarily entail depriving another person of it. However, like a private good, it is possible to educate some individuals without necessarily educating everyone. Nevertheless, our nation has a long tradition of public education, which is based on arguments like this of Thomas Jefferson:
Education is here placed among the articles of public care, …[for] a public institution can alone supply those sciences which, though rarely called for, are yet necessary to complete the circle, all the parts of which contribute to the improvement of the country, and some of them to its preservation.46
Jefferson is using the phrase “public care” similarly to the way we have been using the term “common good:” as an element of the common good, education contributes to the preservation and improvement of the country as a whole (which is more than the sum of its parts) even as it directly benefits the individuals who are educated. The United States accepts that a certain level of education for all will help to sustain and enhance the common good. Moreover, it equips us individually not only with a sense of community and of our shared heritage, but also with skills and information that allow us to be better participants in public discourse and in civil society. Education is therefore treated like a public good, even though it is more accurately interpreted as a “ mixed good ”—a good that has some of the qualities of a private good, and some of the qualities of a public good.
It is worthwhile noting that while certified private education at all levels is permitted, and while higher education is encouraged and publicly assisted (through grants, financial aid to students, and through the establishment of state colleges and universities), the state has established a minimal level of education that it requires of all citizens. As a nation, we have decided that primary and secondary education are beneficial to individuals, to society as a collective, and to the common good, and we therefore not only provide access to all citizens but require citizens to receive a minimal level of education. Cultivating the intelligence of its citizenry is therefore an element of the common good, and as such is an object of moral concern for the state.
There are other goods that are often considered to be (or treated as) public goods which are actually mixed goods.47 One example would be potable water. Ordinarily, in the United States , there are adequate supplies of potable water for most people. However, when stores of potable water are limited—during disasters such as hurricanes, droughts, or contamination—providing potable water to one group may entail restricting or prohibiting access to another group. In those instances, potable water loses some of the qualities that would ordinarily cause us to see it as a public good, and it takes on qualities that we normally associate with private goods, i.e. , it is not automatically provided to everyone when it is provided to anyone, and providing it to some may actually entail depriving others of it. Even in those instances when it ceases to qualify as a public good, potable water retains a quality that causes us to see it as an element of the common good: it is something that everyone needs to sustain his or her life. Such mixed goods are also often referred to as “ primary goods ”48 or “basic goods” because a certain level of each person's need for those goods must be met before that person can (and in order for that person to be able to) actively participate in society and lead his life, regardless of what other goods he may desire or projects he may wish to pursue. In cases of extreme need and periods of unrest, the community's need to exercise fair, judicious, collective stewardship in order to protect and advanced the common good becomes more, rather than less, evident.
Society (as represented by governmental institutions) ordinarily provides, protects, and or regulates both pure public goods and a number of mixed goods in order to sustain the common good. Maintaining a safe public water supply, regulating industries to ensure breathable air and a relatively clean environment, maintaining systems of public sanitation and public health, maintaining domestic and national security, maintaining a legal system for resolution of disagreements and enforcement of laws, etc., all of those functions are conducive to the good of individuals as well as to the good of sustaining the social union that allows individuals and society as a whole to flourish.
Ordinarily, the distribution and exchange of private goods are left to markets, and markets, themselves, generally redound to the common good. Negotiations between those who supply and those who demand various goods and services usually encourage innovation, improvements in quality, and efficiency in both distribution and production of market goods and services. Of course, “free markets” are ideals: they presuppose perfect information is available and fully understood by all parties, perfect competition among sellers, perfect access to markets for buyers, and parity of power among the various agents participating in the market. To advance the common good, the state establishes and enforces regulations and standards to ensure that actual markets more closely approximate the ideal of “free markets.” It monitors and regulates the safety and marketing of everything from foodstuffs, to products for infants and children, automobiles, machinery, and pharmaceuticals; it establishes engineering and fire safety standards; it ensures occupational safety; it protects human subjects in research; etc. The state also provides and maintains public roads, air traffic control, and other elements of our nation's infrastructure. The state—that is to say, we, members of society, through our elected officials—invest our common wealth in research, education, and communications. All of those activities involve a harnessing of common wealth and the commonwealth for the common good.
The question we will now turn to is: what type of good is medical care, and how should the state relate to that good?
B. Medical Care as a Good
While we have already indicated why we have chosen to focus our attention on medical care rather than on health or health care, it is useful to review the distinctions among those goods, again, in light of our taxonomy of goods.
We can fairly easily define health as the adequate and ordinary well-working of an organism and its self-maintaining activity; however, assessing the “adequacy” of a person's health is complex. In many ways, the assessment of person's current state of health (and an assessment of the degree of healthiness to which a person can reasonably aspire) depends on a number of factors ranging from her medical history to her age, diet, activity level, etc. Similarly, there are innumerable ways in which one might try to maintain or enhance one's health. Our conceptions of “health” and “health care” are, therefore, expansive notions that threaten to “medicalize” practically every aspect of our lives. Optimal health is an ideal to which we aspire, and, as an ideal, it can generate an almost infinite number of ways in which we might maintain and enhance it—accompanied by a correspondingly expansive list of ways to care for health. Health and health care are clearly mixed goods (in that, like public goods, they benefit all individuals and they benefit the collective as well), and they are elements of the common good, since healthy, thriving individuals can help to establish a healthy, thriving people.
Nevertheless, medical care, care that is essential to the physical well-being of the organism, can be differentiated from the expansive conceptions of health and health care that we just described. As we discussed in our critique of the inadequacy of seeing medical care as a commodity, there is clearly a sense in which a person's health is inseparable from, and foundational to, a person's sense of “self.” Injury, disease, and illness are felt not merely as an assault on “a body;” they are an assault on the person . That assault is one of the “traumatic events” alluded to earlier, events that shock us into recognizing our dependence on others, our interdependence as social beings. When emergent or catastrophic injury or chronic disease assaults our bodies, our autonomy is compromised, and we are in dire need not only of attention to our physical needs, but also of communal support and reaffirmation of our interconnectedness and social worth. For that reason, “medical care”—care that is critical to addressing acute or chronic threats to the basic (although not necessarily the “optimal”) functioning of the organism—is so intimately connected to a person's sense of self that it must be recognized as a particularly important good.
Clearly, medical care is a primary good (as was acknowledged by the 1983 President's Commission) for it is something that one needs regardless of whatever else one may desire. Clearly, also, medical care is an element of the common good: ensuring that medical care is provided to those who need it fosters a sense of community and of security. Indeed, surveys over the past five years49 have consistently shown that the insured population's fear that their insurance may be inadequate and the uninsured population's fear of being unable to pay for medical care outrank their fears of losing their jobs, being unable to pay their rent or mortgage, or being the victims of violent crime or terrorist attack. For that reason, being assured that one will receive needed medical care is analogous to being assured that one will be protected from violence when or if such protection is needed. Like intelligence, health needs to be cultivated; and like national security, medical security is a primary concern of contemporary Americans.
In light of the value that our culture places on autonomy, conditions that warrant medical care are likely to be intimately related to their sufferer's sense of self-worth—particularly if the sufferer is marginalized or alienated for other reasons ( e.g. , poverty, mental illness, strained or non-existent familial relationships). Even those who have families and material resources often find dealing with catastrophic, emergent, and chronic medical conditions to be frightening, depressing, and demoralizing. For all of those reasons, medical care is an essential element of the common good.
C. Access to Medical Care Is a Moral Obligation of a Good Society
The United States first demonstrated its commitment to ensuring
that its most vulnerable members receive medical care many decades
ago, and it continues to uphold that commitment today in a number
of ways. Federal programs like Medicare, Medicaid, and S-CHIP provide
access to health and medical care to the elderly, the disabled,
some of the poor, and some children. In the health care programs
of the Veterans Administration that commitment benefits those who
have served their country in the armed services. Moreover, the federal
law EMTALA requires that emergency rooms treat anyone who seeks
treatment without regard to insurance status or ability to pay.
Federal and state governments help hospitals and physicians defray
some of the costs that patients do not pay through uncompensated
care funds. Finally, as a nation, we demonstrate our recognition
of the unique importance of health and medical care by exempting
the purchase of employer-based health insurance from taxes. In all
of these ways, we demonstrate that we recognize that medical care
is a special public concern worthy of our support.
Despite these efforts, approximately 47 million persons in the United States remain without any form of public or private coverage for medical care on any given day. EMTALA does ensure that all who request care in emergency rooms will be stabilized before being discharged, but this assurance does nothing to alleviate multiple causes for public concern: (1) the emergency stabilization and discharge of a patient does not ensure that the patient is actually capable of sustaining her condition upon discharge; (2) the failure of federal legislation to provide a dedicated funding mechanism for uncompensated care leaves emergency rooms vulnerable to financial hardship; (3) while the uninsured do get care (and often pay out of pocket for it), they do not get as much care as typical insured persons do;50 (4) moreover, according to a study by the Institute of Medicine, some 18,000 deaths a year are attributable in part to lack of insurance coverage.51 Clearly, there is ample reason to conclude that the number of uninsured is a problem for our society—particularly that portion of the uninsured that is involuntarily so due to an inability to afford insurance and a failure to qualify for entitlement programs. Given this state of affairs, we conclude that:
A good society that recognizes the equal dignity of its members can, should, and, indeed, must respond to such avoidable human suffering—especially a society as affluent as our own. Our society has a moral obligation, not to meet every conceivable health-related need of every citizen, but rather to ensure that its members—especially the vulnerable members of our society—have the requisite ability to meet their needs for emergency, catastrophic, and chronic care.
In reaching this conclusion, we refrain from taking a position on any particular way of rendering this societal obligation into workable public policy. Health care reform is a complex matter and numerous factors make reform difficult, especially the problem of rising costs. We are convinced, however, that we cannot afford to lose sight of the numerous Americans who are not getting the care that they need even as we consider these complicating factors. We recognize that our primary conclusion may lead to different intuitions about how to best approach fulfilling that obligation, but that fact does not hinder us from concluding that it is imperative that the United States ensure that all of its citizens have access to medical care when they need it.
_______________________
FOOTNOTES
1. For these points, see Bridget Harrison, “A Historical Survey of National Health Movements and Public Opinion in the United States ,” JAMA , March 5, 2003, Vol. 289, No. 9.
2. See Jack Hadley, John Holahan, Teresa Coughlin, and Dawn Miller, “Covering the Uninsured in 2008: Current Costs, Sources of Payment, and Incremental Costs,” Health Affairs , 2008, Web Exclusive 27, No. 5, w401-402.
3. Institute of Medicine , Hidden Costs, Value Lost: Uninsurance in America , 2003.
4. See Carmen DeNava-Walt, Bernadette Proctor, and Jessica Smith, Income, Poverty, and Health Insurance Coverage in the United States : 2006 , U.S. Census Bureau, 2007.
5. For a helpful discussion of these points and references to the relevant literature, see “How Many People Lack Health Insurance and For How Long?”, a 2003 paper from the Congressional Budget Office, available at www.cbo.org.
6. See MEPS Statistical Brief #183: “The Long Term Uninsured in America 2002-2005: Estimates for the U.S. Population under Age 65.” August 2007. Available at http://www.meps.ahrq.gov/mepsweb/
7. From “How Many People Lack Health Insurance,” p. 1.
8. For these facts, see Income, Poverty, and Health Insurance Coverage.
9. Chart from The Uninsured: A Primer , from the Kaiser Family Foundation, August 2007, p. 4. Available at www.kff.org.
10. See the data cited in Mark Pauly, “Conflict and Compromise over Tradeoffs in Universal Health Insurance Plans,” Journal of Law, Medicine, and Ethics , Fall 2004, p. 467.
11. For a helpful summary and discussion of these facts, see Health Care Costs: A Primer , from the Kaiser Family Foundation, August 2007, available at www.kff.org.
12. Table 1.1 from “An Overview of the U.S. Health Care System Chartbook,” Centers for Medicare and Medicaid Services, January 2007. Available at www.cms.gov/TheChartSeries/
13. See Table 1.3 of the CMS Chart Book cited above.
14. Ezekiel J. Emanuel and Victor R. Fuchs, “Who Really Pays for Health Care? The Myth of ‘Shared Responsibility',” JAMA , 2008, Vol. 299, No. 9, pp. 1057-1059. Emanuel and Fuchs write “the increasing costs of Medicaid and other government health care programs are a primary reason for the substantial increase in tuition and fees for state colleges and universities.”
15. “The Long Term Outlook for Health Spending,” Congressional Budget Offices, November 2007.
16. Orzag and Ellis, “The Challenge of Rising Health Care Costs,” NEJM , p. 1793.
17. Chart from Orszag and Ellis, “The Challenge of Rising Health Care Costs,” p. 1794.
18. Readers interested in these issues may consult the literature cited in our background paper for the June 2008 meeting of the Council, available at www.bioethics.gov.
19. Elizabeth McGlynn, et al., “The Quality of Health Care Delivered to Adults in the United States,” New England Journal of Medicine , 2003, Vol. 328, pp. 2635-2645; and Institute of Medicine, To Err is Human: Building a Safer Health Care System , 1999.
20. See, for example, Fisher's March 2008 presentation to the Council
21. See, among others, Jonathan Skinner, Elliot Fisher, and John Wennberg, “The Efficiency of Medicare,” NBER Working Paper No. 8395, available at www.nber.org.
22. Victor Fuchs, “More Variation in the Use of Care, More Flat-of-the-Curve Medicine,” Health Affairs , Web Exclusive, October 7, 2004.
23. Peter Orszag of the CBO suggests that as much 5% of GDP, or $700 billion a year, may be spent on health and medical care that cannot be shown to improve health outcomes. See Orszag, “Health Care and Behavioral Economics: A Presentation to the National Academy of Social Insurance,” May 29, 2008, pp. 4-5. Available at cbo.org.
24. Fisher referred to this chart in his presentation to the Council. Its source is Katherine Baicker and Amitabh Chandra, “Medicare Spending, the Physician Workforce, and Beneficiaries' Quality of Care,” Health Affairs , Web Exclusive, April 7, 2004, w4-187.
25. We borrow the terms marketists and medicalists from Sherry Glied's helpful discussion in her Chronic Condition: Why Health Reform Fails (1997), especially Chapter 2. For arguments that it is a mistake to see health care as special, see Richard Epstein, Mortal Peril: Our Inalienable Right to Health Care? (1997), and H. Tristam Engelhardt and Michael Rie, “Morality for the Medical-Industrial Complex,” New England Journal of Medicine , Vol. 319, No. 16, Oct. 20, 1988, pp. 1088-89. For the medicalist view, see Arnold Relman, A Second Opinion: Rescuing American Health Care (2007).
26. M. Cathleen Kaveny, “Commodifying the Polyvalent Good of Health Care,” The Journal of Medicine and Philosophy , June 1999, Vol. 24, No. 3, p. 209.
27. Ibid.
28. Ibid., at p. 210.
29. For one articulation of these critiques, see Regina Herzlinger's and James Capretta's presentations to the Council, available on our website. It should be noted that not all proponents of markets are advocates of the specific models usually associated with consumer-driven health care (health savings accounts with high deductible insurance plans); for an argument for that model, see David Gratzer, The Cure: How Capitalism Can Save American Health Care (2006).
30. In addition to deep roots in some aspects of American political culture, the “contractualist” view of medical ethics has some prominent defenders in bioethicists, such as Robert Veatch. See, for example, A Theory of Medical Ethics , Chapter 5, “The Triple Contract: A New Foundation for Medical Ethics” (1981). In fairness to Veatch, he is by no means a proponent of “consumer-driven health care.”
31. http://dictionary.oed.com/cgi/entry/50172866?query_type
=word&queryword=patient&first=1&max_to_show=10&sort_type=alpha&result
_place=1&search_id=ofRW-aS5hdT-5261&hilite=50172866. Accessed August 28, 2008.
32. For a more extended treatment, on which this discussion draws, see Dr. Edmund Pellegrino, “Toward a Reconstruction of Medical Morality: The Primacy of the Act of Profession and the Fact of Illness,” in Physician and Philosopher: The Philosophical Foundation of Medicine , ed. Daniel Sulmasy, OFM, 2001, pp. 18-36.
33. http://dictionary.oed.com/cgi/entry/50189445?single=1&query_type=word&queryword
=professional&first=1&max_to_show=10. Accessed August 28, 2008.
34. Professor Daniels presented his arguments to the Council in November 2006; a transcript is available at www.bioethics.gov.
35. For a helpful discussion of the genesis of the Universal Declaration, see Mary Ann Glendon, A World Made New: Eleanor Roosevelt and the Universal Declaration of Human Rights (2001).
36. For a more extended presentation of his views, see Just Health: Meeting Health Needs Fairly (2008).
37. For the use of the term “right to health care” in this context, see Just Health , p. 144.
38. See Chapter 4 of Just Health .
39. Just Health , p. 4.
40. For the use of the term “right to health,” see Just Health , p. 144; for discussion of the social determinants of health, see Chapter 3 of the same book.
41. For one articulation of this view, see Leon Kass, “The End of Medicine and the Pursuit of Health,” in Toward a More Natural Science (1985).
42. Kass, “The End of Medicine and the Pursuit of Health,” p. 176.
43. Mary Ann Glendon, Rights Talk: The Impoverishment of Political Discourse , 1993, p. 14.
44. Daniel Sulmasy, “Dignity and Bioethics: History, Theory, and Selected Applications,” in Human Dignity and Bioethics: Essays Commissioned by the President's Council on Bioethics , 2008, pp. 485-86.
45. Charles Taylor, “Irreducibly Social Goods,” Philosophical Arguments , 1995, pp.127-145.
46. Thomas Jefferson: 6th Annual Message, 1806. ME 3:423. Available at: http://etext.virginia.edu/jefferson/quotations/jeff1370.htm
47.It may actually be the case that during periods of extreme scarcity, all public goods become more like private goods.
48. The President's Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research identified medical care as a primary good in its 1983 report, Securing Access to Health Care , p. 16. The ethical framework expounded in that report provides a firm foundation for this Council's reflections herein.
49. http://www.kff.org/healthpollreport/CurrentEdition/security/upload/HSW0408.pdf
50. See Jack Hadley, John Holahan, Teresa Coughlin, and Dawn Miller, “Covering the Uninsured in 2008: Current Costs, Sources of Payment, and Incremental Costs,” in Health Affairs , 2008, Web Exclusive 27, No. 5, w401-402.
51.Institute of Medicine , Hidden Costs, Value Lost: Uninsurance in America , 2003.
|
