")

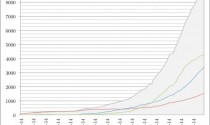
Alessandro Vespignani hopes that his latest work will turn out to be wrong. In July, the physicist from Northeastern University in Boston started modeling how the deadly Ebola virus may spread in West Africa. Extrapolating existing trends, the number of the sick and dying mounts rapidly from the current toll—more than 3000 cases and 1500 deaths—to about 10,000 cases by 24 September, and hundreds of thousands in the months after that. “The numbers are really scary,” he says—although he stresses that the model assumes control efforts aren't stepped up. "We all hope to see this NOT happening," Vespigani writes in an e-mail.
Vespignani is not the only one trying to predict how the unprecedented outbreak will progress. Last week, the World Health Organization (WHO) estimated that the number of cases could ultimately exceed 20,000. And scientists across the world are scrambling to create computer models that accurately describe the spread of the deadly virus. Not all of them look quite as bleak as Vespignani's. But the modelers all agree that current efforts to control the epidemic are not enough to stop the deadly pathogen in its tracks.
Computer models “are incredibly helpful” in curbing an outbreak, says infectious disease researcher Jeremy Farrar, who heads the Wellcome Trust research charity in London. They can help agencies such as WHO predict the medical supplies and personnel they will need—and can indicate which interventions will best stem the outbreak. Mathematical epidemiologist Christian Althaus of the University of Bern, who is also building Ebola models, says both WHO and Samaritan's Purse, a relief organization fighting Ebola, have contacted him to learn about his projections.
But the modelers are hampered by the paucity of data on the current outbreak and lack of knowledge about how Ebola spreads. Funerals of Ebola victims are known to spread the virus, for example—but how many people are infected that way is not known. “Before this we have never had that much Ebola, so the epidemiology was never well developed,” says Ira Longini, a biostatistician at the University of Florida in Gainesville. “We are caught with our pants down.”
To a mathematician, combating any outbreak is at its core a fight to reduce one number: Re, the pathogen’s effective reproductive rate, the number of people that an infected person in turn infects on average. An Re above 1, and the disease spreads. Below 1, an outbreak will stall.
Outbreak models typically assume that there are four groups of people: those who are susceptible, those who have been infected but are not contagious yet, those who are sick and can transmit the virus, and those who have recovered. A model, in essence, describes the rates at which people move from one group to the next. From those, Re can be calculated.
If the disease keeps spreading as it has, most of the modelers Science talked to say WHO’s estimate will turn out to be conservative. “If the epidemic in Liberia were to continue in this way until the 1st of December, the cumulative number of cases would exceed 100,000,” Althaus predicts. Such long-term forecasts are error-prone, he acknowledges. But other modelers aren’t much more encouraging. Caitlin Rivers of the Virginia Polytechnic Institute and State University in Blacksburg expects roughly 1000 new cases in Liberia in the next 2 weeks and a similar number in Sierra Leone.
Vespignani has analyzed the likelihood that Ebola will spread to other countries. Using data on millions of air travelers and commuters, as well as mobility patterns based on data from censuses and mobile devices, he has built a model of the world, into which he can introduce Ebola and then run hundreds of thousands of simulations. In general, the chance of further spread beyond West Africa is small, Vespignani says, but the risk grows with the scale of the epidemic. Ghana, the United Kingdom, and the United States are among the countries most likely to have an introduced case, according to the model. (Senegal, which reported its first Ebola case last week, was in his top ten countries, too.)
The models are only as good as the data fed to them; up to three-quarters of Ebola cases may go unreported. The modelers are also assuming that key parameters, such as the virus’s incubation time, are the same as in earlier outbreaks. “We might be missing the boat and we have no signal to indicate that,” says Martin Meltzer of the U.S. Centers for Disease Prevention and Control in Atlanta.
The biggest uncertainty is how much doctors, nurses, and others can slow the virus. There are many ways of pushing down Re, Farrar says—washing hands, wearing masks, or quarantining people, for example. “But given the complexity of this outbreak and the limited resources, we need to find out what are the two or three things that will most help drive down infections,” Farrar says, and that’s where models can help. For instance, would following up on all the contacts of every case be more effective than following up on the much smaller number who had a certain type of contact with a case, such as sharing a room?
Rivers is evaluating interventions, such as increased use of protective equipment or campaigns to isolate infected people. In the most optimistic scenario, every contact of infected people is traced, and transmission in hospitals is reduced by 75%. Even that, while drastically reducing the number of Ebola deaths, did not push Re below one.
The challenge varies by country, Althaus says. “In Guinea and Sierra Leone, Re is close to 1 and the outbreak could be stopped if interventions improve a bit.” In Liberia, Re has been near 1.5 the whole time. “That means work is only just beginning there.” But Meltzer says there is no reason to believe the situation is any better in Sierra Leone. “We are not seeing any change in the rate of the accumulation of cases,” he says.
As models get better at differentiating what is happening in places, Rivers says, “you might be able to put firelines around certain communities.” But such measures are very controversial. When Liberia last week barricaded off West Point, a sprawling slum with probably more than 100,000 inhabitants, it drew a largely negative response. “Quarantines and curfews tend to instill fear and distrust towards the whole of the outbreak response including health structures,” a representative for Doctors Without Borders told Science. Paul Seabright, a researcher at the Toulouse School of Economics in France who has studied such measures, says they are an incentive for people to keep it secret if they have had contact with a patient. Liberia’s harsh actions are “the last thing this epidemic needs,” he says.
People in West Africa will have to alter behaviors, Meltzer says. “We won’t stop this outbreak solely by building hospitals. There will have to be a change in the way the community deals with the disease.” Modeling that is easy enough, Vespignani says. “I can decrease the transmission at funerals by 40% easily in a model. That’s one line of code. But in the field that is really hard.”
*The Ebola Files: Given the current Ebola outbreak, unprecedented in terms of number of people killed and rapid geographic spread, Science and Science Translational Medicine have made a collection of research and news articles on the viral disease freely available to researchers and the general public.